Pharmacology: Pitavastatin calcium inhibits HMG-CoA reductase, which is a rate-determining enzyme involved with biosynthesis of cholesterol, in a manner of competition with the substrate so that it inhibits cholesterol synthesis in the liver. As a result, the expression of LDL-receptors followed by the uptake of LDL from blood to liver is accelerated, and then the plasma total cholesterol decreases. Furthermore, the sustained inhibition of cholesterol synthesis in the liver decreases VLDL secretion into blood, thus plasma triglyceride levels decrease.
Inhibition of HMG-CoA Reductase: Pitavastatin calcium antagonistically inhibited HMG-CoA reductase in a study by using rat hepatic microsomes. The IC
50 was 6.8 nM (
in vitro).
Inhibition of Cholesterol Synthesis: Pitavastatin calcium inhibited cholesterol synthesis dose-dependently in a study by using human liver cancer derived cells (HepG2) (
in vitro). Moreover, liver-selective inhibition of cholesterol synthesis after the oral administration of pitavastatin calcium was observed (rats).
Plasma Lipid-lowering Effect: Plasma total cholesterol and plasma triglycerides were significantly decreased by oral administration of pitavastatin calcium (dogs, guinea pigs).
Suppressing Effects on Lipid Accumulation and Intimal Thickening: Pitavastatin calcium suppressed the accumulation of cholesteryl ester in macrophages loaded by oxidized-LDL (murine monocyte derived cell line)
in vitro. Furthermore, it significantly suppressed the intimal thickening with a balloon-injured carotid artery through oral administration (rabbits).
Mechanism of Action: Acceleration of LDL-receptor expression: Pitavastatin calcium accelerated the expression of mRNA for LDL-receptor in HepG2 cells so that the binding and the uptake of LDL and the apoB-degradation were increased (
in vitro). Moreover, it accelerated LDL-receptor expression dose-dependently by oral administration (guinea pigs).
VLDL-secretion lowering effect: The secretion of VLDL-triglyceride was significantly decreased by the oral administration of pitavastatin calcium (guinea pigs).
Clinical Studies: The aggregated result of clinical studies (including a double-blind comparative study) by the administration of pitavastatin calcium (1 to 4 mg) once a day for 8-104 weeks in 862 patients with hypercholesterolemia including familial hypercholesterolemia, showed a significant effect on serum lipids improvement. On week 8, the decline of total cholesterol was 28%, that of LDL-cholesterol was 40%, and that of triglyceride was 26% in patients with triglyceride levels ≥150 mg/dL before the administration. No difference was observed between the elderly and the non-elderly subjects in the reduction of total cholesterol.
Furthermore, a long-term administration study (28 to 52 weeks) in patients with hypercholesterolemia indicated sustained and stable serum lipids improvement. Moreover, stable decrease in total cholesterol value and that of LDL-cholesterol value were observed on the long-term administration study (52 to 104 weeks) in patients with familial hypercholesterolemia.
Effect on Blood Steroid Hormones in the Elderly: Oral administration of pitavastatin calcium (2 mg) once a day for 8 weeks in 34 hyperlipidemic patients aged 70 years old or older indicated no significant change on the blood steroid hormones.
Effect on Sugar Metabolism in Hyperlipidemic Patients with Concomitant Diabetes: Oral administration of pitavastatin calcium (2 mg) once a day for 8 weeks in 33 hyperlipidemic patients with concomitant non-insulin dependent diabetes affected a little on the blood sugar control.
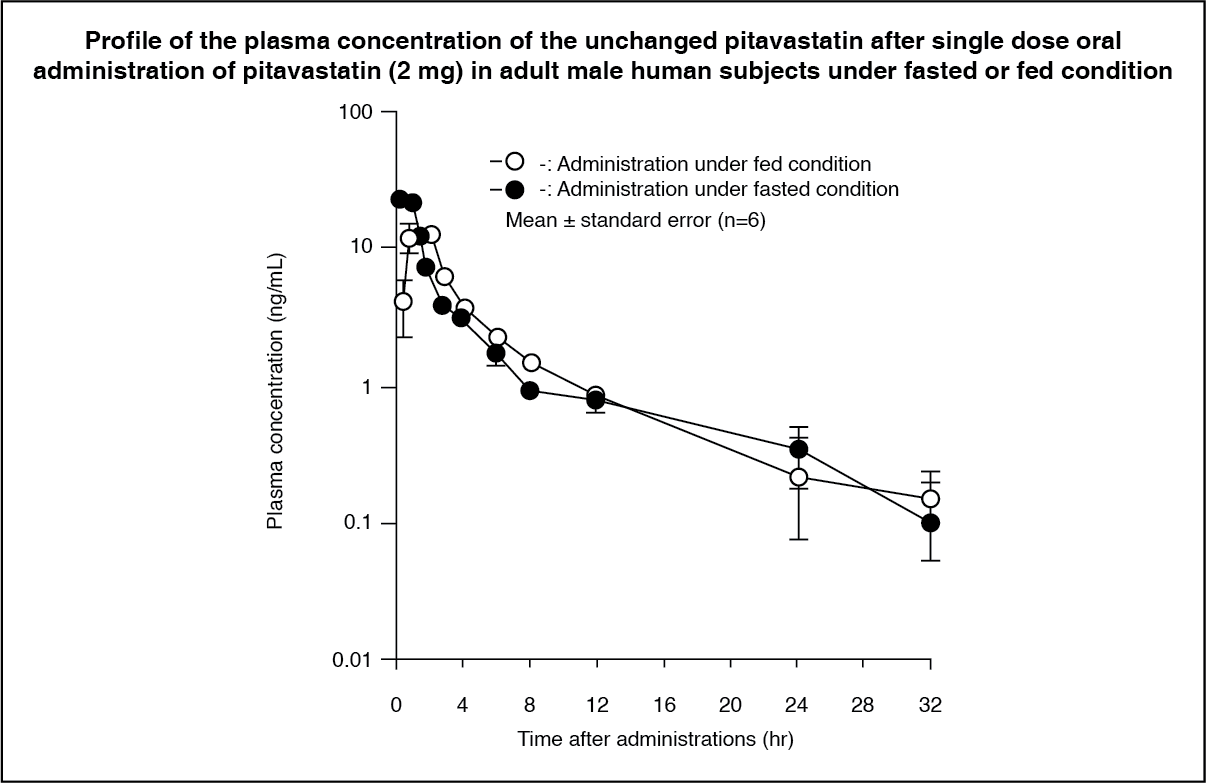
Pharmacokinetics: Pharmacokinetics in Adult Male Human Subjects: Plasma concentration after single dose oral administration: In 6 healthy adult male human subjects, single dose oral administration of pitavastatin calcium (2 mg or 4 mg) was performed under fasted conditions. Unchanged pitavastatin and its lactone, the main metabolite, were mainly found in plasma. The pharmacokinetic parameters after the administration of pitavastatin calcium (2 mg) are shown in the following table.
Effect of food on pharmacokinetics of unchanged pitavastatin: single oral dose administration demonstrated a delay in T
max and decrease in C
max, but no significant difference in AUC. (See Table 1 and Figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Blood concentration after repeated oral administration:
After repeated oral administration of pitavastatin calcium (4 mg) once a day after breakfast for 7 days in 6 healthy adult human male subjects, fluctuation of the pharmacokinetic parameters by repeated administration was slight, and T
½ was around 11 hours. (See Table 2.)
Click on icon to see table/diagram/image
Furthermore, after 5-day repeated oral administration of pitavastatin calcium 2 mg once a day in 6 elderly subjects and 5 non-elderly subjects, no significant difference in the pharmacokinetic parameters in either cohort was observed.
Pharmacokinetics in Patients with Hepatic Dysfunction: Cirrhosis (Data from foreign subjects): Single oral administration of pitavastatin calcium (2 mg) in 12 patients with cirrhosis and 6 healthy adult human subjects was performed. The plasma concentration in the patients classified as Child-Pugh grade A increased by 1.3 times based on C
max and by 1.6 times based on AUC compared with normal hepatic function, and, that in patients classified as Child-Pugh grade B increased by 2.7 times based on C
max and by 3.9 times based on AUC.
Fatty liver disease: Seven-day repeated oral administration of pitavastatin calcium (2 mg) was performed in 6 patients with fatty liver and 6 subjects with normal hepatic function. The effect on the pharmacokinetics was minimal.
Pharmacokinetics in Patients with Renal Dysfunction: Single oral administration of pitavastatin calcium (2 mg) for 7 days in 6 patients with renal dysfunction (serum creatinine ≥1.5 x normal upper limit, to ≤ 3 x normal upper limit) and hypercholesterolemia and 6 patients with normal renal function and hypercholesterolemia was performed. The plasma concentration in the patients with renal dysfunction and hypercholesterolemia increased by 1.7 times based on C
max and by 1.9 times based on AUC compared with patients with normal renal function and hypercholesterolemia.
Drug-drug Interaction: In vitro studies: *An inhibitory study against model substrate of CYP species demonstrated that pitavastatin calcium did not affect the metabolism of tolbutamide, a substrate for CYP2C9 and testosterone, a substrate for CYP3A4. It was demonstrated that an organic anion transporting polypeptide, OATP1B1 (OATP-C/OATP2) is involved in the uptake of pitavastatin into liver, and the uptake of pitavastatin into liver was inhibited by cyclosporine, erythromycin or rifampicin.
Clinical studies: Cyclosporine: Six-day repeated oral administration of pitavastatin calcium (2 mg) in 6 healthy adult male subjects was performed with the administration of cyclosporine (2 mg/kg) 1 hour before the administration of pitavastatin calcium on day 6. The plasma concentration of the unchanged pitavastatin increased by 6.6 times based on C
max and by 4.6 times based on AUC compared with the control value.
Erythromycin (Data from foreign subjects): In 18 healthy adult human subjects, 6-day repeated oral administration of erythromycin (500 mg) four times daily was performed accompanied with a single administration of pitavastatin calcium 4 mg on day 4. As the results, the plasma concentration of pitavastatin increased by 3.6 times based on C
max and by 2.8 times based on AUC compared with pitavastatin alone.
Rifampicin (Data from foreign subjects): In 18 healthy adult human subjects, 15-day repeated oral administration of rifampicin (600 mg) was performed accompanied with 5-day repeated oral administration of pitavastatin calcium (4 mg) once daily on day 11-15. As the results, the plasma concentration of pitavastatin increased by 2.0 times based on C
max and by 1.3 times based on AUC compared with pitavastatin alone.
Plasma concentration by co-administration with fibrates (Data from foreign subjects): In 24 healthy adult human subjects, 6-day repeated oral administration of pitavastatin calcium (4 mg) was performed followed by 1-day washout and then 7-day repeated oral co-administration of pitavastatin calcium (4 mg) and fenofibrate or gemfibrozil. The plasma concentrations of the unchanged pitavastatin (AUC) increased by 1.2 times in case of fenofibrate and 1.4 times in case of gemfibrozil.
Warfarin (Data from foreign subjects): In 23 healthy adult male subjects, 21-day repeated oral administration of warfarin (individually titrated dose) on day 1-21 was performed accompanied with 9-day repeated oral administration of pitavastatin calcium (4 mg) once daily on day 14-22. As the results, the plasma concentration of R-warfarin increased by 1.034 times based on C
max and by 1.066 times based on AUC, the plasma concentration of S-warfarin increased by 1.033 times based on C
max and by 1.058 times based on AUC compared with warfarin alone. Pitavastatin calcium had no significant pharmacokinetic interaction with R- and S- warfarin. The steady-state pharmacodynamics (prothrombin time [PT] and international normalized ratio [INR]) of warfarin in healthy subject were unaffected by the co-administration of pitavastatin 4 mg daily. However, patients receiving warfarin should have their PT and INR monitored when pitavastatin is added to their therapy.
Darunavir/Ritonavir (Data from foreign subjects): In 27 healthy adult human subjects, pitavastatin 4 mg was administered once daily (days 1-5 and days 12-16), darunavir/ritonavir 800mg/100mg was administered (days 6-16). As the results, the plasma concentration of pitavastatin decreased by 0.96 times based on C
max and by 0.74 times based on AUC compared with pitavastatin alone.
Lopinavir/Ritonavir (Data from foreign subjects): In 23 healthy adult human subjects, pitavastatin 4 mg was administered once daily (days 1-5 and days 20-24), lopinavir/ritonavir 400mg/100mg was administered (days 9-24). As the results, the plasma concentration of pitavastatin decreased by 0.99 (58.2/58.6) times based on C
max and by 0.83 (113.9/136.8) times based on AUC compared with pitavastatin alone. The effect on exposures when pitavastatin and lopinavir/ritonavir are coadministered was minimal. Concomitant use of pitavastatin and lopinavir/ritonavir was safe and well tolerated.
Atazanavir (Data from foreign subjects): In 17 healthy adult human subjects, 9-day repeated oral administration of atazanavir (300 mg) was performed accompanied with 5-day repeated oral administration of pitavastatin calcium (4 mg) once daily on day 5-9. As the results, the plasma concentration of pitavastatin increased by 1.6 times based on C
max and by 1.3 times based on AUC compared with pitavastatin alone. When atazanavir is co-administered with pitavastatin there is a small increase in maximum concentrations of and exposure to both pitavastatin and atazanavir compared to when they are administered alone. In this study these changes in pharmacokinetics did not appear to affect any safety parameters measured.
Urinary Excretion: After single oral administration of pitavastatin calcium 2 mg or 4 mg in 6 healthy adult male humans, the urinary excretion rate of the unchanged pitavastatin was less than 0.6%, and that of its lactone metabolite was less than 1.3%. The total excretion rate of the unchanged pitavastatin and its lactone was less than 2% of the dose.
After 7-day repeated oral dose of pitavastatin (4 mg) once a day in 6 healthy adult male human subjects, the urinary excretion of the unchanged pitavastatin and its lactone metabolite showed no increase during the period from the first administration until day 7, and decreased rapidly after completion of administration.
Metabolism: Pitavastatin calcium was metabolized by cyclization to its lactone, β-oxidation on the side-chain, hydroxylation of the quinoline ring and glucuronate or taurine conjugation. The main route of excretion was rectally (rats, dogs).
In human subjects, the unchanged pitavastatin and its lactone metabolite as the main metabolite were mainly observed in blood, and the other metabolites such as propionate derivative and 8-hydroxide were minimally observed. Meanwhile, the unchanged pitavastatin, its lactone, dehydro-lactone, 8-hydroxide and these conjugates were minimally observed in urine.
Drug-metabolizing Enzymes: Pitavastatin calcium was minimally metabolized in study using human hepatic microsomes, and its 8-hydroxide occurred mainly by CYP2C9 metabolism (
in vitro).
Plasma Protein Binding Rate: Plasma protein binding rate of pitavastatin calcium was as high as 99.5% to 99.6% with human plasma or 4% human serum albumin and 94.3% to 94.9% with 0.06% human α
1-acid glycoprotein (
in vitro).


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image


 Sign Out
Sign Out