Pharmacotherapeutic group: Antiviral for systemic use; antivirals for treatment of HIV infections, combinations.
ATC code: Not yet assigned.
Namibia Pharmacological Classification: 20.2.8 Antiviral agents.
Pharmacology: Pharmacodynamics: Mechanism of action: Dolutegravir inhibits HIV integrase by binding to the integrase active site and blocking the strand transfer step of retroviral Deoxyribonucleic acid (DNA) integration which is essential for the HIV replication cycle.
Emtricitabine is a nucleoside reverse transcriptase inhibitor (NRTI) and nucleoside analogue of 2'-deoxycytidine. Emtricitabine is phosphorylated by cellular enzymes to form emtricitabine triphosphate. Emtricitabine triphosphate inhibits HIV replication through incorporation into viral DNA by the HIV reverse transcriptase (RT), which results in DNA chain-termination. Emtricitabine has activity against HIV-1, HIV-2, and HBV.
Tenofovir alafenamide is a nucleotide reverse transcriptase inhibitor (NtRTI) and phosphonoamidate prodrug of tenofovir (2'-deoxyadenosine monophosphate analogue). Tenofovir alafenamide is permeable into cells and due to increased plasma stability and intracellular activation through hydrolysis by cathepsin A, tenofovir alafenamide is more efficient than tenofovir disoproxil fumarate in concentrating tenofovir in peripheral blood mononuclear cells (PBMCs) or HIV target cells including lymphocytes and macrophages. Intracellular tenofovir is subsequently phosphorylated to the pharmacologically active metabolite tenofovir diphosphate. Tenofovir diphosphate inhibits HIV replication through incorporation into viral DNA by the HIV RT, which results in DNA chain-termination.
Tenofovir has activity against HIV-1, HIV-2, and HBV.
Pharmacodynamic effects: Antiviral activity
in vitro: The IC
50 for dolutegravir in various labstrains using PBMC was 0.5 nM, and when using MT-4 cells it ranged from 0.7-2 nM. Similar IC
50s were seen for clinical isolates without any major difference between subtypes; in a panel of 24 HIV-1 isolates of clades A, B, C, D, E, F and G and group O the mean IC
50 value was 0.2 nM (range 0.02-2.14). The mean IC
50 for 3 HIV-2 isolates was 0.18 nM (range 0.09-0.61).
In 100%
human serum, the mean protein fold shift was 75 fold, resulting in protein adjusted IC
90 of 0.064 ug/mL.
No antagonistic effects
in vitro were seen with dolutegravir and other antiretrovirals tested: stavudine, abacavir, efavirenz, nevirapine, lopinavir, amprenavir, enfuvirtide, maraviroc and raltegravir. In addition, no antagonistic effects were seen for dolutegravir and adefovir, and ribavirin had no apparent effect on dolutegravir activity.
Emtricitabine and tenofovir alafenamide demonstrated synergistic antiviral activity in cell culture. No antagonism was observed with emtricitabine or tenofovir alafenamide when combined with other antiretroviral agents.
The antiviral activity of emtricitabine against laboratory and clinical isolates of HIV-1 was assessed in lymphoblastoid cell lines, the MAGI CCR5 cell line, and PBMCs. The 50% effective concentration (EC
50) values for emtricitabine were in the range of 0.0013 to 0.64 μM. Emtricitabine displayed antiviral activity in cell culture against HIV-1 clades A, B, C, D, E, F, and G (EC
50 values ranged from 0.007 to 0.075 μM) and showed strain specific activity against HIV-2 (EC
50 values ranged from 0.007 to 1.5 μM).
The antiviral activity of tenofovir alafenamide against laboratory and clinical isolates of HIV-1 subtype B was assessed in lymphoblastoid cell lines, PBMCs, primary monocyte/macrophage cells and CD4+ T-lymphocytes. The EC
50 values for tenofovir alafenamide were in the range of 2.0 to 14.7 nM. Tenofovir alafenamide displayed antiviral activity in cell culture against all HIV-1 groups (M, N, and O), including subtypes A, B, C, D, E, F, and G (EC
50 values ranged from 0.10 to 12.0 nM) and showed strain specific activity against HIV-2 (EC
50 values ranged from 0.91 to 2.63 nM).
Resistance:
In vitro: Dolutegravir: Serial passage is used to study resistance evolution
in vitro. When using the lab-strain HIV-1 IIIB during passage over 112 days, mutations selected appeared slowly, with substitutions at positions S153Y and F, resulting in a maximal fold change in susceptibility of 4 (range 2-4). These mutations were not selected in patients treated with dolutegravir in the clinical studies. Using strain NL432, mutations E92Q (FC 3) and G193E (also FC 3) were selected. The E92Q mutation has been selected in patients with pre-existing raltegravir resistance who were then treated with dolutegravir (listed as a secondary mutation for dolutegravir).
In further selection experiments using clinical isolates of subtype B, mutation R263K was seen in all five isolates (after 20 weeks and onwards). In subtype C (n=2) and A/G (n=2) isolates the integrase substitution R263K was selected in one isolate, and G118R in two isolates. R263K was reported from two ART experienced, INI naive individual patients with subtypes B and C in the clinical program, but without effects on dolutegravir susceptibility
in vitro. G118R lowers the susceptibility to dolutegravir in site directed mutants (FC 10), but was not detected in patients receiving dolutegravir in the Phase III program.
Primary mutations for raltegravir/elvitegravir (Q148H/R/K, N155H, Y143R/H/C, E92Q and T66I) do not affect the
in vitro susceptibility of dolutegravir as single mutations. When mutations listed as secondary integrase inhibitor associated mutations (for raltegravir/elvitegravir) are added to these primary mutations in experiments with site directed mutants, dolutegravir susceptibility is still unchanged (FC <2 vs wild type virus), except in the case of Q148-mutations, where a FC of 5-10 or higher is seen with combinations of certain secondary mutations. The effect by the Q148-mutations (H/R/K) was also verified in passage experiments with site directed mutants. In serial passage with strain NL432, starting with site directed mutants harbouring N155H or E92Q, no further selection of resistance was seen (FC unchanged around 1).
In contrast, starting with mutants harbouring mutation Q148H (FC 1), a variety of secondary mutations were seen with a consequent increase of FC to values >10.
A clinically relevant phenotypic cut-off value (FC vs wild type virus) has not been determined; genotypic resistance was a better predictor for outcome.
Seven hundred and five raltegravir resistant isolates from raltegravir experienced patients were analyzed for susceptibility to dolutegravir. Dolutegravir has a less than or equal to 10 FC against 94% of the 705 clinical isolates.
Emtricitabine: Reduced susceptibility to emtricitabine is associated with M184V/I mutations in HIV-1 RT.
Tenofovir Alafenamide: HIV-1 isolates with reduced susceptibility to tenofovir alafenamide express a K65R mutation in HIV-1 RT; in addition, a K70E mutation in HIV-1 RT has been transiently observed.
In vivo: Dolutegravir: In previously untreated patients receiving dolutegravir + 2 NRTIs in Phase-IIb and Phase-III, no development of resistance to the integrase class, or to the NRTI class was seen (n=1118 follow-up of 48-96 weeks).
In patients with prior failed therapies, but naïve to the integrase class (SAILING study), integrase inhibitor substitutions were observed in 4/354 patients (follow-up 48 weeks) treated with dolutegravir, which was given in combination with an investigator selected background regimen (BR). Of these four, two subjects had a unique R263K integrase substitution, with a maximum FC of 1.93, one subject had a polymorphic V151V/I integrase substitution, with maximum FC of 0.92, and one subject had pre-existing integrase mutations and is assumed to have been integrase experienced or infected with integrase resistant virus by transmission. The R263K mutation was also selected
in vitro (see previous text).
In the presence of integrase class-resistance (VIKING-3 study) the following mutations were selected in 32 patients with protocol defined virological failure (PDVF) through Week 24 and with paired genotypes (all treated with dolutegravir 50 mg twice daily + optimized background agents): L74L/M (n=1), E92Q (n=2), T97A (n=9), E138K/A/T (n=8), G140S (n=2), Y143H (n=1), S147G (n=1), Q148H/K/R (n=4), and N155H (n=1) and E157E/Q (n=1). Treatment emergent integrase resistance typically appeared in patients with a history of the Q148-mutation (baseline or historic). Five further subjects experienced PDVF between weeks 24 and 48, and 2 of these 5 had treatment emergent mutations. Treatment-emergent mutations or mixtures of mutations observed were L74I (n=1), N155H (n=2).
The VIKING-4 study examined dolutegravir (plus optimized background therapy) in subjects with primary genotypic resistance to INIs at Screening in 30 subjects. Treatment-emergent mutations observed were consistent with those observed in the VIKING-3 study.
Effects on electrocardiogram: No relevant effects were seen on the QTc interval, with doses exceeding the clinical dose by approximately three fold.
Clinical efficacy and safety: Previously untreated patients: The efficacy of dolutegravir in HIV-infected, therapy naïve subjects is based on the analyses of 96-week data from two randomized, international, double-blind, active-controlled trials, SPRING-2 (ING113086) and SINGLE (ING114467). This is supported by 96-week data from an open-label, randomized and active-controlled study FLAMINGO (ING114915) and additional data from the open-label phase of SINGLE to 144 weeks.
In SPRING-2, 822 adults were randomized and received at least one dose of either dolutegravir 50 mg once daily or raltegravir (RAL) 400 mg twice daily, both administered with either ABC/3TC or TDF/FTC. At baseline, median patient age was 36 years, 14% were female, 15% non-white, 11% had hepatitis B and/or C co-infection and 2% were CDC Class C, these characteristics were similar between treatment groups.
In SINGLE, 833 subjects were randomized and received at least one dose of either dolutegravir 50 mg once daily with fixed-dose abacavir-lamivudine (DTG + ABC/3TC) or fixed-dose efavirenz-tenofovir-emtricitabine (EFV/TDF/FTC). At baseline, median patient age was 35 years, 16% were female, 32% nonwhite, 7% had hepatitis C co-infection and 4% were CDC Class C, these characteristics were similar between treatment groups.
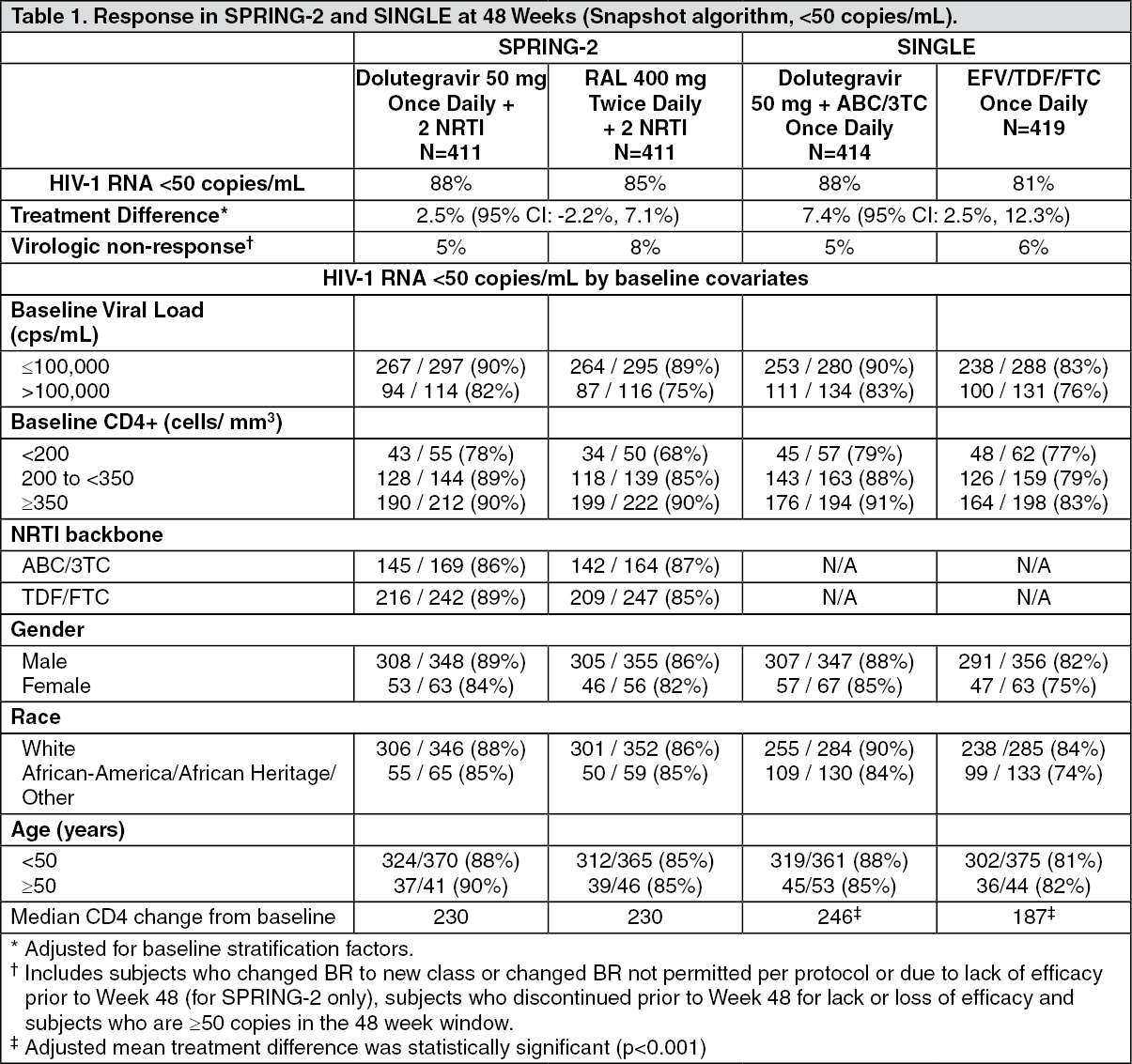
The primary endpoint and other week 48 outcomes (including outcomes by key baseline covariates) for SPRING-2 and SINGLE are shown in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
At week 48, dolutegravir was non-inferior to raltegravir in the SPRING-2 study, and in the SINGLE study dolutegravir + ABC/3TC was superior to efavirenz/TDF/FTC (p=0.003), Table 1 as previously mentioned. In SINGLE, the median time to viral suppression was shorter in the dolutegravir treated patients (28 vs 84 days, (p<0.0001, analysis pre-specified and adjusted for multiplicity).
At week 96, results were consistent with those seen at week 48. In SPRING-2, dolutegravir was still non-inferior to raltegravir (viral suppression in 81% vs 76% of patients), and with a median change in CD4 count of 276 vs 264 cells/mm
3, respectively. In SINGLE, dolutegravir + ABC/3TC was still superior to EFV/TDF/FTC (viral suppression in 80% vs 72%, treatment difference 8.0% (2.3, 13.8), p=0.006, and with an adjusted mean change in CD4 count of 325 vs 281 cells/mm
3, respectively. At 144 weeks in the open-label phase of SINGLE, virologic suppression was maintained, the dolutegravir + ABC/3TC arm (71%) was superior to the EFV/TDF/FTC arm (63%), treatment difference was 8.3% (2.0, 14.6).
In FLAMINGO (ING114915), an open-label, randomised and active-controlled study, 484 HIV-1 infected antiretroviral naïve adults received one dose of either dolutegravir 50 mg once daily (n=242) or darunavir/ritonavir (DRV/r) 800 mg/100 mg once daily (n=242), both administered with either ABC/3TC or TDF/FTC. At baseline, median patient age was 34 years, 15% were female, 28% non-white, 10% had hepatitis B and/or C co-infection, and 3% were CDC Class C; these characteristics were similar between treatment groups. Virologic suppression (HIV-1 RNA <50 copies/mL) in the dolutegravir group (90%) was superior to the DRV/r group (83%) at 48 weeks. The adjusted difference in proportion and 95% CI were 7.1% (0.9, 13.2), p=0.025. At 96 weeks, virologic suppression in the dolutegravir group (80%) was superior to the DRV/r group (68%), (adjusted treatment difference [DTG-(DRV+RTV)]: 12.4%; 95% CI: [4.7, 20.2].
Treatment emergent resistance in previously untreated patients failing therapy: Through 96 weeks in SPRING-2 and FLAMINGO and 144 weeks in SINGLE, no cases of treatment emergent primary resistance to the integrase- or NRTI-class were seen in the dolutegravir-containing arms. For the comparator arms, the same lack of treatment emergent resistance was also the case for patients treated with darunavir/r in FLAMINGO. In SPRING-2, four patients in the RAL-arm failed with major NRTI mutations and one with raltegravir resistance; in SINGLE, six patients in the EFV/TDF/FTC-arm failed with mutations associated with NNRTI resistance, and one developed a major NRTI mutation.
Patients with prior treatment failure, but not exposed to the integrase class: In the international multicentre, double-blind SAILING study (ING111762), 719 HIV-1 infected, antiretroviral therapy (ART)-experienced adults were randomized and received either dolutegravir 50 mg once daily or raltegravir 400 mg twice daily with investigator selected background regimen consisting of up to 2 agents (including at least one fully active agent). At baseline, median patient age was 43 years, 32% were female, 50% non-white, 16% had hepatitis B and/or C co-infection, and 46% were CDC Class C. All patients had at least two class ART resistance, and 49% of subjects had at least 3-class ART resistance at baseline.
Week 48 outcomes (including outcomes by key baseline covariates) for SAILING are shown in Table 2. (See Table 2.)
Click on icon to see table/diagram/image
In the SAILING study, virologic suppression (HIV-1 RNA <50 copies/mL) in the Dolutegravir arm (71%) was statistically superior to the raltegravir arm (64%), at Week 48 (p=0.03).
Statistically fewer subjects failed therapy with treatment-emergent integrase resistance on Dolutegravir (4/354, 1%) than on raltegravir (17/361, 5%) (p=0.003) (Refer to Resistance:
in vivo as previously mentioned for details).
Patients with prior treatment failure that included an integrase inhibitor (and integrase class resistance): In the multicentre, open-label, single arm VIKING-3 study (ING112574), HIV-1 infected, ART experienced adults with virological failure and current or historical evidence of raltegravir and/or elvitegravir resistance received Dolutegravir 50 mg twice daily with the current failing background regimen for 7 days but with optimised background ART from Day 8. The study enrolled 183 patients, 133 with INI-resistance at Screening and 50 with only historical evidence of resistance (and not at Screening). Raltegravir/elvitegravir was part of the current failing regimen in 98/183 patients (part of prior failing therapies in the others). At baseline, median patient age was 48 years, 23% were female, 29% non-white, and 20% had hepatitis B and/or C co-infection. Median baseline CD4+ was 140 cells/mm
3, median duration of prior ART was 14 years, and 56% were CDC Class C. Subjects showed multiple class ART resistance at baseline: 79% had ≥2 NRTI, 75% ≥1 NNRTI, and 71% ≥2 PI major mutations; 62% had non-R5 virus.
Mean change from baseline in HIV RNA at day 8 (primary endpoint) was -1.4log
10 copies/mL (95% CI -1.3 – -1.5log
10, p<0.001). Response was associated with baseline INI mutation pathway, as shown in Table 3. (See Table 3.)
Click on icon to see table/diagram/image
In patients without a primary mutation detected at baseline (N=60) (i.e. RAL/EVG not part of current failing therapy) there was a 1.63 log
10 reduction in viral load at day 8.
After the functional monotherapy phase, subjects had the opportunity to re-optimize their background regimen when possible. The overall response rate through 24 weeks of therapy, 69% (126/183), was generally sustained through 48 weeks with 116/183 (63%) of patients with HIV-1 RNA <50c/mL (ITT-E, Snapshot algorithm). When excluding patients who stopped therapy for non-efficacy reasons, and those with major protocol deviations (incorrect dolutegravir dosing, intake of prohibited co-medication), namely, "the Virological Outcome (VO)-population)", the corresponding response rates were 75% (120/161, week 24) and 69% (111/160, week 48).
The response was lower when the Q148-mutation was present at baseline, and in particular in the presence of ≥2 secondary mutations, Table 4. The overall susceptibility score (OSS) of the optimised background regimen (OBR) was not associated with Week 24 response, nor with the week 48 response. (See Table 4.)
Click on icon to see table/diagram/image
The median change in CD4+ T cell count from baseline for VIKING-3 based on observed data was 61 cells/mm
3 at Week 24 and 110 cells/mm
3 at Week 48.
In the double blind, placebo-controlled VIKING-4 study (ING116529), 30 HIV-1 infected, ART-experienced adults with primary genotypic resistance to INIs at Screening, were randomised to receive either dolutegravir 50 mg twice daily or placebo with the current failing regimen for 7 days followed by an open label phase with all subjects receiving dolutegravir. At baseline, median patient age was 49 years, 20% were female, 58% non-white, and 23% had hepatitis B and/or C co-infection. Median baseline CD4+ was 160 cells/mm
3, median duration of prior ART was 13 years, and 63% were CDC Class C. Subjects showed multiple class ART resistance at baseline: 80% had ≥2 NRTI, 73% ≥1 NNRTI, and 67% ≥2 PI major mutations; 83% had non-R5 virus. Sixteen of 30 subjects (53%) harboured Q148 virus at baseline. The primary endpoint at Day 8 showed that dolutegravir 50 mg twice daily was superior to placebo, with an adjusted mean treatment difference for the change from Baseline in Plasma HIV-1 RNA of -1.2 log
10 copies/mL (95% CI -1.5 - -0.8log
10 copies/mL, p<0.001). The day 8 responses in this placebo controlled study were fully in line with those seen in VIKING-3 (not placebo controlled), including by baseline integrase resistance categories. At week 48, 12/30 (40%) subjects had HIV-1 RNA <50 copies/mL (ITT-E, Snapshot algorithm).
In a combined analysis of VIKING-3 and VIKING-4 (n=186, VO population), the proportion of subjects with HIV RNA <50 copies/mL at Week 48 was 126/186 (68%). The proportion of subjects with HIV RNA <50 copies/mL was 96/126 (76%) for No Q148 mutations, 22/41 (54%) for Q148+1 and 5/19 (26%) for Q148+≥2 secondary mutations.
Paediatric population: In a Phase I/II 48 week multicentre, open-label study (P1093/ING112578), the pharmacokinetic parameters, safety, tolerability and efficacy of Dolutegravir will be evaluated in combination regimens in HIV-1 infected adolescents.
At 24 weeks, 16 of 23 (70%) adolescents (12 to less than 18 years of age) treated with Dolutegravir once daily (35 mg n=4, 50 mg n=19) plus OBR achieved viral load <50 copies/mL.
Four subjects had virologic failure none of which had INI resistance at the time of virologic failure.
The European Medicines Agency has deferred the obligation to submit the results of studies with combination of Dolutegravir in one or more subsets of the paediatric population (aged 4 weeks to below 12 years) in the treatment of HIV-1 infection (see Dosage & Administration for information on paediatric use).
Emtricitabine and Tenofovir alafenamide: In treatment-naïve patients: In a pooled analysis of antiretroviral-naïve patients receiving emtricitabine and tenofovir alafenamide (10 mg) given with elvitegravir and cobicistat as a fixed-dose combination tablet in GS-US-292-0104, GS-US-292-0111, and GS-US-292-0102, genotyping was performed on plasma HIV-1 isolates from all patients with HIV-1 RNA > 400 copies/mL at confirmed virological failure, at Week 48, or at the time of early study drug discontinuation. Through Week 48, the development of one or more primary emtricitabine, tenofovir alafenamide, or elvitegravir resistance-associated mutations was observed in HIV-1 isolates from 7 of 14 patients with evaluable genotypic data from paired baseline and E/C/F/TAF treatment-failure isolates (7 of 978 patients [0.7%]) compared with 7 of 15 treatment-failure isolates from patients in the E/C/F/TDF group (7 of 925 patients [0.8%]). In the E/C/F/TAF group, the mutations that emerged were M184V/I (n = 7) and K65R (n = 1) in RT and T66T/A/I/V (n = 2), E92Q (n = 2), Q148Q/R (n = 1), and N155H (n = 1) in integrase. In the E/C/F/TDF group, the mutations that emerged were M184V/I (n = 7) and K65R (n = 2) in RT and E92E/Q (n = 3) and Q148R (n = 2) in integrase. All HIV-1 isolates from patients in both treatment groups who developed resistance mutations to elvitegravir in integrase also developed resistance mutations to emtricitabine in RT.
Cross-resistance in HIV-1 infected, treatment-naïve or virologically suppressed patients: Emtricitabine-resistant viruses with the M184V/I substitution were cross-resistant to lamivudine, but retained sensitivity to didanosine, stavudine, tenofovir, and zidovudine.
The K65R and K70E mutations result in reduced susceptibility to abacavir, didanosine, lamivudine, emtricitabine, and tenofovir, but retain sensitivity to zidovudine.
Multinucleoside-resistant HIV-1 with a T69S double insertion mutation or with a Q151M mutation complex including K65R showed reduced susceptibility to tenofovir alafenamide.
Clinical data: Clinical efficacy of with Emtricitabine and Tenofovir alafenamide was established from studies conducted with emtricitabine and tenofovir alafenamide when given with elvitegravir and cobicistat as the fixed-dose combination tablet E/C/F/TAF.
HIV-1 infected, treatment-naïve patients: In studies GS-US-292-0104 and GS-US-292-0111, patients were randomized in a 1:1 ratio to receive either emtricitabine 200 mg and tenofovir alafenamide 10 mg (n = 866) once daily or emtricitabine 200 mg + tenofovir disoproxil (as fumarate) 245 mg (n = 867) once daily, both given with elvitegravir 150 mg + cobicistat 150 mg as a fixed-dose combination tablet. The mean age was 36 years (range: 18-76), 85% were male, 57% were White, 25% were Black, and 10% were Asian. Nineteen percent of patients were identified as Hispanic/Latino. The mean baseline plasma HIV-1 RNA was 4.5 log10 copies/mL (range: 1.3-7.0) and 23% had baseline viral loads > 100,000 copies/mL. The mean baseline CD4+ cell count was 427 cells/mm
3 (range: 0-1,360) and 13% had a CD4+ cell count < 200 cells/mm
3.
E/C/F/TAF met the non-inferiority criteria in achieving HIV-1 RNA < 50 copies/mL when compared to E/C/F/TDF. Pooled treatment outcomes at 48 weeks are shown in Table 5. (See Table 5.)
Click on icon to see table/diagram/image
The mean increases from baseline in CD4+ cell count at Week 48 was 230 cells/mm
3 in patients receiving emtricitabine and tenofovir alafenamide and 211 cells/mm
3 in patients receiving emtricitabine and tenofovir disoproxil fumarate (p = 0.024).
Clinical efficacy of with Emtricitabine and Tenofovir alafenamide in treatment-naïve patients was also established from a study conducted with emtricitabine and tenofovir alafenamide (10 mg) when given with darunavir (800 mg) and cobicistat as a fixed-dose combination tablet (D/C/F/TAF). In study GS-US-299-0102, patients were randomized in a 2:1 ratio to receive either fixed-dose combination D/C/F/TAF once daily (n = 103) or darunavir and cobicistat and emtricitabine/tenofovir disoproxil fumarate once daily (n = 50). The proportions of patients with plasma HIV-1 RNA < 50 copies/mL and < 20 copies/mL are shown in Table 6. (See Table 6.)
Click on icon to see table/diagram/image
HIV-1 infected virologically suppressed patients: In study GS-US-311-1089, the efficacy and safety of switching from emtricitabine/tenofovir disoproxil fumarate to with Emtricitabine and Tenofovir alafenamide while maintaining the third antiretroviral agent were evaluated in a randomized, double-blind study of virologically suppressed HIV-1 infected adults (n = 663). Patients must have been stably suppressed (HIV-1 RNA < 50 copies/mL) on their baseline regimen for at least 6 months and had HIV-1 with no resistance mutations to emtricitabine or tenofovir alafenamide prior to study entry. Patients were randomized in a 1:1 ratio to either switch to with Emtricitabine and Tenofovir alafenamide (n = 333), or stay on their baseline emtricitabine/tenofovir disoproxil fumarate containing regimen (n = 330). Patients were stratified by the class of the third agent in their prior treatment regimen. At baseline, 46% of patients were receiving emtricitabine/tenofovir disoproxil fumarate in combination with a boosted PI and 54% of patients were receiving emtricitabine/tenofovir disoproxil fumarate in combination with an unboosted third agent.
Treatment outcomes of study GS-US-311-1089 through 48 weeks are presented in Table 7. (See Table 7.)
Click on icon to see table/diagram/image
HIV-1 infected patients with mild to moderate renal impairment: In study GS-US-292-0112, the efficacy and safety of emtricitabine and tenofovir alafenamide were evaluated in an open-label clinical study in which 242 HIV-1 infected patients with mild to moderate renal impairment (eGFR
CG: 30-69 mL/min) were switched to emtricitabine and tenofovir alafenamide (10 mg) given with elvitegravir and cobicistat as a fixed-dose combination tablet. Patients were virologically suppressed (HIV-1 RNA < 50 copies/mL) for at least 6 months before switching.
The mean age was 58 years (range: 24-82), with 63 patients (26%) who were ≥ 65 years of age. Seventy-nine percent were male, 63% were White, 18% were Black, and 14% were Asian. Thirteen percent of patients were identified as Hispanic/Latino. At baseline, median eGFR was 56 mL/min, and 33% of patients had an eGFR from 30 to 49 mL/min. The mean baseline CD4+ cell count was 664 cells/mm
3 (range: 126-1,813). At Week 144, 83.1% (197/237 patients) maintained HIV-1 RNA < 50 copies/mL after switching to emtricitabine and tenofovir alafenamide given with elvitegravir and cobicistat as a fixed-dose combination tablet.
Changes in measures of bone mineral density: In studies in treatment-naïve patients, emtricitabine and tenofovir alafenamide given with elvitegravir and cobicistat or darunavir and cobicistat as a fixed-dose combination tablet was associated with smaller reductions in bone mineral density (BMD; as measured by hip and lumbar spine dual energy X ray absorptiometry [DXA] analysis) compared to E/C/F/TDF or darunavir, cobicistat, emtricitabine and tenofovir disoproxil fumarate after 48 weeks of treatment. Small improvements in BMD were noted at 48 weeks after switching to emtricitabine and tenofovir alafenamide containing regimen from a TDF containing regimen compared to maintaining the TDF containing regimen.
Changes in measures of renal function: In studies in treatment-naïve patients, emtricitabine and tenofovir alafenamide given with elvitegravir and cobicistat or darunavir and cobicistat as a fixed-dose combination tablet was associated with lower impact of renal safety parameters (as measured by eGFR
CG, urine protein to creatinine ratio, and urine albumin to creatinine ratio) compared to E/C/F/TDF or darunavir and cobicistat and emtricitabine/tenofovir disoproxil fumarate after 48 weeks of treatment (see also Precautions).
Paediatric population: In study GS-US-292-0106, the efficacy, safety, and pharmacokinetics of emtricitabine and tenofovir alafenamide were evaluated in an open-label study in which 50 HIV-1 infected, treatment-naïve adolescents received emtricitabine and tenofovir alafenamide (10 mg) given with elvitegravir and cobicistat as a fixed-dose combination tablet. Patients had a mean age of 15 years (range: 12-17), and 56% were female, 12% were Asian, and 88% were Black. At baseline, median plasma HIV-1 RNA was 4.7 log
10 copies/mL, median CD4+ cell count was 456 cells/mm
3 (range: 95-1,110), and median CD4+% was 23% (range: 7-45%). Overall, 22% had baseline plasma HIV-1 RNA > 100,000 copies/mL. At 48 weeks, 92% (46/50) achieved HIV-1 RNA < 50 copies/mL, similar to response rates in studies of treatment-naïve HIV-1 infected adults. The mean increases from baseline in CD4+ cell count at Week 48 was 224 cells/mm
3. No emergent resistance to E/C/F/TAF was detected through Week 48.
Pharmacokinetics: Dolutegravir pharmacokinetics are similar between healthy and HIV-infected subjects. The PK variability of dolutegravir is low to moderate. In Phase I studies in healthy subjects, between-subject CVb% for AUC and C
max ranged from ~20 to 40% and Cτ from 30 to 65% across studies. The between-subject PK variability of dolutegravir was higher in HIV-infected subjects than healthy subjects. Within-subject variability (CVw%) is lower than between-subject variability.
Absorption: Dolutegravir is rapidly absorbed following oral administration, with median T
max at 2 to 3 hours post dose for tablet formulation.
Food increased the extent and slowed the rate of absorption of dolutegravir. Bioavailability of dolutegravir depends on meal content: low, moderate, and high fat meals increased dolutegravir AUC
(0-∞) by 33%, 41%, and 66%, increased C
max by 46%, 52%, and 67%, prolonged T
max to 3, 4, and 5 hours from 2 hours under fasted conditions, respectively. These increases may be clinically relevant in the presence of certain integrase class resistance. Therefore, Dolutegravir is recommended to be taken with food by patients infected with HIV with integrase class resistance (see Dosage & Administration).
The absolute bioavailability of dolutegravir has not been established.
Emtricitabine is rapidly and extensively absorbed following oral administration with peak plasma concentrations occurring at 1 to 2 hours post-dose. Following multiple dose oral administration of emtricitabine to 20 HIV-1 infected subjects, the (mean ± SD) steady state plasma emtricitabine peak concentrations (C
max) were 1.8 ± 0.7 μg/mL and the area-under the plasma concentration-time curve over a 24-hour dosing interval (AUC) was 10.0 ± 3.1 μg·h/mL. The mean steady state plasma trough concentration at 24 hours post-dose was equal to or greater than the mean
in vitro IC
90 value for anti-HIV-1 activity.
Emtricitabine systemic exposure was unaffected when emtricitabine was administered with food.
Following administration of food in healthy subjects, peak plasma concentrations were observed approximately 1 hour post-dose for tenofovir alafenamide administered as F/TAF (25 mg) or E/C/F/TAF (10 mg). The mean C
max and AUC
last, (mean ± SD) under fed conditions following a single 25 mg dose of tenofovir alafenamide administered in Dolutegravir, Emtricitabine and Tenofovir alafenamide were 0.21 ± 0.13 μg/mL and 0.25 ± 0.11 μg·h/mL, respectively. The mean C
max and AUC
last following a single 10 mg dose of tenofovir alafenamide administered in E/C/F/TAF were 0.21 ± 0.10 μg/mL and 0.25 ± 0.08 μg·h/mL, respectively.
Relative to fasting conditions, the administration of tenofovir alafenamide with a high fat meal (~800 kcal, 50% fat) resulted in a decrease in tenofovir alafenamide C
max (15-37%) and an increase in AUC
last (17-77%).
Distribution: Dolutegravir is highly bound (>99%) to human plasma proteins based on
in vitro data. The apparent volume of distribution is 17 L to 20 L in HIV-infected patients, based on a population pharmacokinetic analysis. Binding of dolutegravir to plasma proteins is independent of dolutegravir concentration. Total blood and plasma drug-related radioactivity concentration ratios averaged between 0.441 to 0.535, indicating minimal association of radioactivity with blood cellular components. The unbound fraction of dolutegravir in plasma is increased at low levels of serum albumin (<35 g/L) as seen in subjects with moderate hepatic impairment.
Dolutegravir is present in cerebrospinal fluid (CSF). In 13 treatment-naïve subjects on a stable dolutegravir plus abacavir/lamivudine regimen, dolutegravir concentration in CSF averaged 18 ng/mL (comparable to unbound plasma concentration, and above the IC
50).
Dolutegravir is present in the female and male genital tract. AUC in cervicovaginal fluid, cervical tissue and vaginal tissue were 6-10% of those in corresponding plasma at steady state. AUC in semen was 7% and 17% in rectal tissue of those in corresponding plasma at steady state.
In vitro binding of emtricitabine to human plasma proteins was < 4% and independent of concentration over the range of 0.02-200 μg/mL. At peak plasma concentration, the mean plasma to blood drug concentration ratio was ~1.0 and the mean semen to plasma drug concentration ratio was ~4.0.
In vitro binding of tenofovir to human plasma proteins is < 0.7% and is independent of concentration over the range of 0.01-25 μg/mL.
Ex vivo binding of tenofovir alafenamide to human plasma proteins in samples collected during clinical studies was approximately 80%.
Biotransformation: Dolutegravir is primarily metabolized through glucuronidation via UGT1A1 with a minor CYP3A component. Dolutegravir is the predominant circulating compound in plasma; renal elimination of unchanged active substance is low (< 1% of the dose). Fifty-three percent of total oral dose is excreted unchanged in the faeces. It is unknown if all or part of this is due to unabsorbed active substance or biliary excretion of the glucuronidate conjugate, which can be further degraded to form the parent compound in the gut lumen. Thirty-two percent of the total oral dose is excreted in the urine, represented by ether glucuronide of dolutegravir (18.9% of total dose), N-dealkylation metabolite (3.6% of total dose), and a metabolite formed by oxidation at the benzylic carbon (3.0% of total dose).
In vitro studies indicate that emtricitabine is not an inhibitor of human CYP enzymes. Following administration of [
14C]-emtricitabine, complete recovery of the emtricitabine dose was achieved in urine (~86%) and faeces (~14%). Thirteen percent of the dose was recovered in the urine as three putative metabolites. The biotransformation of emtricitabine includes oxidation of the thiol moiety to form the 3'-sulfoxide diastereomers (~9% of dose) and conjugation with glucuronic acid to form 2'-O-glucuronide (~4% of dose). No other metabolites were identifiable.
Metabolism is a major elimination pathway for tenofovir alafenamide in humans, accounting for > 80% of an oral dose.
In vitro studies have shown that tenofovir alafenamide is metabolised to tenofovir (major metabolite) by cathepsin A in PBMCs (including lymphocytes and other HIV target cells) and macrophages; and by carboxylesterase-1 in hepatocytes.
In vivo, tenofovir alafenamide is hydrolyzed within cells to form tenofovir (major metabolite), which is phosphorylated to the active metabolite tenofovir diphosphate. In human clinical studies, a 10 mg oral dose of tenofovir alafenamide (given with emtricitabine and elvitegravir and cobicistat) resulted in tenofovir diphosphate concentrations > 4-fold higher in PBMCs and > 90% lower concentrations of tenofovir in plasma as compared to a 245 mg oral dose of tenofovir disoproxil (as fumarate) (given with emtricitabine and elvitegravir and cobicistat).
In vitro, tenofovir alafenamide is not metabolised by CYP1A2, CYP2C8, CYP2C9, CYP2C19, or CYP2D6. Tenofovir alafenamide is minimally metabolised by CYP3A4. Upon co-administration with the moderate CYP3A inducer probe efavirenz, tenofovir alafenamide exposure was not significantly affected. Following administration of tenofovir alafenamide, plasma [
14C]-radioactivity showed a time-dependent profile with tenofovir alafenamide as the most abundant species in the initial few hours and uric acid in the remaining period.
Elimination: Dolutegravir has a terminal half-life of ~14 hours. The apparent oral clearance (CL/F) is approximately 1L/hr in HIV-infected patients based on a population pharmacokinetic analysis.
Emtricitabine is primarily excreted by the kidneys with complete recovery of the dose achieved in urine (approximately 86%) and faeces (approximately 14%). Thirteen percent of the emtricitabine dose was recovered in urine as three metabolites. The systemic clearance of emtricitabine averaged 307 mL/min. Following oral administration, the elimination half-life of emtricitabine is approximately 10 hours.
Renal excretion of intact tenofovir alafenamide is a minor pathway with < 1% of the dose eliminated in urine. Tenofovir alafenamide is mainly eliminated following metabolism to tenofovir. Tenofovir alafenamide and tenofovir have a median plasma half-life of 0.51 and 32.37 hours, respectively. Tenofovir is eliminated from the body by the kidneys by both glomerular filtration and active tubular secretion.
Drug interactions: In vitro, dolutegravir demonstrated no direct, or weak inhibition (IC
50>50 μM) of the enzymes cytochrome P450 (CYP)1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP3A, uridine diphosphate glucuronosyl transferase (UGT)1A1 or UGT2B7, or the transporters Pgp, BCRP, BSEP, OATP1B1, OATP1B3, OCT1, MATE2-K, MRP2 or MRP4.
In vitro, dolutegravir did not induce CYP1A2, CYP2B6 or CYP3A4. Based on this data, dolutegravir is not expected to affect the pharmacokinetics of medicinal products that are substrates of major enzymes or transporters (see Interactions).
In vitro, dolutegravir was not a substrate of human OATP 1B1, OATP 1B3 or OCT 1.
Age, gender, and ethnicity: Population PK analyses using pooled pharmacokinetic data from Phase IIb and Phase III adult trials revealed no clinically relevant effect of gender on the exposure of dolutegravir.
Population PK analyses using pooled pharmacokinetic data from Phase IIb and Phase III adult trials revealed no clinically relevant effect of race on the exposure of dolutegravir.
The pharmacokinetics of dolutegravir following single dose oral administration to Japanese subjects appear similar to observed parameters in Western (US) subjects.
No clinically relevant pharmacokinetic differences due to age, gender or ethnicity have been identified for emtricitabine, or tenofovir alafenamide.
Elderly: Population pharmacokinetic analysis of dolutegravir using data in HIV-1 infected adults showed that there was no clinically relevant effect of age on dolutegravir exposure.
Pharmacokinetic data for dolutegravir in subjects >65 years of age are limited.
Paediatric population: The pharmacokinetics of dolutegravir in 10 antiretroviral treatment-experienced HIV-1 infected adolescents (12 to <18 years of age) showed that Dolutegravir 50 mg once daily oral dosage resulted in dolutegravir exposure comparable to that observed in adults who received Dolutegravir 50 mg orally once daily.
Exposures of emtricitabine and tenofovir alafenamide (given with elvitegravir and cobicistat) achieved in 24 paediatric patients aged 12 to < 18 years who received emtricitabine and tenofovir alafenamide given with elvitegravir and cobicistat in study GS-US-292-0106 were similar to exposures achieved in treatment-naïve adults (Table 8). (See Table 8.)
Click on icon to see table/diagram/image
Linearity/non-linearity: The linearity of dolutegravir pharmacokinetics is dependent on dose and formulation. Following oral administration of tablet formulations, in general, dolutegravir exhibited nonlinear pharmacokinetics with less than dose-proportional increases in plasma exposure from 2 to 100 mg; however, increase in dolutegravir exposure appears dose proportional from 25 mg to 50 mg for the tablet formulation. With 50 mg twice daily, the exposure over 24 hours was approximately doubled compared to 50 mg once daily.
Pharmacokinetic/pharmacodynamic relationship(s): In a randomized, dose-ranging trial, HIV-1–infected subjects treated with dolutegravir monotherapy (ING111521) demonstrated rapid and dose-dependent antiviral activity, with mean decline in HIV-1 RNA of 2.5 log
10 at day 11 for 50 mg dose. This antiviral response was maintained for 3 to 4 days after the last dose in the 50 mg group.
PK/PD modelling using pooled data from clinical studies in integrase resistant patients suggest that increasing the dose from 50 mg twice daily to 100 mg twice daily may increase the effectiveness of dolutegravir in patients with integrase resistance and limited treatment options due to advanced multi class resistance. The proportion of responders (HIV-1 RNA <50 c/mL) at week 24 was predicted to increase around 4-18% in the subjects with Q148 + ≥2 secondary mutations from G140A/C/S, E138A/K/T, L74I.
Although these simulated results have not been confirmed in clinical trials, this high dose may be considered in the presence of the Q148 + ≥2 secondary mutations from G140A/C/S, E138A/K/T, L74I in patients with overall limited treatment options due to advanced multi class resistance. There is no clinical data on the safety or efficacy of the 100 mg twice daily dose. Co-treatment with atazanavir increases the exposure of dolutegravir markedly, and should not be used in combination with this high dose, since safety with the resulting dolutegravir exposure has not been established.
Renal impairment: Renal clearance of unchanged active substance is a minor pathway of elimination for dolutegravir. A study of the pharmacokinetics of dolutegravir was performed in subjects with severe renal impairment (CrCL <30 mL/min) and matched healthy controls. The exposure to dolutegravir was decreased by approximately 40% in subjects with severe renal impairment. The mechanism for the decrease is unknown. No dosage adjustment is considered necessary for patients with renal impairment. Dolutegravir has not been studied in patients on dialysis.
No clinically relevant differences in tenofovir alafenamide, or tenofovir pharmacokinetics were observed between healthy subjects and patients with severe renal impairment (estimated CrCl > 15 but < 30 mL/min) in studies of tenofovir alafenamide. There are no pharmacokinetic data on tenofovir alafenamide in patients with estimated CrCl < 15 mL/min. Mean systemic emtricitabine exposure was higher in patients with severe renal impairment (CrCl < 30 mL/min) (33.7 μg·h/ml) than in subjects with normal renal function (11.8 μg·h/mL).
Hepatic impairment: Dolutegravir is primarily metabolized and eliminated by the liver. A single dose of 50 mg of dolutegravir was administered to 8 subjects with moderate hepatic impairment (Child-Pugh class B) and to 8 matched healthy adult controls. While the total dolutegravir concentration in plasma was similar, a 1.5- to 2-fold increase in unbound exposure to dolutegravir was observed in subjects with moderate hepatic impairment compared to healthy controls. No dosage adjustment is considered necessary for patients with mild to moderate hepatic impairment. The effect of severe hepatic impairment on the pharmacokinetics of Dolutegravir has not been studied.
The pharmacokinetics of emtricitabine have not been studied in subjects with hepatic impairment; however, emtricitabine is not significantly metabolised by liver enzymes, so the impact of liver impairment should be limited. Clinically relevant changes in tenofovir pharmacokinetics in patients with hepatic impairment were not observed in patients with mild to moderate hepatic impairment, and no tenofovir alafenamide dose adjustment is required in patients with mild to moderate hepatic impairment. The effect of severe hepatic impairment (Child-Pugh Class C) on the pharmacokinetics of tenofovir alafenamide has not been studied.
Hepatitis B and/or hepatitis C virus co-infection: Population pharmacokinetic analysis indicated that hepatitis C virus co-infection had no clinically relevant effect on the exposure to dolutegravir. There are limited data on subjects with hepatitis B co-infection.
The pharmacokinetics of emtricitabine and tenofovir alafenamide have not been fully evaluated in patients co-infected with HBV and/or HCV.
Polymorphisms in drug metabolising enzymes: There is no evidence that common polymorphisms in drug metabolising enzymes alter dolutegravir pharmacokinetics to a clinically meaningful extent. In a meta-analysis using pharmacogenomics samples collected in clinical studies in healthy subjects, subjects with UGT1A1 (n=7) genotypes conferring poor dolutegravir metabolism had a 32% lower clearance of dolutegravir and 46% higher AUC compared with subjects with genotypes associated with normal metabolism via UGT1A1 (n=41).
Toxicology: Preclinical safety data: Dolutegravir: Dolutegravir was not mutagenic or clastogenic using
in vitro tests in bacteria and cultured mammalian cells, and an
in vivo rodent micronucleus assay. Dolutegravir was not carcinogenic in long term studies in the mouse and rat.
Dolutegravir did not affect male or female fertility in rats at doses up to 1000 mg/kg/day, the highest dose tested (24 times the 50 mg twice daily human clinical exposure based on AUC).
Oral administration of dolutegravir to pregnant rats at doses up to 1000 mg/kg daily from days 6 to 17 of gestation did not elicit maternal toxicity, developmental toxicity or teratogenicity (27 times the 50 mg twice daily human clinical exposure based on AUC).
Oral administration of dolutegravir to pregnant rabbits at doses up to 1000 mg/kg daily from days 6 to 18 of gestation did not elicit developmental toxicity or teratogenicity (0.40 times the 50 mg twice daily human clinical exposure based on AUC). In rabbits, maternal toxicity (decreased food consumption, scant/no faeces/urine, suppressed body weight gain) was observed at 1000 mg/kg (0.40 times the 50 mg twice daily human clinical exposure based on AUC).
The effect of prolonged daily treatment with high doses of dolutegravir has been evaluated in repeat oral dose toxicity studies in rats (up to 26 weeks) and in monkeys (up to 38 weeks). The primary effect of dolutegravir was gastrointestinal intolerance or irritation in rats and monkeys at doses that produce systemic exposures approximately 21 and 0.82 times the 50 mg twice daily human clinical exposure based on AUC, respectively. Because gastrointestinal (GI) intolerance is considered to be due to local active substance administration, mg/kg or mg/m
2 metrics are appropriate determinates of safety cover for this toxicity. GI intolerance in monkeys occurred at 15 times the human mg/kg equivalent dose (based on a 50 kg human), and 5 times the human mg/m
2 equivalent dose for a clinical dose of 50 mg twice daily.
Emtricitabine and Tenofovir alafenamide: Non-clinical data on emtricitabine reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction and development. Emtricitabine has demonstrated low carcinogenic potential in mice and rats.
Non-clinical studies of tenofovir alafenamide in rats and dogs revealed bone and kidney as the primary target organs of toxicity. Bone toxicity was observed as reduced BMD in rats and dogs at tenofovir exposures at least four times greater than those expected after administration of with Emtricitabine and Tenofovir alafenamide. A minimal infiltration of histiocytes was present in the eye in dogs at tenofovir alafenamide and tenofovir exposures of approximately 4 and 17 times greater, respectively, than those expected after administration of Dolutegravir, Emtricitabine and Tenofovir alafenamide.
Tenofovir alafenamide was not mutagenic or clastogenic in conventional genotoxicity assays.
Because there is a lower tenofovir exposure in rats and mice after the administration of tenofovir alafenamide compared to tenofovir disoproxil fumarate, carcinogenicity studies and a rat peri-postnatal study were conducted only with tenofovir disoproxil fumarate. No special hazard for humans was revealed in conventional studies of carcinogenic potential and toxicity to reproduction and development.
Reproductive toxicity studies in rats and rabbits showed no effects on mating, fertility, pregnancy or fetal parameters. However, tenofovir disoproxil fumarate reduced the viability index and weight of pups in a peri-postnatal toxicity study at maternally toxic doses.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image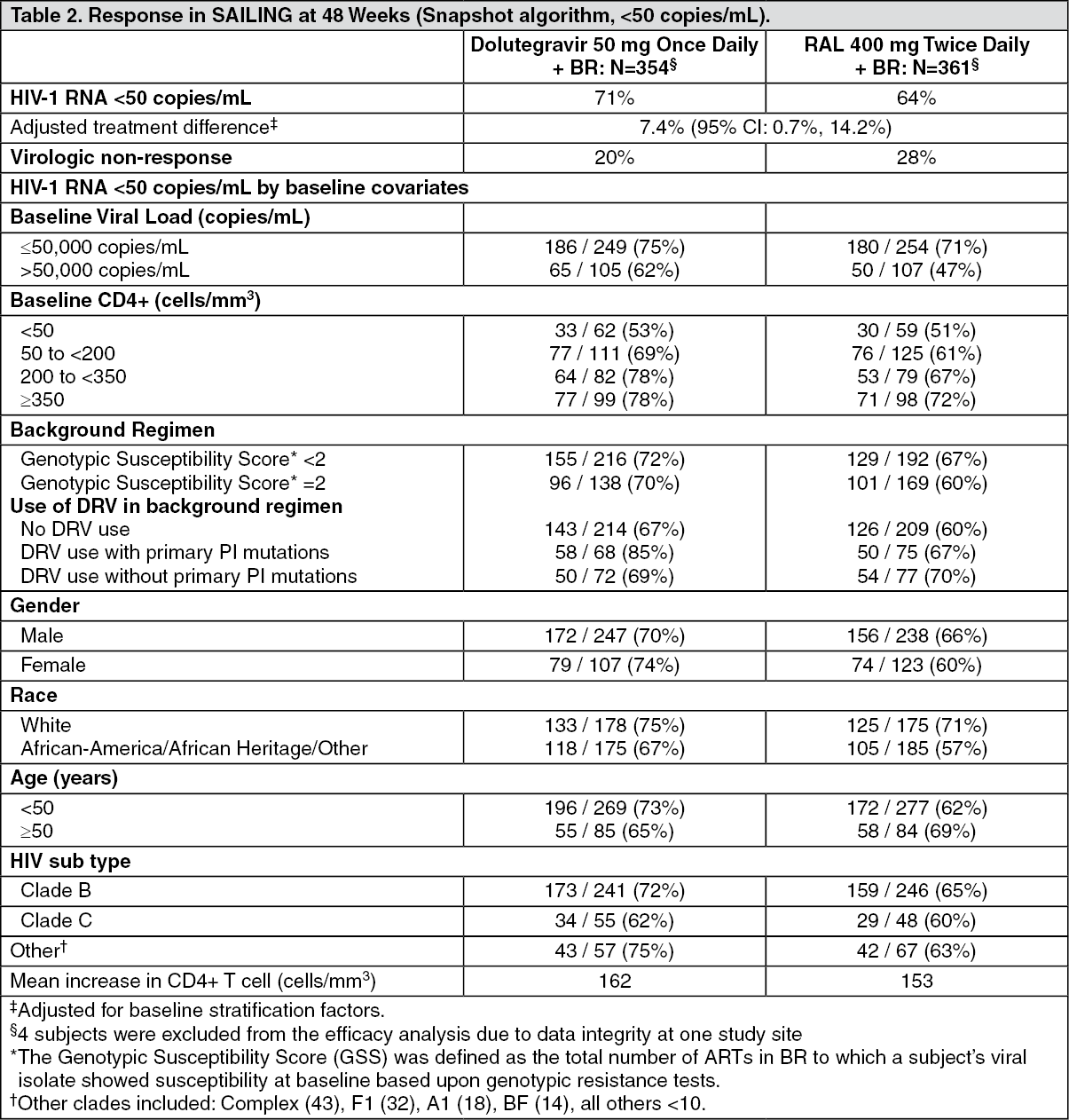 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image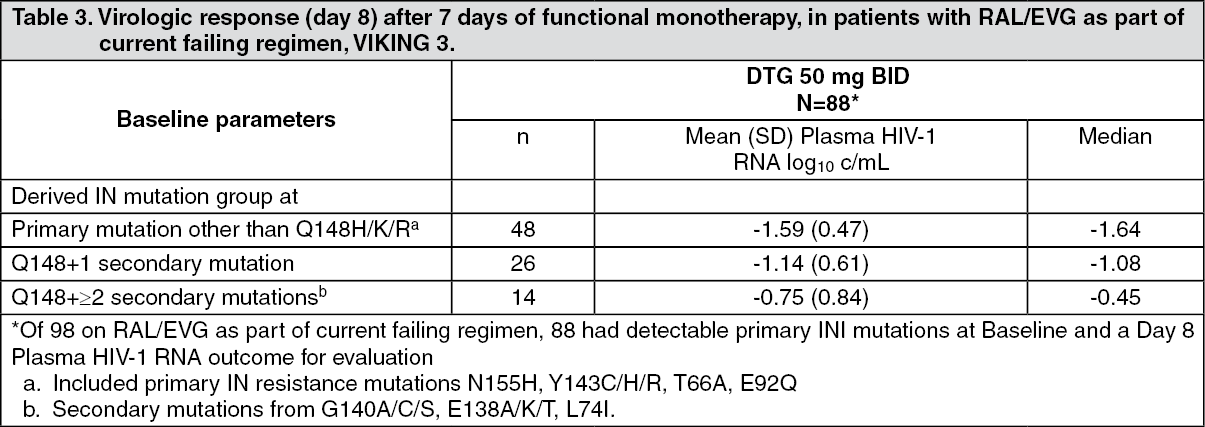 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image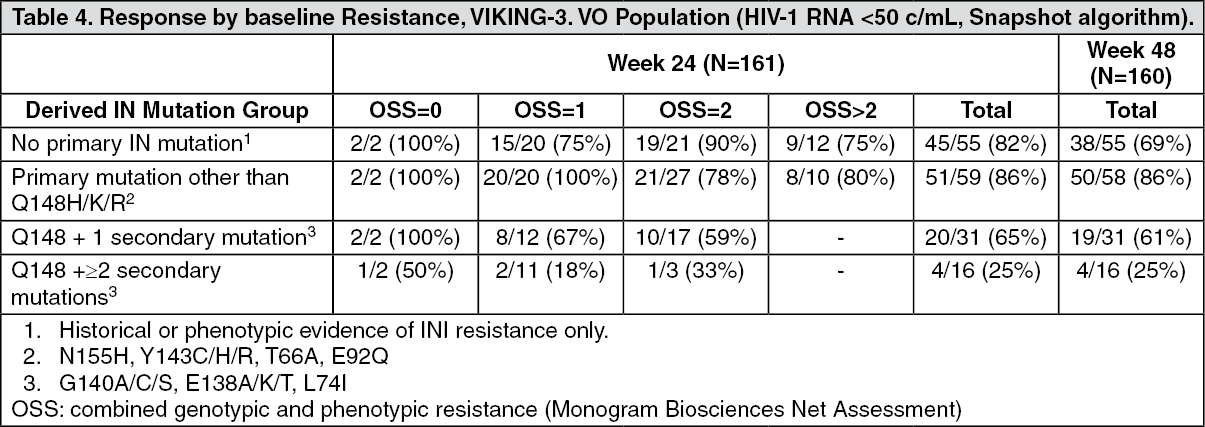 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image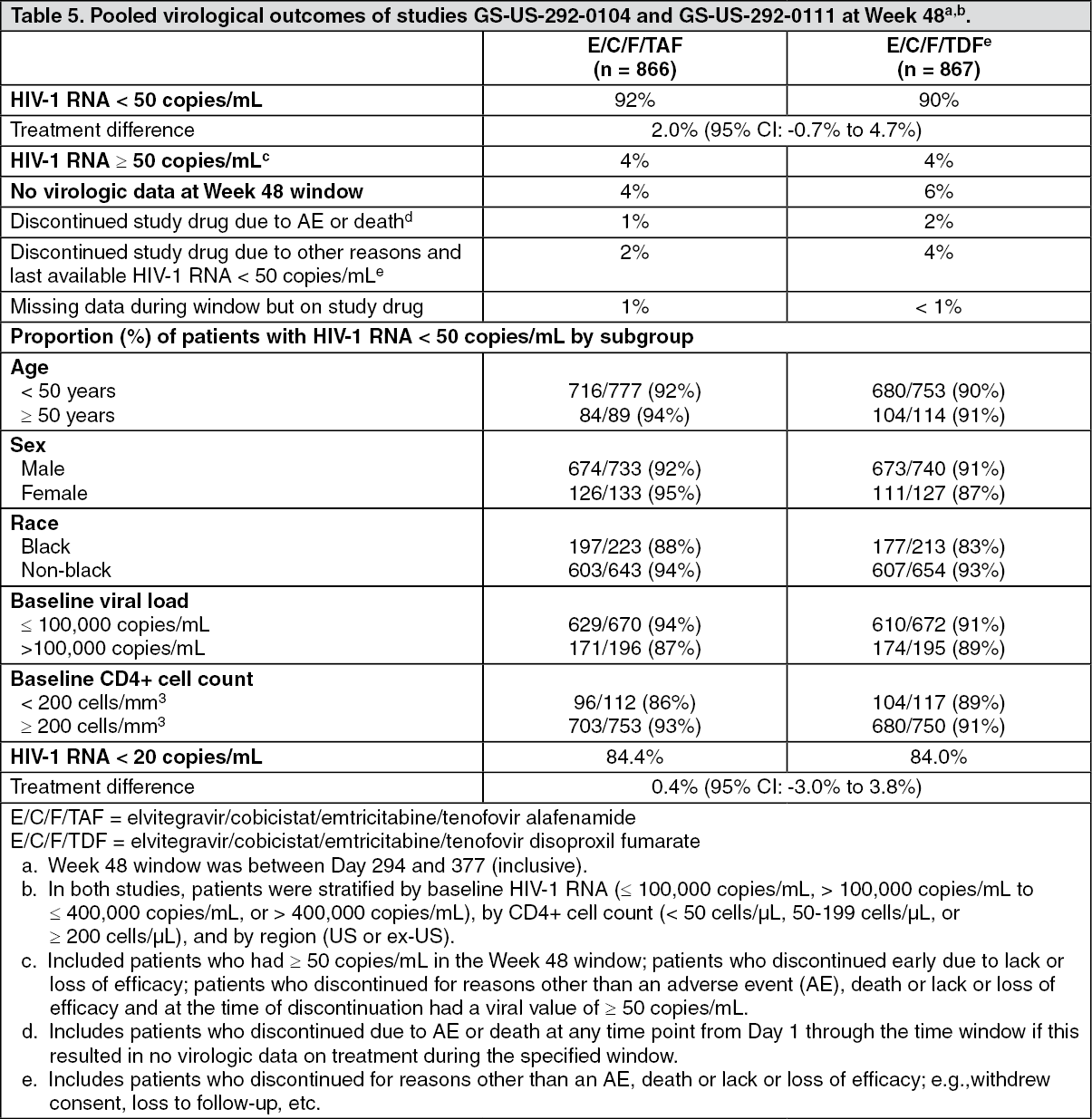 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image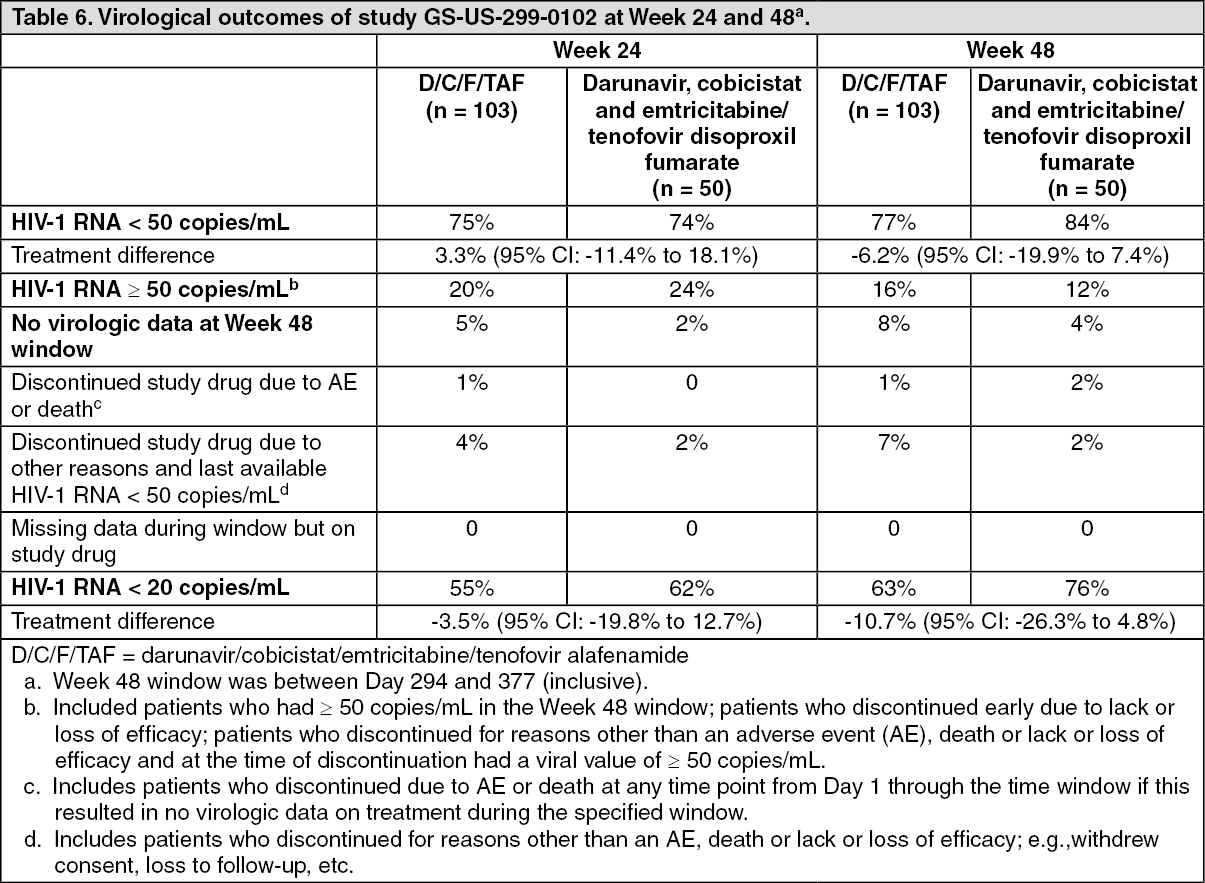 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image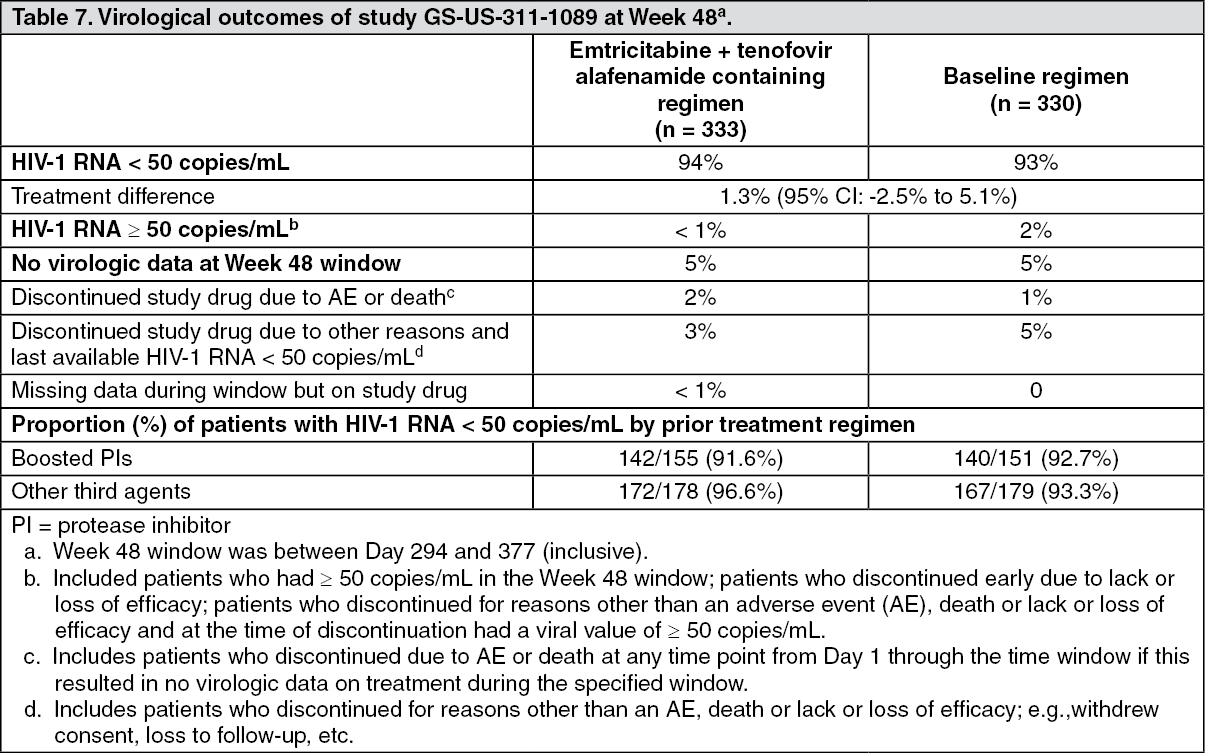 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image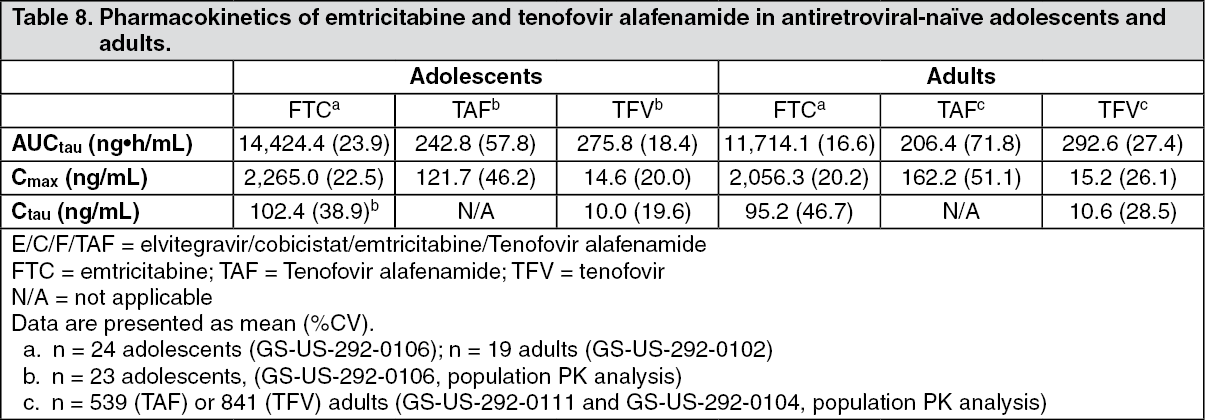 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out