


 Sign Out
Sign Out

Therapy with edoxaban in NVAF patients should be continued long term.
Treatment of DVT, treatment of PE and prevention of recurrent DVT and PE (VTE): The recommended dose is 60 mg edoxaban once daily following initial use of parenteral anticoagulant for at least 5 days (see PHARMACOLOGY: Pharmacodynamics under Actions). Edoxaban and initial parenteral anticoagulant should not be administered simultaneously.
The duration of therapy for treatment of DVT and PE (venous thromboembolism (VTE)), and prevention of recurrent VTE should be individualised after careful assessment of the treatment benefit against the risk for bleeding (see Precautions). Short duration of therapy (at least 3 months) should be based on transient risk factors (e.g. recent surgery, trauma, immobilisation) and longer durations should be based on permanent risk factors or idiopathic DVT or PE.
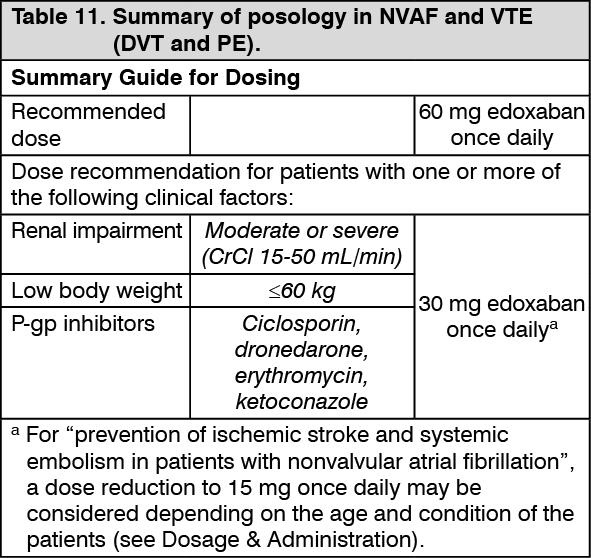
For NVAF and VTE the recommended dose is 30 mg edoxaban once daily in patients with one or more of the following clinical factors: Moderate or severe renal impairment (creatinine clearance (CrCl) 15 - 50 mL/min); Low body weight ≤ 60 kg; Concomitant use of the following P-glycoprotein (P-gp) inhibitors: ciclosporin, dronedarone, erythromycin, or ketoconazole.
NVAF in elderly patients with a high risk of hemorrhage depending on the age and condition (see as follows) dose may be reduced to 15 mg edoxaban once daily. (See Table 11.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMissed dose: If a dose of edoxaban is missed, the dose should be taken immediately and then be continued the following day with the once-daily intake as recommended. The patient should not take double the prescribed dose on the same day to make up for a missed dose.
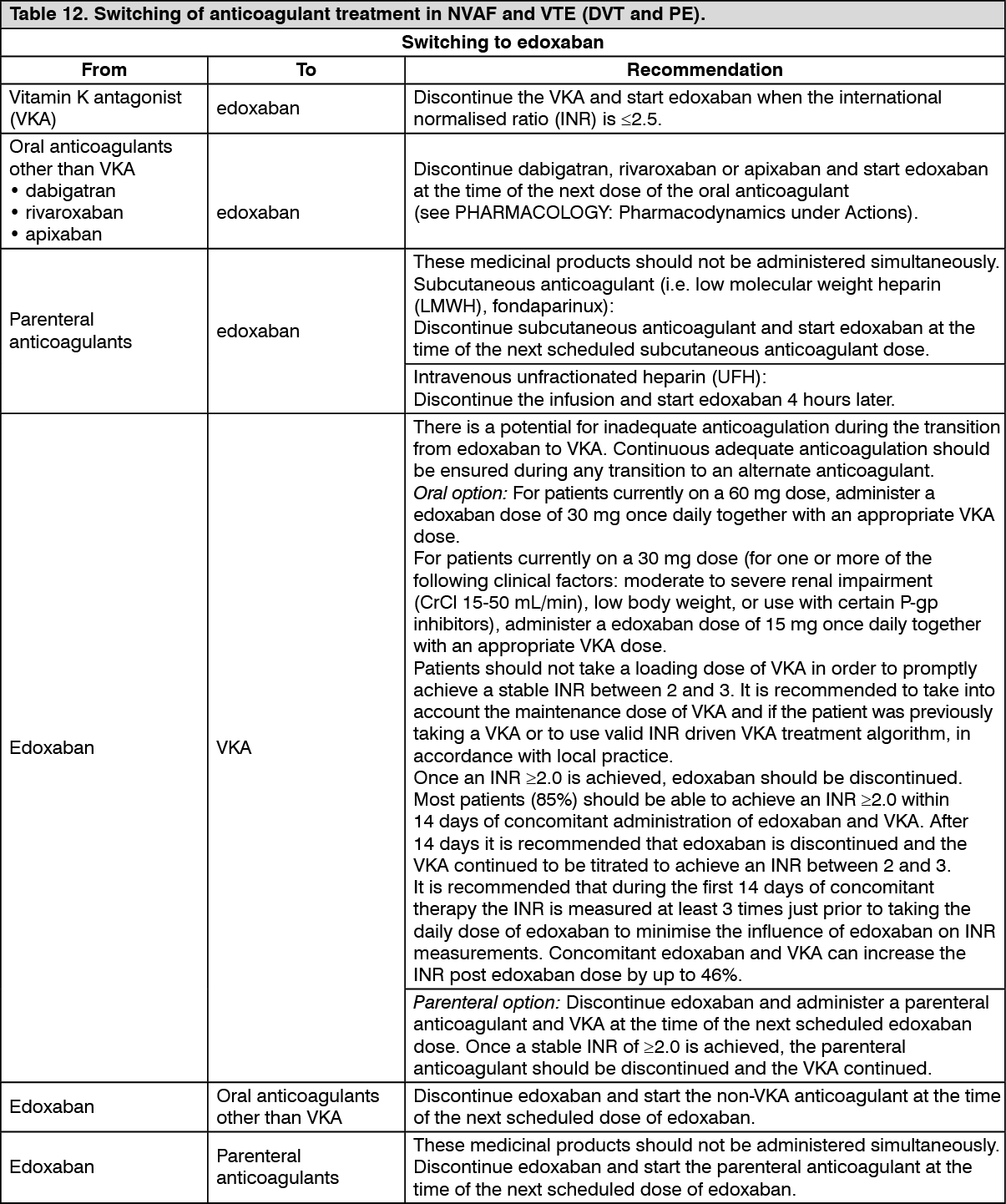
Switching to and from edoxaban: Continued anticoagulant therapy is important in patients with NVAF and VTE. There may be situations that warrant a change in anticoagulation therapy (Table 12). (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSpecial populations: Elderly population (see PHARMACOLOGY: Pharmacodynamics and Pharmacokinetics under Actions).
Prevention of ischemic stroke and systemic embolism in patients with nonvalvular atrial fibrillation: For elderly patients (roughly 80 years of age or older) who meet both the following criteria, the appropriateness of administration of edoxaban should be carefully determined, taking therapeutic benefits and the risk of hemorrhage into account. Oral administration of once daily edoxaban 15 mg may be considered if the administration is necessary.
1. Having at least one of the following hemorrhagic diatheses: History of hemorrhage in important organs, including intracranial hemorrhage, intraocular hemorrhage, and hemorrhage in the gastrointestinal tract; Low body weight (≤ 45 kg); Creatinine clearance level of ≥ 15 mL/min and < 30 mL/min; Regular use of nonsteroidal anti-inflammatory drugs; Use of antiplatelet drugs.
2. Unable to receive a usual dose of edoxaban or an approved dose of other oral anticoagulants because of a risk of hemorrhage.
Renal impairment: Renal function should be assessed in all patients by calculating the CrCl prior to initiation of treatment with edoxaban to exclude patients with end stage renal disease (e.g. CrCl < 15 mL/min), to use the correct edoxaban dose in patients with CrCl 15 - 50 mL/min (30 mg once dailya), in patients with CrCl > 50 mL/min (60 mg once daily) and when deciding on the use of edoxaban in patients with increased creatinine clearance (see Precautions).
Renal function should also be assessed when a change in renal function is suspected during treatment (e.g. hypovolaemia, dehydration, and in case of concomitant use of certain medicinal products).
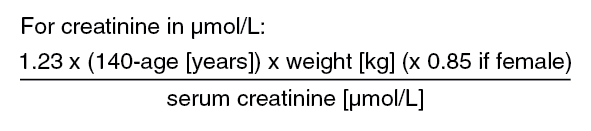
The method used to estimate renal function (CrCl in mL/min) during the clinical development of edoxaban was the Cockcroft-Gault method. The formula is as follows: See Equations 1 and 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image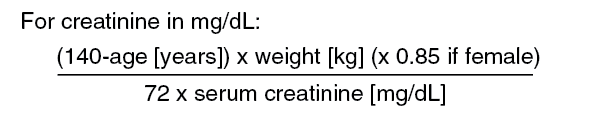 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThis method is recommended when assessing patients' CrCl prior to and during edoxaban treatment.
In patients with mild renal impairment (CrCl > 50 - 80 mL/min), the recommended dose is 60 mg edoxaban once daily.
In patients with moderate or severe renal impairment (CrCl 15 - 50 mL/min), the recommended dose is 30 mga edoxaban once daily (see PHARMACOLOGY: Pharmacokinetics under Actions).
a For "prevention of stroke and systemic embolism in adult patients with nonvalvular atrial fibrillation" with creatinine clearance level of ≥15mL/min and <30 mL/min, a dose reduction to 15 mg once daily may be considered depending on the age and condition of patients (see Dosage & Administration).
In patients with end stage renal disease (ESRD) (CrCl < 15 mL/min) or on dialysis, the use of edoxaban is not recommended (see Precautions and PHARMACOLOGY: Pharmacokinetics under Actions).
Hepatic impairment: Edoxaban is contraindicated in patients with hepatic disease associated with coagulopathy and clinically relevant bleeding risk (see Contraindications).
In patients with severe hepatic impairment edoxaban is not recommended (see Precautions and PHARMACOLOGY: Pharmacokinetics under Actions).
In patients with mild to moderate hepatic impairment the recommended dose is 60 mg edoxaban once daily (see PHARMACOLOGY: Pharmacokinetics under Actions). Edoxaban should be used with caution in patients with mild to moderate hepatic impairment (see Precautions).
Patients with elevated liver enzymes (alanine aminotransferase (ALT) or aspartate transaminase (AST) >2x upper limit of normal (ULN)) or total bilirubin ≥ 1.5x ULN were excluded in clinical studies. Therefore edoxaban should be used with caution in this population (see Precautions and PHARMACOLOGY: Pharmacokinetics under Actions). Prior to initiating edoxaban, liver function testing should be performed.
Body weight: For patients with body weight ≤ 60 kg, the recommended dose is 30 mg Edoxaban once daily (see PHARMACOLOGY: Pharmacokinetics under Actions). For "prevention of stroke and systemic embolism in adult patients with nonvalvular atrial fibrillation" with body weight ≤ 45 kg, a dose reduction to 15 mg once daily may be considered depending on the age and condition of patients (see Dosage & Administration).
Gender: No dose reduction is required (see PHARMACOLOGY: Pharmacokinetics under Actions).
Concomitant use of edoxaban with P-glycoprotein (P-gp) inhibitors: In patients concomitantly taking edoxaban and the following P-gp inhibitors: ciclosporin, dronedarone, erythromycin, or ketoconazole, the recommended dose is 30 mg edoxaban once daily (see Interactions).
No dose reduction is required for concomitant use of amiodarone, quinidine or verapamil (see Interactions).
The use of edoxaban with other P-gp inhibitors including HIV protease inhibitors has not been studied.
Paediatric population: The safety and efficacy of edoxaban in children and adolescents less than 18 years of age have not been established. No data are available.
Patients undergoing cardioversion: Edoxaban can be initiated or continued in patients who may require cardioversion. For transoesophageal echocardiogram (TEE) guided cardioversion in patients not previously treated with anticoagulants, Edoxaban treatment should be started at least 2 hours before cardioversion to ensure adequate anticoagulation (see PHARMACOLOGY: Pharmacodynamics and Pharmacokinetics under Actions). Cardioversion should be performed no later than 12 hours after the dose of edoxaban on the day of the procedure.
For all patients undergoing cardioversion: Confirmation should be sought prior to cardioversion that the patient has taken edoxaban as prescribed. Decisions on initiation and duration of treatment should follow established guidelines for anticoagulant treatment in patients undergoing cardioversion.
Method of administration: For oral use.
Edoxaban can be taken with or without food (see PHARMACOLOGY: Pharmacokinetics under Actions).
For patients who are unable to swallow whole tablets, edoxaban tablets may be crushed and mixed with water or apple puree and immediately administered orally (see PHARMACOLOGY: Pharmacokinetics under Actions).
Alternatively, edoxaban tablets may be crushed and suspended in a small amount of water and immediately delivered through a gastric tube after which it should be flushed with water (see PHARMACOLOGY: Pharmacokinetics under Actions). Crushed edoxaban tablets are stable in water and apple puree for up to 4 hours.