Fimasartan 60 mg contains 66.01 mg of fimasartan potassium trihydrate (or 60 mg as fimasartan potassium).
Fimasartan 120 mg contains 132.02 mg of fimasartan potassium trihydrate (or 120 mg as fimasartan potassium).
Pharmacology: Pharmacodynamics: During an in vitro study, fimasartan was found to bind selectively to AT1, which was also demonstrated in non-clinical studies. These findings was also confirmed in phase I and phase IIa clinical studies where ARB-specific changes, such as elevation of plasma renin activity (PRA), increased AI and AII concentrations were identified.
In addition, it has been well established from the results of phase II and III clinical studies that this mechanism of action is associated with the blood pressure lowering effect.
Pharmacokinetics: Absorption: Time to peak plasma concentration (Tmax) following single oral administration of fimasartan at doses of 20-480 mg in healthy subjects ranged 0.5-3 hours with the terminal half-life (t1/2) being 5-16 hours. Similar results were obtained in patients with hypertension, i.e., Tmax ranged 0.5-1.3 hours and t1/2 were 7-10 hours following fimasartan administration at doses 20-180 mg. Several subjects showed a second peak, and the total systemic exposure as assessed by the area under the concentration-time curve was linear (i.e., dose-independent). Accumulation index was 1.20-1.26 and 1.02-1.08 for healthy subjects and patients, respectively. The absolute bioavailability of fimasartan in healthy subjects following 60 mg oral administration compared to 30 mg intravenous infusion was estimated to be 19%.
These results support the notion that oral fimasartan is rapidly absorbed, have linear pharmacokinetic profiles over 20-480 mg doses, and accumulation is minimal when dosed once daily. Therefore, the total systemic exposure can be easily predicted for each dose, which helps increase certainty about the safe and effective use of fimasartan in a clinical setting.
Distribution and Protein Binding: In vitro protein binding in human plasma ranged 95.6-97.2% at fimasartan concentrations of 0.01-100 μg/mL, which was not dose-dependent. These results were similar to those obtained in the dog and rat using the in vitro and ex vivo methods.
Metabolism: In vitro study showed CYP3A4 would be mainly involved in fimasartan metabolism. Fimasartan has not been shown to inhibit or induce other CYP enzymes. The parent drug was ≥85% of the fimasartan moieties found in human plasma with a few metabolites identified, which supports the notion that the pharmacological action of fimasartan is mainly driven by the parent drug. The most abundant circulating metabolites of fimasartan in plasma in healthy male subjects were identified as desulfo-fimasartan and fimasartan-S-oxide. These metabolites accounted for approximately 14% (each 7%) of the total drug related exposure. No parent or metabolite has been assayed in human faeces; however, in vivo metabolism of fimasartan is most likely to be minimal given the systemic exposure level of fimasartan was weakly increased by specific CYP3A4 inhibitors. These favorable pharmacokinetic properties of fimasartan enable its safe use in a clinical setting.
Elimination: Less than 3% of the fimasartan dose was recovered in urine over 24 hours post dose following oral administration in healthy male subjects and patients with hypertension. Therefore, the kidney is unlikely involved in the elimination of fimasartan.
Food Effect: A preliminary exploration was made in a phase I study conducted in the UK for food effect on the pharmacokinetics of fimasartan, and no food effect was noted. A formal food effect study was performed in South Korea, in which the point estimates for the geometric mean ratios of AUC0-∞ and Cmax with and without food were 0.6371 and 0.3481, respectively, suggesting food affects fimasartan's absorption. However, given the exposure-response relationship of fimasartan in reducing blood pressure has been well established and is relatively flat over the therapeutically recommended doses of 60-120 mg, and it took 2-4 weeks to take on drug effect, the observed food effect on the pharmacokinetics of fimasartan is considered insignificant large enough to justify dosage adjustment with food.
Pharmacokinetic Characteristics in special populations: Elderly Subjects: Elderly subjects (i.e., aged ≥65 years old) had a 1.69 times greater systemic exposure than young adults. However, since the renin-angiotensin system (RAS) activity in the elderly is generally lower than young adults, increased systemic exposure will be less likely to result in greater blood pressure reduction. This assumption has been frequently affirmed in other angiotensin receptor blockers. In fact, the blood pressure reduction in elderly subjects enrolled in therapeutic fimasartan clinical trials was numerically smaller than the one seen in those <65 years old. In addition, no difference in the safety profiles was noted between elderly and young subjects. These results collectively support the notion that increased systemic exposure in elderly subjects has less clinical significance, and does not require any dosage adjustment in this population.
Drug Interaction: Pharmacokinetic drug interaction potential for fimasartan was investigated using drugs that may be concomitantly used with fimasartan in diverse clinical settings. Antihypertensive drugs such as hydrochlorothiazide and amlodipine did not show a significant pharmacokinetic interaction with fimasartan. Therefore, fimasartan can be safely co-administered with hydrochlorothiazide and amlodipine without dosage adjustment to achieve further blood pressure reduction in those who do not respond well enough to these antihypertensive medications alone.
Likewise, atorvastatin, digoxin and warfarin, which are frequently used in patients with hypertension, showed no clinically significant pharmacokinetic drug interaction with fimasartan, enabling safe concomitant use without dosage adjustment.
Ketoconazole, a CYP3A4 inhibitor, increased fimasartan's systemic exposure by 2 folds, which is considered weak drug interaction. This magnitude of drug interaction does not require any dosage adjustment for concomitant use, but close monitoring of patients may be recommended. In addition, rifampicin, a strong OATP1B1 inhibitor, increased fimasartan's systemic exposure by 4.6 folds as assessed using AUC. Since OATP1B1 is known to play a significant role in fimasartan's transport into hepatic cells and rifampicin also induces CYP3A4, co-administration of rifampicin with fimasartan is not recommended. Based on these results, fimasartan can be safely co-administered with most drugs in patients with hypertension.
Population Pharmacokinetics: A formal population pharmacokinetic-pharmacodynamic modeling analysis was performed using data obtained from two phase I studies (healthy subjects), conducted in UK, and an early phase II study (patients with mild to moderate hypertension), conducted in South Korea. In addition, a back-of-the-envelope type of population pharmacokinetic analysis was performed using concentrations collected in the ABPM study. Population pharmacokinetic parameters derived from the formal population pharmacokinetic-pharmacodynamic analysis was similar to those estimated using the non-compartment analysis approach. Fimasartan's population pharmacokinetic parameters were not significantly affected by race, sex, or glomerular filtration rate (GFR). Instead, body weight, bilirubin and age were significant covariates. Given that the between-subject variability (BSV) on the fimasartan concentration yielding 50% of the maximal blood pressure reduction (i.e., EC50) was large (i.e., 130-140%), those significant covariates on pharmacokinetic parameters are less likely to affect the extent of blood pressure reduction by fimasartan. Therefore, no dosage adjustment for fimasartan is warranted based on covariates. Similar findings were obtained in the back-of-the-envelope population pharmacokinetic analysis, i.e., height was identified as a significant covariate, but no dosage adjustment based on height is required.
These results support the notion that dosage adjustment for fimasartan based on individual's extrinsic and intrinsic factors is not required to treat patients with hypertension. Rather, dosage adjustment based on treatment response (i.e., blood pressure reduction) will be more practical in a clinical setting.
Kanarb Tablets (Fimasartan Potassium Trihydrate) is indicated for the treatment of essential hypertension.
Adult Hypertension: The recommended initial dose of Kanarb Tablets is 60 mg once daily with or without food. If blood pressure is not adequately controlled at 60 mg, the dosage of Kanarb Tablets may be increased to 120 mg once daily. Whenever possible, it is recommended that Kanarb Tablets be taken at the same time during the day (e.g., morning).
The blood pressure lowering effect of Kanarb Tablets is substantially present within 2 weeks, and maximal reduction is generally attained after 8 to 12 weeks of treatment.
Geriatric Use: No initial dosage adjustment is required for elderly patients (age ≤70 years).
Renal Impairment: No initial dosage adjustment is required for patients with mild to moderate renal impairment (creatinine clearance 30 ‒ 80 mL/min). For severe renal impairment (creatinine clearance < 30 mL/min), the recommended initial dose is 30 mg once daily and the dose should not exceed 60 mg.
Hepatic Impairment: No initial dosage adjustment is required for patients with mild hepatic impairment. Kanarb Tablets is not recommended to patients with moderate to severe hepatic impairment.
Pediatric Use: The efficacy and safety of Kanarb Tablets has not been established in patients 18 years or younger.
Intravascular Volume-Depleted Patients (e.g., Patients receiving high doses of diuretics): For patients whose intravascular volume is depleted, at risk for symptomatic hypotension, the initial dose of 30 mg once daily is recommended.
Mode/Route of Administration: To be taken orally.
No data are available about overdosage of Kanarb Tablets in humans. The most likely manifestations of overdosage would be hypotension and tachycardia; bradycardia could occur from parasympathetic (vagal) stimulation. If symptomatic hypotension should occur, supportive treatment should be provided. It is not known whether Kanarb Tablets is removed from the plasma by hemodialysis.
Kanarb Tablets is contraindicated in the following patients: Patients who are hypersensitive to any component of this product.
Pregnant or nursing mothers (see Use in Pregnancy & Lactation).
Hemodialysis Patients (no experience in this population).
Patients with moderate to severe hepatic impairment.
Patients with hepatobiliary obstruction.
Patients with diabetes or renal impairment (GFR <60 mL/min) who are taking aliskiren (see Interactions).
Patients with diabetic nephropathy who are taking angiotensin converting enzyme (ACE) inhibitors (see Interactions).
Patients with genetic disorders such as galactose intolerance, Lapp lactose deficiency, or glucose-galactose malabsorption (since Kanarb Tablets contains lactose).
Drugs directly acting on the renin angiotensin system may cause injury or death to the developing fetus when administered to a pregnant woman during the second and third trimesters. Therefore, Kanarb Tablets should be discontinued when pregnancy is detected in female patients (see Use in Pregnancy & Lactation).
Patients requiring close monitoring during Kanarb Tablets treatment: Intravascular volume- or salt-depletion: These patients (e.g., patients receiving high doses of diuretics), whose renin angiotensin system is activated, may experience symptomatic hypotension at the time of initial Kanarb administration or its dosage increase. Therefore, close monitoring is required in these patients.
Renal impairment: Patients who are sensitive to drugs inhibiting the rennin angiotensin system may experience changes in the renal function. Angiotensin converting enzyme inhibitors or angiotensin II receptor antagonists may cause oliguria, progressive hyperuremia, and rarely acute renal failure or death to patients whose renal function is dependent on the activity of the renin-angiotensin-aldosterone system (e.g., patients with severe congestive heart failure).
Renovascular hypertension: Patients with uni-lateral or bi-lateral renal artery stenosis may have an increased risk for severe hypotension or renal failure when drugs affecting the rennin angiotensin system are administered.
Special caution is required for patients with aortic or mitral valve stenosis, obstructive or hypertrophic cardiac myopathy like other vasodilators.
Patients with primary aldosteronism generally do not respond to the drugs that inhibit the renin-angiotensin system, therefore Kanarb is not recommended in this population.
Allergy or hypersensitivity to Sunset Yellow FCF: Caution is required for patients who have an allergy or are hypersensitive to Sunset Yellow FCF (Food Yellow No.5).
Hepatic Impairment Use: The pharmacokinetics of fimasartan was compared in patients with mild and moderate hepatic impairment to healthy volunteers. A 20% decrease in AUC and 10% increase in Cmax were observed in patients with mild hepatic impairment. The AUC and Cmax in moderate hepatic impairment were increased by 6.5-fold and 5-fold, respectively. Kanarb is not recommended to moderate to severe hepatic impairment.
Effects on the Ability to Drive or Operate Machines: The effects of Kanarb Tablets on driving and the operation of machinery have not been studied. However, drowsiness and dizziness may occur sometimes with blood pressure-lowering agents, therefore patients taking Kanarb Tablets should be warned about these risks when driving or operating machinery is anticipated.
Use in Children: Safety and effectiveness in pediatric patients (age ≤18 years) have not been established.
Use in the Elderly: Kanarb has not been administered to elderly patients more than 70 years old. In a study to compare the pharmacokinetics of elderly healthy volunteers aged 65 years or more and young, healthy volunteers, the AUC of Kanarb in the elderly group increased by 69%. However, no differences in the efficacy and safety were noted in a total of 21 elderly patients (≥65 years, 9.3%), out of 226 patients receiving Kanarb in Phase 3 clinical trials, between the elderly and non-elderly populations. Therefore, no dosage adjustment with Kanarb is necessary in elderly patients (≤70 years), although greater sensitivity of some older individuals cannot be ruled out.
Pregnancy: Drugs that act directly on the renin-angiotensin system can cause foetal and neonatal morbidity and death when administered to pregnant women. The use of drugs that act directly on the renin-angiotensin system during the second and third trimesters of pregnancy has been associated with foetal and neonatal injury, including hypotension, neonatal skull hypoplasia, anuria, reversible or irreversible renal failure, and death. Oligohydramnios has also been reported, presumably resulting from decreased foetal renal function; oligohydramnios in this setting has been associated with foetal limb contractures, craniofacial deformation, and hypoplastic lung development. Prematurity, intrauterine growth retardation and patent ductus arteriosus have also been reported, although it is not clear whether these occurrences were due to exposure to the drug. When pregnancy is detected, Kanarb Tablets should be discontinued as soon as possible. These adverse effects do not appear to have resulted from intrauterine drug exposure that has been limited to the first trimester. Mothers whose embryos and foetuses are exposed to an angiotensin II receptor antagonist only during the first trimester should be so informed. Nonetheless, when patient become pregnant, physicians should advise the patient to discontinue the use of Kanarb Tablets as soon as possible. Infants with histories of in utero exposure to an angiotensin II receptor antagonist should be closely observed for hypotension, oliguria, and hyperkalemia.
Breast-feeding: It is not known whether Kanarb Tablets is excreted in human milk, but Kanarb Tablets was excreted in the milk of lactating rats; therefore, it is not recommended to administer Kanarb Tablets to nursing mothers. A decision should be made whether to discontinue nursing or discontinue Kanarb Tablets, taking into account the importance of the drug to the mother.
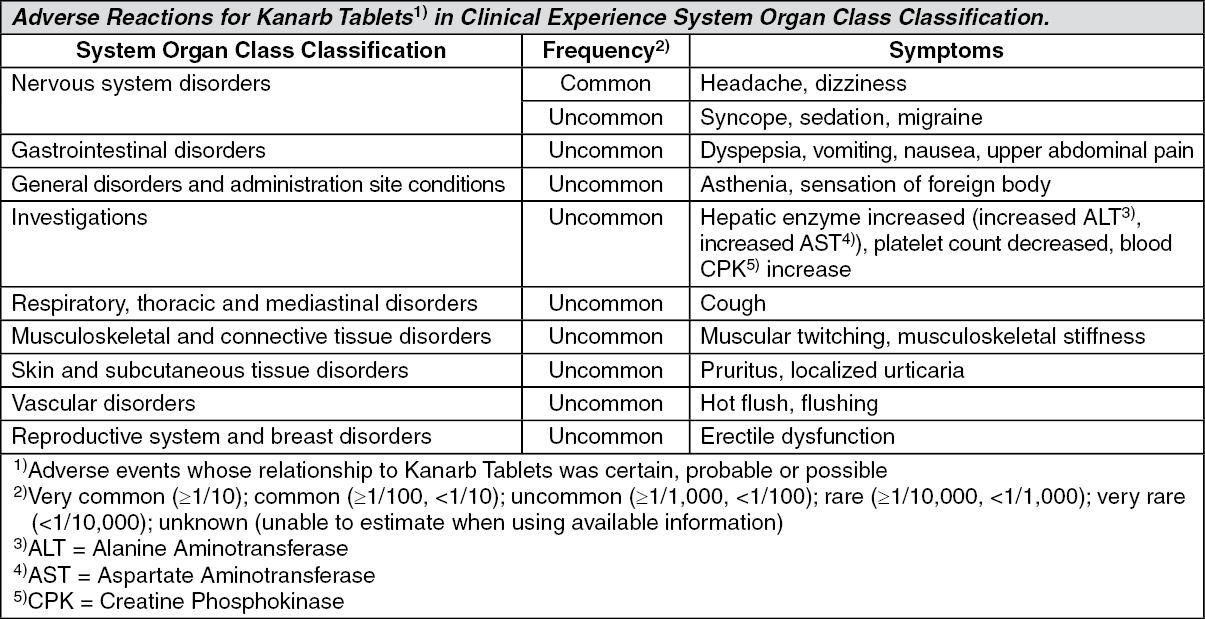
The safety of Kanarb Tablets was evaluated in 406 patients, who had received Kanarb Tablets at the dose range of 60 to 120 mg for 4 to 12 weeks, out of a total of 852 patients with essential hypertension, enrolled in clinical trials and eligible for safety analysis (i.e., the safety database). There were 85 patients that received Kanarb Tablets for 6 months or longer. Most adverse events were mild to moderate, transient, and the occurrence rate was not related to dosage. The most frequently reported adverse events were headache and dizziness. Adverse reactions are summarized below (i.e., adverse events considered to be definitely related, probably related, or possibly related to Kanarb Tablets), reported in the clinical trials of Kanarb Tablets. (See Table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Potassium supplements and potassium-sparing diuretics: Serum potassium can be increased by Kanarb Tablets and other drugs that exert effects on the renin-angiotensin system when co-administered with potassium-sparing diuretics (e.g., spironolactone), potassium supplements, salt alternatives containing potassium, and drugs that may increase serum potassium (e.g., heparin).
The blood pressure-lowering effect of Kanarb Tablets can be increased when co-administered with other antihypertensive agents, including diuretics. When high doses of diuretics were used previously, leading to a volume-depleted state, excessive blood pressure reduction may occur with the initiation of Kanarb Tablets treatment.
Lithium: Reversible increases in serum lithium levels and toxicities have been reported when lithium was used with angiotensin converting enzyme inhibitors whereas those reactions have been very rarely reported in case that angiotensin II receptor antagonist were co-administered with lithium. Although co-administration of lithium with Kanarb Tablets is not generally recommended, should it be necessary, close monitoring of lithium levels is required.
Non-steroidal anti-inflammatory drugs (NSAIDs): When an NSAID (e.g., aspirin, COX-2 inhibitors) is co-administered, the blood pressure-lowering effect of an angiotensin II receptor antagonist may be reduced. Deterioration of damaged renal function (including acute renal failure, although reversible,) has been reported when an angiotensin II receptor antagonist is co-administered with a COX inhibitor in some patients with renal impairment (e.g., dehydrated patients and renally impaired elderly patients). Therefore, caution needs to be exercised when co-administering Kanarb Tablets with NSAIDs, especially in elderly patients. Adequate hydration is required in this case, and the renal function should be closely monitored.
Hydrochlorothiazide: No significant pharmacokinetic drug interaction between Kanarb Tablets and hydrochlorothiazide was found when co-administered.
Amlodipine: No significant pharmacokinetic drug interaction between Kanarb Tablets and amlodipine was found when co-administered.
Dual blockade of the RAS with angiotensin receptor blockers, ACE inhibitors, or aliskiren is associated with increased risks of hypotension, syncope, hyperkalemia, and changes in renal function (including acute renal failure) compared to monotherapy. In general, avoid combined use of RAS inhibitors. Do not co-administer aliskiren with Kanarb Tablets in patients with diabetes or renal impairment (GFR <60 mL/min). Co-administer ACE inhibitor with Kanarb Tablets is not recommended and avoids use of ACE inhibitor with Kanarb Tablets in patients with diabetic nephropathy.
The effects of other drugs on Kanarb Tablets: Ketoconazole: The systemic exposure of Kanarb Tablets, as measured by the area under the concentration-time curve (AUC), was increased approximately by two times when co-administered with ketoconazole. Caution needs to be exercised when Kanarb Tablets is co-administered with ketoconazole.
Rifampicin or other OATP1B1 transporter inhibitors: Kanarb Tablets is a substrate of OAT1 and OATP1B1. When Kanarb Tablets is co-administered with rifampicin (OATP1B1 inhibitor), the AUC of Kanarb Tablets was increased approximately by 4.6-fold. Therefore, co-administration of Kanarb Tablets with rifampicin is not recommended. When co-administered with other OATP1B1 transporter inhibitors (e.g., cyclosporine), the systemic exposure of Kanarb Tablets may increase, and caution is required.
The effects of Kanarb Tablets on other drugs: Warfarin: The pharmacokinetics and pharmacodynamics of warfarin were not significantly affected by co-administered Kanarb Tablets.
Atorvastatin: The AUC's of atorvastatin and its active metabolite were not affected by co-administered Kanarb Tablets. Maximum plasma concentrations (Cmax) of atorvastatin and its active metabolite were increased by 1.9-fold and 2.5-fold, respectively.
Digoxin: The pharmacokinetics and creatinine clearance of digoxin was not affected by co-administered Kanarb Tablets. Cmax of digoxin was increase by 30%. Close monitoring of digoxin level may be required when co-administered with Kanarb Tablets.
Other drug interactions: Kanarb Tablets does not inhibit or induce the CYP450 enzymes.
Incompatibilities: Not applicable.
Kanarb Tablets should be in tightly closed container. It is recommended that Kanarb Tablets should be stored at room temperature (do not store above 30℃) in a light-protected container.
Kanarb Tablets should be stored in a place a child cannot reach.
Repackaging of Kanarb is not recommended because it may cause some accidental mislabeling or adversely affect the product quality.
C09CA10 - fimasartan ; Belongs to the class of angiotensin II receptor blockers (ARBs). Used in the treatment of cardiovascular disease.
Kanarb FC tab 120 mg
3 × 10's
Kanarb FC tab 60 mg
3 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out
