Pregabalin is given orally with or without food. When discontinuing pregabalin, taper gradually over a minimum of 1 week.
Neuropathic pain: The maximum recommended dose of pregabalin is 100 mg three times a day (300 mg/day) in patients with creatinine clearance of at least 60 mL/min. Dosing should begin at 50 mg three times a day (150 mg/day) and may be increased to 300 mg/day within 1 week based on efficacy and tolerability. Because pregabalin is eliminated primarily by renal excretion, the dose should be adjusted for patients with reduced renal function.
Although pregabalin was also studied at 600 mg/day, there is no evidence that this dose confers additional significant benefit and this dose was less well tolerated. In view of the dose dependent adverse effects, treatment with doses above 300 mg/day are not recommended.
Epilepsy: Pregabalin at doses of 150 to 600 mg/day has been shown to be effective as adjunctive therapy in the treatment of partial onset seizures in adults. The total daily dose should be divided and given either two or three times daily. Both the efficacy and adverse event profiles of pregabalin have been shown to be dose related. In general, it is recommended that patients be started on a total daily dose no greater than 150 mg/day (75 mg two times a day, or 50 mg three times a day). Based on individual patient response and tolerability, the dose may be increased to a maximum dose of 600 mg/day.
The effect of dose escalation rate on the tolerability of pregabalin has not been formally studied.
The efficacy of add on pregabalin in patients taking gabapentin has not been evaluated in controlled trials.
Consequently, dosing recommendations for the use of pregabalin with gabapentin cannot be offered.
Patients with Renal Impairment: In view of dose dependent adverse events and since pregabalin is eliminated primarily by renal excretion, the dose should be adjusted in patients with reduced renal function. Dosage adjustment in patients with renal impairment should be based on CL
cr , as indicated in following table. To use this dosing table, an estimate of the patient's CL
cr in mL/min is needed. CL
cr in mL/min may be estimated from serum creatinine (mg/dL) determination using the Cockcroft and Gault equation: See Equation.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
For patients undergoing hemodialysis, pregabalin daily dose should be adjusted based on renal function. In addition to the daily dose adjustment, a supplemental dose should be given immediately following every 4-hour hemodialysis treatment as shown in table below: See Table.
Click on icon to see table/diagram/image
Elderly: Pregabalin oral clearance tended to decrease with increasing age. This decrease in pregabalin oral clearanceis consistent with age related decreases in Cl
cr.
No overall differences in safety and efficacy were observed between these patients and younger patients. Even though the incidence of adverse events did not increase with age, greater sensitivity of some older individuals cannot be ruled out. Pregabalin is known to be substantially excreted by the kidney, and the risk of toxic reactions to pregabalin may be greater in patients with impaired renal function.
Because pregabalin is eliminated primarily by renal excretion, the dose should be adjusted for elderly patients with renal impairment.
Pediatric use: The safety and efficacy of pregabalin in pediatric patients have not been established.
The most commonly reported adverse effects with pregabalin are asthenia, accidental injury, back pain, chest pain, face edema, dry mouth, constipation, flatulence, peripheral edema, weight gain, edema, hypoglycemia, dizziness, somnolence, neuropathy, ataxia, vertigo, confusion, euphoria, incoordination, abnormal thinking, tremor, abnormal gait, amnesia, nervousness, dyspnea, blurry vision, abnormal vision, infection, headache, pain, flu syndrome, vomiting, myasthenia, speech disorder, bronchitis, diplopia, eye disorder, urinary incontinence, twitching, myoclonus, increased appetite, irritability, memory impairement, disturbance in attention, erectile dysfunction and fatigue.
Other infrequently reported adverse effects are abdominal pain, allergic reaction, fever, abscess, cellulitis, chills, malaise, neck rigidity, overdose, pelvic pain, photosensitivity reaction, suicide attempt, deep thrombophlebitis, heart failure, hypotension, postural hypotension, retinal vascular disorder, syncope, gastroenteritis, cholecystitis, cholelithiasis, colitis, dysphagia, esophagitis, gastritis, gastrointestinal hemorrhage, melena, mouth ulceration, pancreatitis, rectal hemorrhage, tongue edema, ecchymosis, anemia, eosinophilia, hypochromic anemia, leukocytosis, leukopenia, lymphadenopathy, thrombocytopenia, arthralgia, leg cramps, myalgia, arthrosis, depersonalization, hypertonia, hypesthesia, decreased libido, nystagmus, paresthesia, stupor, abnormal dreams, agitation, apathy, aphasia, circumoral paresthesia, dysarthria, hallucinations, hostility, hyperalgesia, hyperesthesia, hyperkinesia, hypotonia, increased libido, neuralgia, pruritus, alopecia, dry skin, eczema, skin ulcer, urticaria, vesiculobullous rash, conjunctivitis, otitis media, tinnitus, abnormality of accommodation, blepharitis, dry eyes, eye hemorrhage, hyperacusis, photophobia, retinal edema, taste loss, taste perversion, anorgasmia, impotence, urinary frequency, abnormal ejaculation, albuminuria, amenorrhea, dysmenorrhea, dysuria, hematuria, kidney calculus, leukorrhea, menorrhagia, metrorrhagia, nephritis, oliguria, urinary retention, anorexia, panic attack, restlessness, depression, depressed mood, mood swings, insomnia exacerbated, word finding difficulty, psychomotor hyperactivity, ageusia, dyskinesia, cognitive disorder, hyporeflexia, burning sensation, eye swelling, eye pain, asthenopia, increased lacrimation, tachycardia, flushing, hot flushes, nasal dryness, abdominal distension, gastrooesophageal reflux disease, salivary hypersecretion, sweating, joint swelling, muscle cramp, pain in limb, muscle stiffness, sexual dysfunction, thirst, increased blood creatine phosphokinase, increased alanine aminotransferase, increased aspartate aminotransferase and decreased platelet count.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image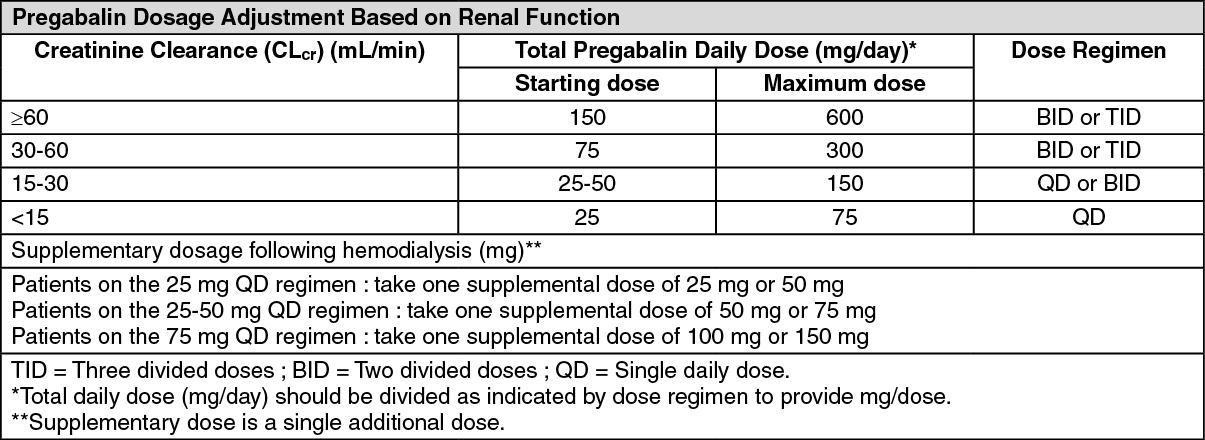 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
