Adult Patients: The total number of patients treated with ertapenem in clinical studies was over 1900 of which over 1850 received a 1 g dose of INVANZ. Most adverse experiences reported in these clinical studies were described as mild to moderate in severity. Drug-related adverse experiences were reported in approximately 20% of patients treated with ertapenem. Ertapenem was discontinued due to adverse experiences thought to be drug-related in 1.3% of patients.
The most common drug-related adverse experiences reported during parenteral therapy in patients treated with ertapenem were diarrhea (4.3%), infused vein complication (3.9%), nausea (2.9%) and headache (2.1%).
The following drug-related adverse experiences were reported during parenteral therapy in patients treated with ertapenem: see Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In clinical studies, seizure was reported during parenteral therapy in 0.2% of patients treated with ertapenem, 0.3% of patients treated with piperacillin/tazobactam and 0% of patients treated with ceftriaxone.
In the majority of clinical studies, parenteral therapy was followed by a switch to an appropriate oral antimicrobial. During the entire treatment period and a 14 day posttreatment follow-up period, drug-related adverse experiences in patients treated with INVANZ included in the table as previously mentioned as well as rash and vaginitis at an incidence of ≥ 1.0% (common) and allergic reactions, malaise and fungal infections at an incidence of >0.1% but <1.0% (uncommon).
In a clinical study for the treatment of diabetic foot infections in which 289 adult diabetic patients were treated with ertapenem, the drug-related adverse experience profile was generally similar to that seen in previous clinical trials.
In a clinical study for the prophylaxis of surgical site infections following elective colorectal surgery in which 476 adult patients received a 1 g dose of ertapenem prior to surgery, the only drug-related adverse experience during parenteral therapy that was not seen in previous clinical trials was sinus bradycardia reported at an incidence of >0.1% but <1.0% (uncommon).
Pediatric Patients: The total number of pediatric patients treated with ertapenem in clinical studies was 384. The overall safety profile is comparable to that in adult patients. In clinical trials, the most common drug-related clinical adverse experiences reported during parenteral therapy were diarrhea (5.5%), infusion site pain (5.5%) and infusion site erythema (2.6%).
The following drug-related adverse experiences were reported during parenteral therapy in pediatric patients treated with ertapenem: see Table 2.
Click on icon to see table/diagram/image
Additional drug-related adverse experiences that were reported during parenteral therapy in >0.5% but <1.0% of patients treated with INVANZ in clinical studies include: infusion site induration, infusion site pruritus, infusion site warmth and phlebitis.
In the pediatric clinical studies, the majority of the patients had parenteral therapy followed by a switch to an appropriate oral antimicrobial. During the entire treatment period and a 14 day posttreatment follow-up period, drug-related adverse experiences in patients treated with INVANZ were no different than those listed previously.
Post-Marketing Experience: The following post-marketing adverse experiences have been reported:
Immune System: anaphylaxis including anaphylactoid reactions.
Psychiatric Disorders: altered mental status (including agitation, aggression, delirium, disorientation, mental status changes).
Nervous System Disorders: dyskinesia, depressed level of consciousness, gait disturbance, hallucinations, myoclonus, tremor.
Gastrointestinal Disorders: teeth staining.
Skin and Subcutaneous Tissue Disorders: Acute Generalized Exanthematous Pustulosis (AGEP), Drug Rash with Eosinophilia and Systemic Symptoms (DRESS syndrome), urticaria.
Musculoskeletal and Connective Tissue Disorders: muscular weakness.
Laboratory Test Findings: Adult Patients: The most frequently observed drug-related laboratory abnormalities during parenteral therapy in patients receiving INVANZ were elevations in ALT, AST, alkaline phosphatase and platelet count.
In the majority of clinical studies, parenteral therapy was followed by a switch to an appropriate oral antimicrobial. During the entire treatment period and a 14 day posttreatment follow-up period, drug-related laboratory abnormalities in patients treated with INVANZ were no different than those listed previously.
Other drug-related laboratory abnormalities included the following: Increases in direct serum bilirubin, total serum bilirubin, eosinophils, indirect serum bilirubin, PTT, urine bacteria, BUN, serum creatinine, serum glucose, monocytes, urine epithelial cells, urine red blood cells; decreases in segmented neutrophils, white blood cells, hematocrit, hemoglobin and platelet count.
In a clinical study for the treatment of diabetic foot infections in which 289 adult diabetic patients were treated with ertapenem, the drug-related laboratory adverse experience profile was generally similar to that seen in previous clinical trials.
In a clinical study for the prophylaxis of surgical site infections following elective colorectal surgery in which 476 adult patients received a 1 g dose of ertapenem prior to surgery, there were no additional drug related laboratory adverse experiences reported during parenteral therapy.
Pediatric Patients: The most frequently observed drug-related laboratory abnormality during parenteral therapy in patients receiving INVANZ was decreases in neutrophil count.
Other drug-related laboratory abnormalities during the entire treatment period plus 14-day follow-up included the following: Elevations in ALT, elevations in AST, decreases in white blood cells, and increases in eosinophils.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image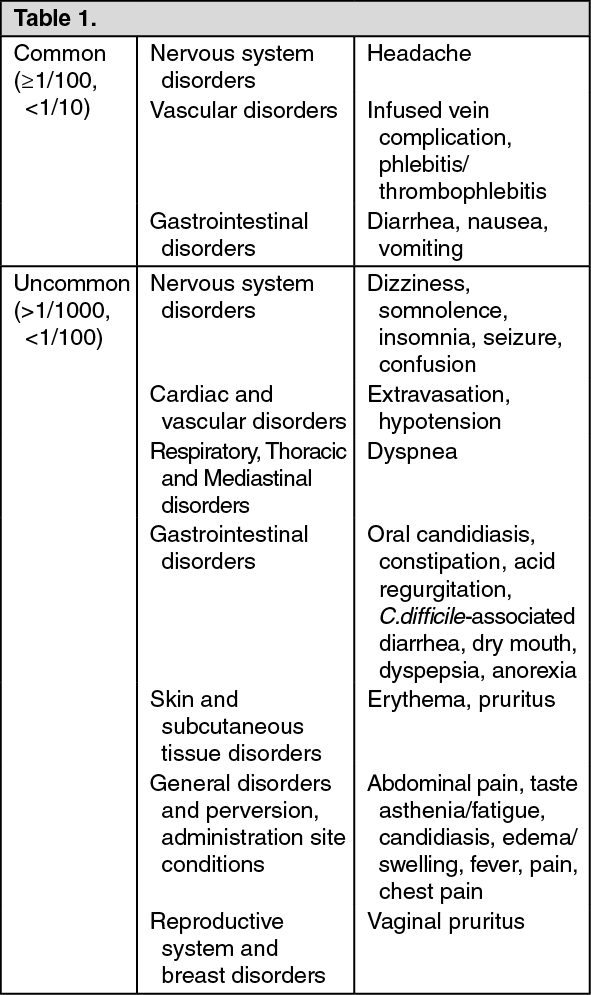 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image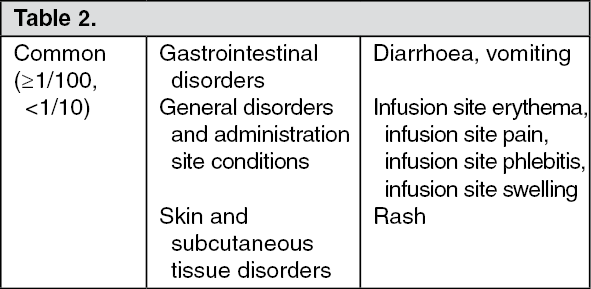 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
