Each hard gelatin capsule contains Pregabalin 75mg/150 mg.
Pregabalin is described chemically as (S)-3-(aminomethyl)-5-methylhexanoic acid. The molecular formula is C8H17NO2 and the molecular weight is 159.23.
Pregabalin is available as a white to off-white crystalline powder.
Excipients/Inactive Ingredients: Lactose monohydrate, Corn starch, Talc.
Pharmacology: Pharmacodynamics: Mechanism of Action: Pregabalin binds with high affinity to the alpha2-delta site (an auxiliary subunit of voltage-gated calcium channels) in central nervous system tissues. Although the mechanism of action of pregabalin has not been fully elucidated, results with genetically modified mice and with compounds structurally related to pregabalin (such as gabapentin) suggest that binding to the alpha2-delta subunit may be involved in pregabalin's anti-nociceptive and anti-seizure effects in animals. In animal models of nerve damage, Pregabalin has been shown to reduce calcium-dependent release of pro-nociceptive neurotransmitters in the spinal cord, possibly by disrupting alpha2-delta containing-calcium channel trafficking and/or reducing calcium currents.
While pregabalin is a structural derivative of the inhibitory neurotransmitter gamma aminobutyric acid (GABA), it does not bind directly to GABAA, GABAB, or benzodiazepine receptors, does not augment GABAA responses in cultured neurons, does not alter rat brain GABA concentration or have acute effects on GABA uptake or degradation. However, in cultured neurons prolonged application of pregabalin increases the density of GABA transporter protein and increases the rate of functional GABA transport. Pregabalin does not block sodium channels, is not active at opiate receptors, and does not alter cyclooxygenase enzyme activity. It is inactive at serotonin and dopamine receptors and does not inhibit dopamine, serotonin, or noradrenaline reuptake.
Pharmacokinetics: Absorption and Distribution: Pregabalin is well absorbed after oral administration. Following oral administration of pregabalin capsules under fasting conditions, peak plasma concentrations occur within 1.5 hours. Pregabalin oral bioavailability is > 90% and is independent of dose. Following single-dose (25 to 300 mg) and multiple-dose (75 to 900 mg/day) administration, maximum plasma concentrations (Cmax) and area under the plasma concentration-time curve (AUC) values increase linearly. Following repeated administration, steady state is achieved within 24 to 48 hours. Multiple-dose pharmacokinetics can be predicted from single-dose data.
The rate of pregabalin absorption is decreased when given with food, resulting in a decrease in Cmax of approximately 25% to 30% and an increase in Tmax to approximately 3 hours. However, administration of pregabalin with food has no clinically relevant effect on the total absorption of pregabalin. Therefore, Pregabalin can be taken with or without food.
Pregabalin does not bind to plasma proteins. The apparent volume of distribution of pregabalin following oral administration is approximately 0.5 L/kg. Pregabalin is a substrate for system L transporter which is responsible for the transport of large amino acids across the blood brain barrier. Although there are no data in humans, pregabalin has been shown to cross the blood brain barrier in mice, rats, and monkeys. In addition, pregabalin has been shown to cross the placenta in rats and is present in the milk of lactating rats.
Metabolism and Elimination: Pregabalin undergoes negligible metabolism in humans. Following a dose of radiolabeled pregabalin, approximately 90% of the administered dose was recovered in the urine as unchanged pregabalin. The N-methylated derivative of pregabalin, the major metabolite of pregabalin found in urine, accounted for 0.9% of the dose.
Pregabalin is eliminated from the systemic circulation primarily by renal excretion as unchanged drug with a mean elimination half-life of 6.3 hours in subjects with normal renal function. Mean renal clearance was estimated to be 67.0 to 80.9 mL/min in young healthy subjects. Because pregabalinis not bound to plasma proteins this clearance rate indicates that renal tubular reabsorption is involved. Pregabalin elimination is nearly proportional to creatinine clearance (CrCl).
Pharmacokinetics in Special Populations: Renal impairment and hemodialysis: Pregabalin clearance is nearly proportional to creatinine clearance (CrCl). Dosage reduction in patients with renal dysfunction is necessary. Pregabalin is effectively removed from plasma by hemodialysis. Following a 4-hour hemodialysis treatment, plasma pregabalin concentrations are reduced by approximately 50%. For patients on hemodialysis, dosing must be modified.
Elderly: Pregabalin oral clearance tended to decrease with increasing age. This decrease in pregabalin oral clearance is consistent with age-related decreases in CrCl. Reduction of pregabalin dose may be required in patients who have age-related compromised renal function.
Pediatric Pharmacokinetics: Pharmacokinetics of pregabalin have not been adequately studied in pediatric patients.
Pregabalin is indicated for: Neuropathic Pain: For the management of neuropathic pain associated with diabetic peripheral neuropathy (DPN) and postherpetic neuralgia (PHN).
Epilepsy: Adjunctive therapy for adult patients with partial-onset seizures.
Fibromyalgia: For management of fibromyalgia in adults.
Generalized Anxiety Disorder: For treatment of Generalized Anxiety Disorder (GAD) in adults.
Pregabalin is given orally with or without food . When discontinuing pregabalin, taper gradually over a minimum of 1 week.
Epilepsy: Pregabalin at doses of 150 to 600 mg/day has been shown to be effective as adjunctive therapy in the treatment of partial onset seizures in adults. Both the efficacy and adverse event profiles of pregabalin have been shown to be dose-related. Administer the total daily dose in two or three divided doses. In general, it is recommended that patients be started on a total daily dose no greater than 150 mg/day (75 mg two times a day, or 50 mg three times a day). Based on individual patient response and tolerability, the dose may be increased to a maximum dose of 600 mg/day.
Because pregabalin is eliminated primarily by renal excretion, adjust the dose in patients with reduced renal function.
The effect of dose escalation rate on the tolerability of pregabalin has not been formally studied.
The efficacy of add-on pregabalin in patients taking gabapentin has not been evaluated in controlled trials. Consequently, dosing recommendations for the use of pregabalin with gabapentin cannot be offered.
Neuropathic Pain (Postherpetic neuralgia): The recommended dose of pregabalin is 75 to 150 mg two times a day, or 50 to 100 mg three times a day (150 to 300 mg/day) in patients with creatinine clearance of at least 60 mL/min. Begin dosing at 75 mg two times a day or 50 mg three times a day (150 mg/day). The dose may be increased to 300 mg/day within 1 week based on efficacy and tolerability. Because pregabalin is eliminated primarily by renal excretion, adjust the dose in patients with reduced renal function.
Patients who do not experience sufficient pain relief following 2 to 4 weeks of treatment with 300 mg/day, and who are able to tolerate pregabalin, may be treated with up to 300 mg two times a day, or 200 mg three times a day (600 mg/day). In view of the dose-dependent adverse reactions and the higher rate of treatment discontinuation due to adverse reactions, reserve dosing above 300 mg/day for those patients who have on-going pain and are tolerating 300 mg daily.
Neuropathic Pain (Diabetic neuropathy): The maximum recommended dose of pregabalin is 100 mg three times a day (300 mg/day) in patients with creatinine clearance of at least 60 mL/min. Begin dosing at 50 mg three times a day (150 mg/day). The dose may be increased to 300 mg/day within 1 week based on efficacy and tolerability. Because pregabalin is eliminated primarily by renal excretion, adjust the dose inpatients with reduced renal function.
In view of the dose-dependent adverse reactions, treatment with doses above 300 mg/day is not recommended.
Fibromyalgia: The recommended dose of pregabalin for fibromyalgia is 300 to 450 mg/day. Begin dosing at 75 mg two times a day (150 mg/day). The dose may be increased to 150 mg two times a day (300 mg/day) within 1 week based on efficacy and tolerability. Patients who do not experience sufficient benefit with 300 mg/day may be further increased to 225 mg two times a day (450 mg/day). Although pregabalin was also studied at 600 mg/day, there is no evidence that this dose confers additional benefit and this dose was less well tolerated. In view of the dose-dependent adverse reactions, treatment with doses above 450 mg/day is not recommended. Because pregabalin is eliminated primarily by renal excretion, adjust the dose in patients with reduced renal function.
Generalized Anxiety Disorder (GAD): The dose range of Pregabalin for Generalized Anxiety Disorder is 150 - 600 mg/day in 2 - 3 divided doses.
Initial dose is 150 mg/day. The dosage may increase based on individual patient response and tolerability at weekly intervals in increments of 150 mg/day up to 300 mg/day after 1 week and up to 450 mg/day in the following week. The maximum dosage of 600 mg/day may be achieved after an additional week. The need for treatment should be reassessed regularly.
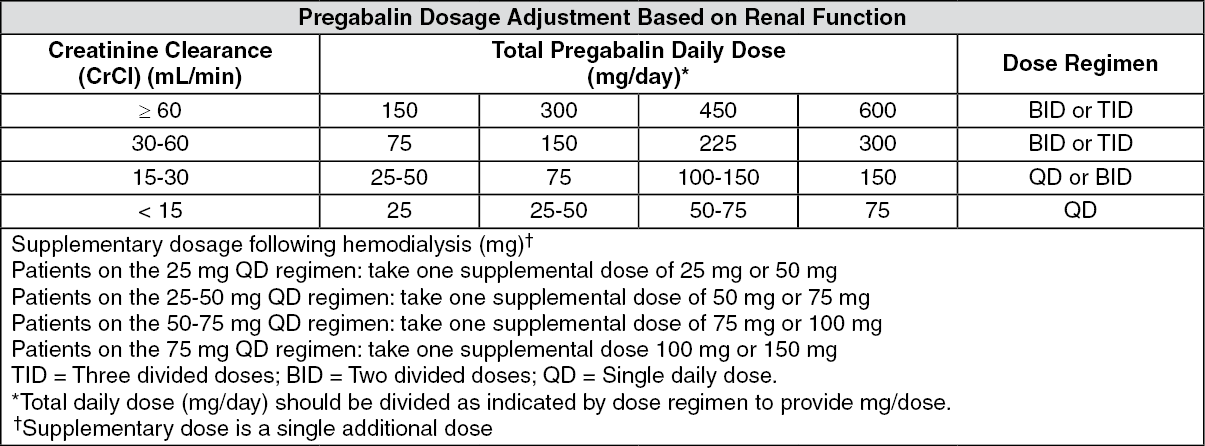
Patients with Renal Impairment: For patients undergoing hemodialysis, adjust the pregabalin daily dose based on renal function. In addition to the daily dose adjustment, administer a supplemental dose immediately following every 4-hour hemodialysis treatment (see Table).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Signs, Symptoms and Laboratory Findings of Acute Over dosage in Humans: There is limited experience with overdose of pregabalin. The highest reported accidental overdose of pregabalin during the clinical development program was 8000 mg, and there were no notable clinical consequences.
Treatment or Management of Overdose: There is no specific antidote for overdose with pregabalin. If indicated, elimination of unabsorbed drug may be attempted by emesis or gastric lavage; observe usual precautions to maintain the airway. General supportive care of the patient is indicated including monitoring of vital signs and observation of the clinical status of the patient. Contact a Certified Poison Control Center for up-to-date information on the management of overdose with pregabalin.
Although hemodialysis has not been performed in the few known cases of overdose, it may be indicated by the patient's clinical state or in patients with significant renal impairment. Standard hemodialysis procedures result in significant clearance of pregabalin (approximately 50% in 4 hours).
Pregabalin is contraindicated in patients with known hypersensitivity to pregabalin or any of its components.
Angioedema: Exercise caution when prescribing pregabalin to patients who have had a previous episode of angioedema. In addition, patients who are taking other drugs associated with angioedema (e.g., angiotensin converting enzyme inhibitors [ACE-inhibitors]) may be at increased risk of developing angioedema.
Hypersensitivity: There have been reports of hypersensitivity in patients shortly after initiation of treatment with pregabalin. Adverse reactions included skin redness, blisters, hives, rash, dyspnea, and wheezing. Discontinue pregabalin immediately in patients with these symptoms.
Withdrawal of Antiepileptic Drugs (AEDs): As with all AEDs, withdraw pregabalin gradually to minimize the potential of increased seizure frequency in patients with seizure disorders. If pregabalin is discontinued, taper the drug gradually over a minimum of 1 week.
Suicidal Behavior and Ideation: Antiepileptic drugs (AEDs), including pregabalin, increase the risk of suicidal thoughts or behavior in patients taking these drugs for any indication. Monitor patients treated with any AED for any indication for the emergence or worsening of depression, suicidal thoughts or behavior, and/or any unusual changes in mood or behavior.
Anyone considering prescribing pregabalin or any other AED must balance the risk of suicidal thoughts or behavior with the risk of untreated illness. Epilepsy and many other illnesses for which AEDs are prescribed are themselves associated with morbidity and mortality and an increased risk of suicidal thoughts and behavior. Should suicidal thoughts and behavior emerge during treatment, the prescriber needs to consider whether the emergence of these symptoms in any given patient may be related to the illness being treated.
Inform patients, their caregivers, and families that pregabalin and other AEDs increase the risk of suicidal thoughts and behavior and advise them of the need to be alert for the emergence or worsening of the signs and symptoms of depression, any unusual changes in mood or behavior, or the emergence of suicidal thoughts, behavior, or thoughts about self-harm. Report behaviors of concern immediately to healthcare providers.
Peripheral Edema: Pregabalin treatment may cause peripheral edema. In short-term trials of patients without clinically significant heart or peripheral vascular disease, there was no apparent association between peripheral edema and cardiovascular complications such as hypertension or congestive heart failure. Peripheral edema was not associated with laboratory changes suggestive of deterioration in renal or hepatic function.
Higher frequencies of weight gain and peripheral edema were observed in patients taking both pregabalin and a thiazolidinedione antidiabetic agent compared to patients taking either drug alone. As the thiazolidinedione class of antidiabetic drugs can cause weight gain and/or fluid retention, possibly exacerbating or leading to heart failure, exercise caution when co-administering pregabalin and these agents.
Because there are limited data on congestive heart failure patients with New York Heart Association (NYHA) Class Ill or IV cardiac status, exercise caution when using pregabalin in these patients.
Dizziness and Somnolence: Pregabalin may cause dizziness and somnolence. Inform patients that pregabalin - related dizziness and somnolence may impair their ability to perform tasks such as driving or operating machinery.
Weight Gain: Pregabalin treatment may cause weight gain.
Abrupt or Rapid Discontinuation: Following abrupt or rapid discontinuation of pregabalin, some patients reported symptoms including insomnia, nausea, headache, and diarrhea. Taper pregabalin gradually over a minimum of 1 week rather than discontinuing the drug abruptly.
Tumorigenic Potential: In standard preclinical in vivo lifetime carcinogenicity studies of pregabalin, an unexpectedly high incidence of hemangiosarcoma was identified in two different strains of mice. The clinical significance of this finding is unknown. Clinical experience during pregabalin's premarketing development provides no direct means to assess its potential for inducing tumors in humans.
In clinical studies across various patient populations, comprising 6396 patient-years of exposure inpatients > 12 years of age, new or worsening-preexisting tumors were reported in 57 patients. Without knowledge of the background incidence and recurrence in similar populations not treated with pregabalin, it is impossible to know whether the incidence seen in these cohorts is or is not affected by treatment.
Ophthalmological Effects: In controlled studies, a higher proportion of patients treated with pregabalin reported blurred vision (7%) than did patients treated with placebo (2%), which resolved in a majority of cases with continued dosing. Less than 1% of patients discontinued pregabalin treatment due to vision-related events (primarily blurred vision).
Although the clinical significance of the ophthalmologic findings is unknown, inform patients to notify their physician if changes in vision occur. If visual disturbance persists, consider further assessment. Consider more frequent assessment for patients who are already routinely monitored for ocular conditions.
Creatine Kinase Elevations: Pregabalin treatment was associated with creatine kinase elevations. Instruct patients to promptly report unexplained muscle pain, tenderness, or weakness, particularly if these muscle symptoms are accompanied by malaise or fever. Discontinue treatment with pregabalin if myopathy is diagnosed or suspected or if markedly elevated creatine kinase levels occur.
Decreased Platelet Count: Pregabalin treatment was associated with a decrease in platelet count. Pregabalin - treated subjects experienced a mean maximal decrease in platelet count of 20 x 103/μL, compared to 11 x103/μL in placebo patients. In the overall database of controlled trials, 2% of placebo patients and 3% of pregabalin patients experienced a potentially clinically significant decrease in platelets, defined as 20% below baseline value and < 150 x 103/μL. A single pregabalin treated subject developed severe thrombocytopenia with a platelet count less than 20 x 103/μL. In randomized controlled trials, pregabalin was not associated with an increase in bleeding-related adverse reactions.
PR Interval Prolongation: Pregabalin treatment was associated with PR interval prolongation. In analyses of clinical trial ECG data, the mean PR interval increase was 3-6 msec at pregabalin doses ≥ 300 mg/day. This mean change difference was not associated with an increased risk of PR increase ≥ 25% from baseline, an increased percentage of subjects with on-treatment PR > 200 msec, or an increased risk of adverse reactions of second or third degree AV block.
Subgroup analyses did not identify an increased risk of PR prolongation in patients with baseline PR prolongation or in patients taking other PR prolonging medications. However, these analyses cannot be considered definitive because of the limited number of patients in these categories.
Effects on ability to drive and operate machines: Pregabalin may have minor or moderate influence on the ability to drive and use machines. It may cause dizziness and somnolence and therefore may influence the ability to drive or use machines. Patients are advised not to drive, operate complex machinery or engage in other potentially hazardous activities until it is known whether this medicinal product affects their ability to perform these activities.
Use in Children: The safety and efficacy of pregabalin in pediatric patients have not been established.
Use in the Elderly: No overall differences in safety and efficacy were observed between these patients and younger patients. Pregabalin is known to be substantially excreted by the kidney, and the risk of toxic reactions to pregabalin may be greater in patients with impaired renal function. Because pregabalin is eliminated primarily by renal excretion, adjust the dose for elderly patients with renal impairment.
Pregnancy: Pregnancy Category C. Increased incidences of fetal structural abnormalities and other manifestations of developmental toxicity, including lethality, growth retardation, and nervous and reproductive system functional impairment, were observed in the offspring of rats and rabbits given pregabalin during pregnancy, at doses that produced plasma pregabalin exposures (AUC) ≥ 5 times human exposure at the maximum recommended dose (MRD) of 600 mg/day.
There are no adequate and well-controlled studies in pregnant women. Use pregabalin during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Labor and Delivery: The effects of pregabalin on labor and delivery in pregnant women are unknown.
Nursing Mothers: It is not known if pregabalin is excreted in human milk; it is, however, present in the milk of rats. Because many drugs are excreted in human milk, and because of the potential for tumorigenicity shown for pregabalin in animal studies, decide whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Clinical studies conducted have reported following adverse events:
Adverse Reactions Most Commonly Leading to Discontinuation: In the pregabalin treatment group, the adverse reactions most frequently leading to discontinuation were dizziness (4%) and somnolence (3%).
Most Common Adverse Reactions: The most common side effects events seen with pregabalin treatment are dizziness, somnolence, headache, ataxia, asthenia, dry mouth, constipation, edema, blurred vision, weight gain, and "thinking abnormal" (primarily difficulty with concentration/attention).
Since pregabalin is predominantly excreted unchanged in the urine, undergoes negligible metabolism in human, does not bind to plasma proteins, its pharmacokinetics are unlikely to be affected by other agents through metabolic interactions or protein binding displacement. In vitro and in vivo studies showed that pregabalin is unlikely to be involved in significant pharmacokinetic drug interactions. Specifically, there are no pharmacokinetic interactions between pregabalin and the following antiepileptic drugs: carbamazepine, valproic acid, lamotrigine, phenytoin, phenobarbital, and topiramate. Concomitant administration of gabapentin with pregabalin did not alter pharmacokinetics of gabapentin although the rate, but not the extent, of the absorption of pregabalin was decreased slightly. Tiagabine does not appear to affect the pharmacokinetics of pregabalin.
Multiple oral doses of pregabalin were co-administered with oxycodone, lorazepam, or ethanol. Although no pharmacokinetic interactions were seen, additive effects on cognitive and gross motor functioning were seen when pregabalin was co-administered with these drugs. No clinically important effects on respiration were seen.
Coadministration with ACE-Inhibitors drug may increase the risk of swelling and hives. Instruct patient to contact health care provider immediately if these signs occur and with thiazolidinedione may lead to additive effect on edema and weight gain and/or fluid retention , possibly exacerbating or leading to heart failure.
Protect from light and moisture.
Store below 30°C in a dry place.
N02BF02 - pregabalin ; Belongs to the class of gabapentinoids. Used to relieve pain and other conditions.
Ligaba hard cap 150 mg
3 × 10's
Ligaba hard cap 75 mg
3 × 10's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
