


 Sign Out
Sign Out
If a patient misses a dose, and it cannot be taken within 12 hours, then that dose should be skipped and the next dose should be taken at the usual time of administration.
Treatment should continue as long as clinical benefit is observed or until unacceptable toxicity occurs.
Optimal medical management (i.e. treatment or therapy) for nausea, vomiting, and diarrhoea should be initiated prior to any lenvatinib therapy interruption or dose reduction; however, gastrointestinal toxicity should be actively treated in order to reduce the risk of development of renal impairment or failure (see Renal failure and impairment under Precautions).
Posology: DTC: The recommended daily dose of lenvatinib is 24 mg (two 10 mg capsules and one 4 mg capsule) once daily. The daily dose is to be modified as needed according to the dose/toxicity management plan.
RCC: First-Line Treatment of Patients with Advanced RCC: The recommended starting daily dose of lenvatinib is 20 mg (two 10-mg capsules) once daily in combination with pembrolizumab 200 mg administered as an intravenous infusion over 30 minutes every 3 weeks.
Refer to the pembrolizumab prescribing information for other pembrolizumab dosing information.
Previously Treated RCC: The recommended daily dose of lenvatinib is 18 mg (one 10 mg capsule and two 4 mg capsules) once daily in combination with 5 mg of everolimus once daily.
Refer to the everolimus prescribing information for other everolimus dosing information.
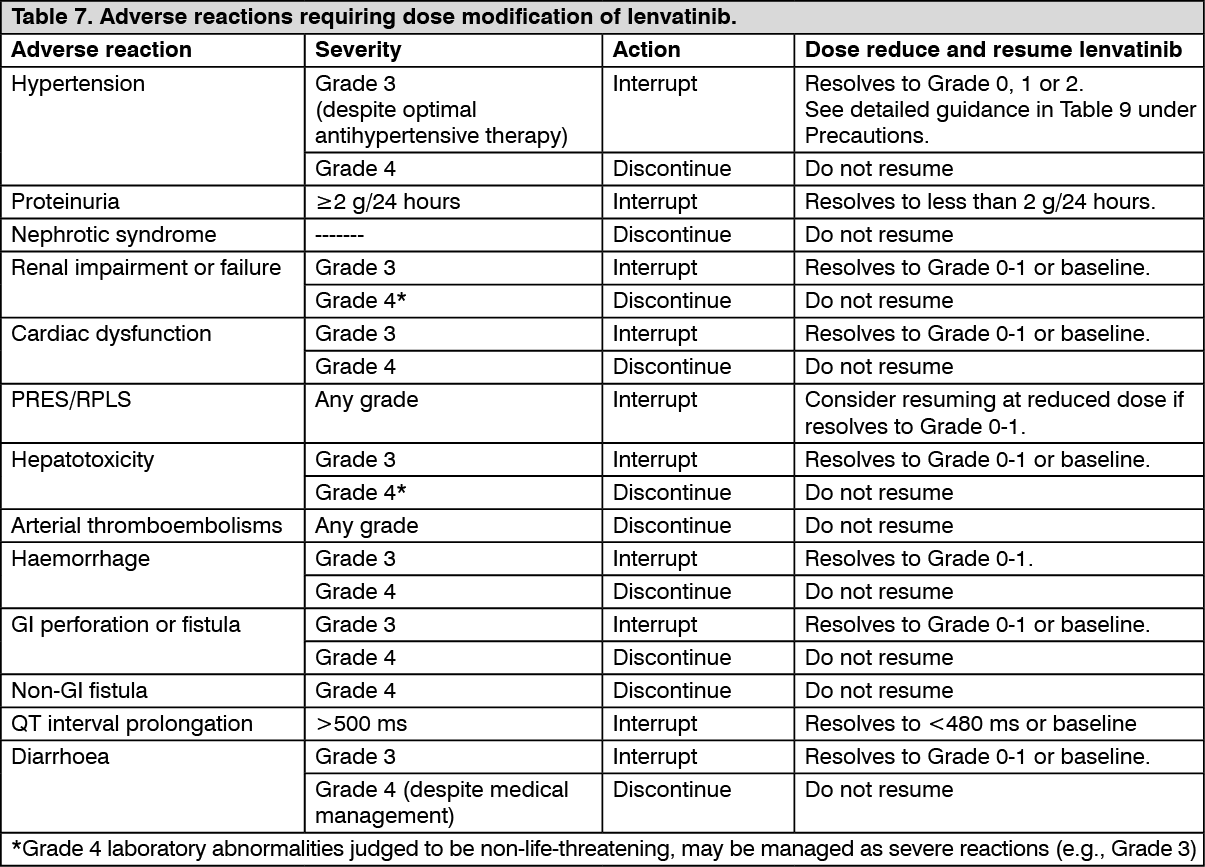
Dose adjustment and discontinuations for DTC and RCC: Management of adverse reactions may require dose interruption, adjustment, or discontinuation of lenvatinib therapy or the combination therapy with everolimus (see Precautions). Mild to moderate adverse reactions (e.g., Grade 1 or 2) generally do not warrant interruption of lenvatinib or of the combination, unless intolerable to the patient despite optimal management. Severe (e.g., Grade 3) or intolerable adverse reactions require interruption of lenvatinib or the combination until improvement of the reaction to Grade 0-1 or baseline.
For lenvatinib related toxicities (see Table 7), upon resolution/improvement of an adverse reaction to Grade 0-1 or baseline, treatment should be resumed at a reduced dose of lenvatinib as suggested in Table 8.
For toxicities thought to be related to everolimus, treatment should be interrupted, reduced to alternate day dosing, or discontinued (see the everolimus SmPC for advice on specific adverse reactions).
For toxicities thought to be related to both lenvatinib and everolimus, lenvatinib should be withheld or reduced (see Table 8) prior to reducing everolimus. Refer to the everolimus prescribing information for additional dose modification information.
Treatment should be discontinued in case of life-threatening reactions (e.g., Grade 4) with the exception of laboratory abnormality judged to be non-life-threatening, in which case they should be managed as severe reaction (e.g., Grade 3).
HCC: The recommended daily dose of lenvatinib is 8 mg (two 4 mg capsules) once daily for patients with a body weight of <60 kg and 12 mg (three 4 mg capsules) once daily for patients with a body weight of ≥60 kg. Dose adjustments are based only on toxicities observed and not on body weight changes during treatment. The daily dose is to be modified, as needed, according to the dose/toxicity management plan.
Dose adjustment and Discontinuation for HCC: Management of some adverse reactions may require dose interruption, adjustment, or discontinuation of lenvatinib therapy. Mild to moderate adverse reactions (e.g., Grade 1 or 2) generally do not warrant interruption of lenvatinib, unless intolerable to the patient despite optimal management. Details for monitoring, dose adjustment and discontinuation are provided in Table 8.
Grades are based on the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events (CTCAE).
EC: The recommended dosage of lenvatinib is 20 mg orally once daily in combination with pembrolizumab 200 mg administered as an intravenous infusion over 30 minutes every 3 weeks until unacceptable toxicity or disease progression.
Refer to the pembrolizumab prescribing information for other pembrolizumab dosing information.
Details for monitoring, dose adjustment and discontinuation are provided in Table 8.
Recommended Dose Modifications for Adverse Reactions for LENVIMA in Combination with Pembrolizumab: When administering lenvatinib in combination with pembrolizumab, modify the dosage one or both drugs as appropriate. Withhold, dose reduce or discontinue LENVIMA as shown in Table 7. Refer to pembrolizumab prescribing information for additional dose modification information.
Recommended Dose Modifications for Adverse Reactions for LENVIMA in Combination with Everolimus: When administering LENVIMA in combination with everolimus, withhold or reduce the LENVIMA dose first and then the everolimus dose for adverse reactions of both LENVIMA and everolimus. Refer to the everolimus prescribing information for additional dose modification information.
For lenvatinib related toxicities (see Table 7), upon resolution/improvement of an adverse reaction to Grade 0, 1 or baseline, treatment should be resumed at a reduced dose of lenvatinib as suggested in Table 8. (See Tables 7 and 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image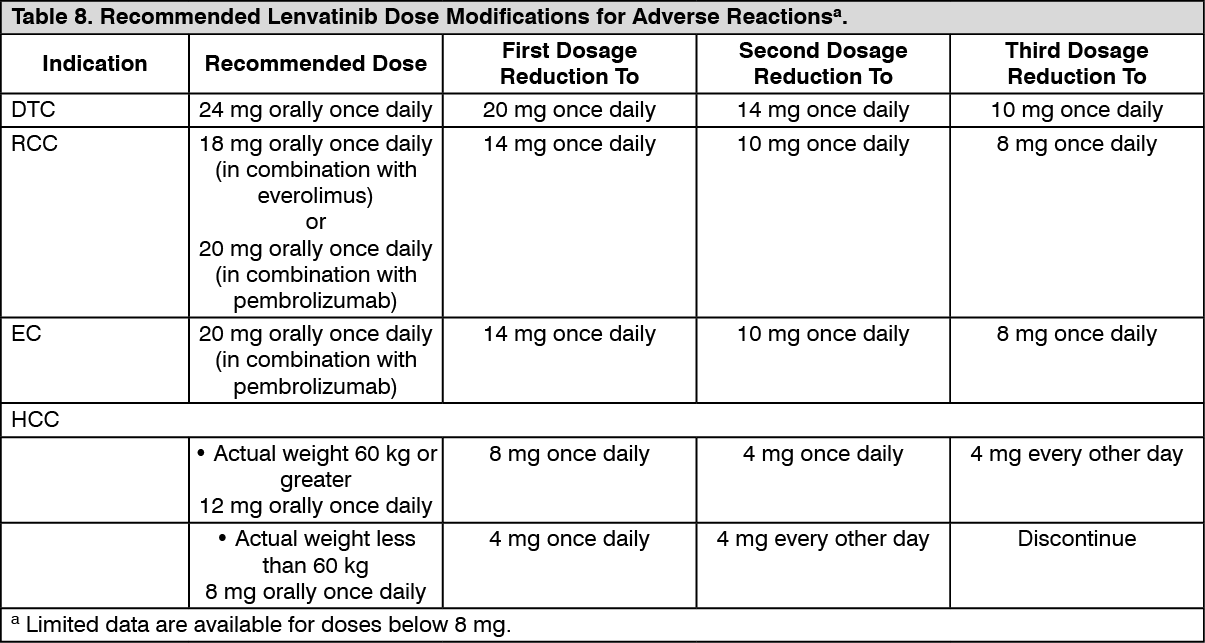 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSpecial populations: DTC: Patients of age ≥75 years, of Asian race, with comorbidities (such as hypertension, and hepatic or renal impairment), or body weight below 60 kg appear to have reduced tolerability to lenvatinib (see Other special populations under Adverse Reactions). All patients other than those with severe hepatic or renal impairment (see as follows) should initiate treatment at the recommended 24 mg dose, following which the dose should be further adjusted on the basis of individual tolerability.
RCC: No data for the combination of lenvatinib and everolimus are available for most of the special populations. The following information is derived from the clinical experience on single agent lenvatinib in patients with differentiated thyroid cancer (DTC).
All patients other than those with severe hepatic or renal impairment (see as follows) should initiate treatment at the recommended dose of 20 mg of lenvatinib daily with pembrolizumab or 18 mg of lenvatinib with 5 mg of everolimus taken once daily as indicated, following which the dose should be further adjusted on the basis of individual tolerability.
HCC: Patients ≥75 years, of white race or female sex or those with worse baseline hepatic impairment (Child-Pugh A score of 6 compared to score of 5) appear to have reduced tolerability to lenvatinib.
HCC patients other than those with moderate and severe hepatic impairment or severe renal impairment should initiate treatment at the recommended starting dose of 8 mg (two 4 mg capsules) for body weight <60 kg and 12 mg (three 4 mg capsules) for body weight ≥60 kg, following which the dose should be further adjusted on the basis of individual tolerability.
Patients with hypertension: Blood pressure should be well controlled prior to treatment with lenvatinib, and should be regularly monitored during treatment (see Precautions). Refer also to Other special populations under Adverse Reactions.
Patients with hepatic impairment: In DTC patients, no adjustment of starting dose is required on the basis of hepatic function in patients with mild (Child-Pugh A) or moderate (Child-Pugh B) hepatic impairment. In patients with severe (Child-Pugh C) hepatic impairment, the recommended starting dose for DTC is 14 mg taken once daily. Further dose adjustments may be necessary on the basis of individual tolerability. Refer also to Other special populations under Adverse Reactions.
In RCC, no data for the combination of lenvatinib with everolimus are available in patients with hepatic impairment. No adjustment of starting dose of the combination is required on the basis of hepatic function in patients with mild (Child Pugh A) or moderate (Child Pugh B) hepatic impairment. In patients with severe (Child Pugh C) hepatic impairment, the recommended starting dose of lenvatinib is 10 mg taken once daily in combination with the dose of everolimus (recommended in the everolimus SmPC) taken once daily. Further dose adjustments may be necessary on the basis of individual tolerability. The combination therapy should be used in patients with severe hepatic impairment only if the anticipated benefit exceeds the risk. Refer also to Other special populations under Adverse Reactions.
In the patient populations enrolled in the HCC study, no dose adjustments were required on the basis of hepatic function in those patients who had mild hepatic impairment (Child-Pugh A). The available very limited data are not sufficient to allow for a dosing recommendation for HCC patients with moderate hepatic impairment (Child-Pugh B). Close monitoring of overall safety is recommended in these patients (see Precautions and Pharmacology: Pharmacokinetics under Actions). Lenvatinib has not been studied in patients with severe hepatic impairment (Child-Pugh C) and is not recommended for use in these patients.
In the patient populations enrolled in the endometrial carcinoma study, no adjustments of starting dose were required on the basis of hepatic function in patients with mild (Child-Pugh A) or moderate (Child-Pugh B) hepatic impairment. In patients with severe (Child-Pugh C) hepatic impairment, the recommended dose of LENVIMA is 10 mg for the treatment of endometrial carcinoma, taken orally once daily.
Patients with renal impairment: No adjustment of starting dose is required on the basis of renal function in patients with mild or moderate renal impairment.
In DTC patients, no adjustment of starting dose is required on the basis of renal function in patients with mild or moderate renal impairment. In patients with severe renal impairment, the recommended starting dose is 14 mg taken once daily. Further dose adjustments may be necessary based on individual tolerability. Patients with end-stage renal disease were not studied, therefore the use of lenvatinib in these patients is not recommended. Refer also to Other special populations under Adverse Reactions.
In RCC patients, no adjustment of starting dose is required on the basis of renal function in patients with mild or moderate renal impairment. In patients with severe renal impairment, the recommended starting dose is 10 mg of lenvatinib taken once daily. Refer to the SmPC for pembrolizumab or everolimus for dosing in patients with renal impairment. Further dose adjustments may be necessary based on individual tolerability. Patients with end-stage renal disease have not been studied, therefore the use of lenvatinib in these patients is not recommended. Refer also to Other special populations under Adverse Reactions.
In the HCC patients, no dose adjustments are required on the basis of renal function in patients with mild or moderate renal impairment. The available data do not allow for a dosing recommendation for patients with HCC and severe renal impairment.
In the EC patients, no dose adjustments are required on the basis of renal function in patients with mild or moderate renal impairment. In patients with severe renal impairment, the recommended dose of LENVIMA is 10 mg in the treatment of endometrial carcinoma. Further dose adjustments may be necessary based on tolerability. Subjects with endometrial carcinoma and end stage renal disease were not studied, therefore the use of LENVIMA in these patients is not recommended.
Elderly population: No adjustment of starting dose is required on the basis of age. Limited data are available on use in patients aged ≥75 years (see also Other special populations under Adverse Reactions).
Paediatric population: Lenvatinib should not be used in children younger than 2 years of age because of safety concerns identified in animal studies (see Pharmacology: Toxicology: Preclinical safety data under Actions). The safety and efficacy of lenvatinib in children aged 2 to <18 years have not yet been established (see Pharmacology: Pharmacodynamics under Actions). No data are available.
Race: No adjustment of starting dose is required on the basis of race (see Pharmacology: Pharmacokinetics under Actions). Limited data are available on use in patients from ethnic origins other than Caucasian or Asian (see also Other special populations under Adverse Reactions).
Body weight below 60 kg in RCC: No adjustment of starting dose is required on the basis of body weight. Limited data are available on treatment with lenvatinib in combination with everolimus in patients with a body weight below 60 kg with RCC (see also Other special populations under Adverse Reactions).
Patients with high ECOG performance status in RCC: Patients with an ECOG (Eastern Cooperative Oncology Group) performance status of 2 or higher were excluded from the RCC study (see Pharmacology: Pharmacodynamics under Actions). Patients with a KPS (Karnofsky Performance Status) <70 were excluded from Study 307 (CLEAR). Benefit-risk in these patients has not been evaluated.
Method of administration: Lenvatinib is for oral use. The capsules should be taken at about the same time each day, with or without food (see Pharmacology: Pharmacokinetics under Actions). Caregivers should not open the capsule, in order to avoid repeated exposure to the contents of the capsule.
Lenvatinib capsules can be swallowed whole with water or administered as a suspension prepared by dispersing the whole capsule(s) in water, apple juice, or milk. The suspension may be administered orally or via a feeding tube. If administered via a feeding tube, then the suspension should be prepared using water (see Preparation and administration of suspension under Cautions for Usage).
If not used at the time of preparation, lenvatinib suspension may be stored in a covered container and must be refrigerated at 2ºC to 8ºC for a maximum of 24 hours. After removal from the refrigerator the suspension should be shaken for approximately 30 seconds before use. If not administered within 24 hours, the suspension should be discarded.