Pharmacotherapeutic group: Cephalosporins and related substances.
ATC code: J01DA.
Pharmacology: 100 mg tablet and Fine granules for oral susp: Antibacterial activity: Cefditoren pivoxil is metabolized into cefditoren upon absorption from the intestinal wall and shows its antibacterial activity.
Cefditoren exerts antibacterial activity
in vitro against a wide spectrum of gram-positive and gram-negative bacteria. Its activity against gram-positive bacteria including
Staphylococcus sp. and
Streptococcus sp. such as
Streptococcus pneumoniae as well as against gram-negative bacteria including
E. coli,
B. catarrhalis, Klebsiella sp.,
Proteus sp. and
H. influenzae and anaerobic bacteria including
Peptostreptococcus sp.,
P. acnes and
Bacteroides sp., is particularly noteworthy.
In vitro, cefditoren was stable to β-lactamase produced by various bacteria. It also shows strong antibacterial activity against strains that produce β-lactamase.
Mechanism of action: Cefditoren inhibits the synthesis of bacterial cell wall. It has high affinity to penicillin binding proteins (PBPs) in various bacteria, showing a bactericidal effect.
Therapeutic efficacy on experimental infections: Cefditoren pivoxil demonstrated excellent therapeutic efficacy on experimental infections by
Staphylococcus aureus, S. pneumoniae, E. coli, Klebsiella pneumoniae and
Proteus sp., in mice. Its therapeutic efficacy on the infections by β-lactamase - producing strains was equivalent or superior to similar drugs.
Pharmacodynamics: 200 mg tablet: Mode of action: Cefditoren exerts its antibacterial action by inhibiting bacterial cell wall synthesis due to its affinity for penicillin-binding proteins (PBPs).
Pharmacokinetic/Pharmacodynamic relationship: With a dosage of 200 mg twice daily, plasma concentrations exceed the minimum inhibitory concentrations (MIC
90) for
Moraxella catarrhalis, Haemophilus influenzae, Streptococcus pyogenes and penicillin-susceptible
Streptococcus pneumoniae strains for at least 50% of the dose interval. The dosage of 400 mg twice daily, also provides a time above the minimum inhibitory concentrations which is enough to exceed the MIC
90 of
Streptococcus pneumoniae resistant to penicillin.
Mechanisms of resistance:
Bacterial resistance to cefditoren may be due to one or more of the following mechanisms: Hydrolysis by beta-lactamases. Cefditoren may be efficiently hydrolysed by certain of the extended-spectrum beta-lactamases (ESBLs) and by the chromosomally encoded (AmpC) beta-lactamases that may be induced or stably derepressed in certain aerobic gram-negative bacterial species.
Reduced affinity of penicillin-binding proteins for cefditoren.
Outer membrane impermeability, which restricts access of cefditoren to penicillin-binding proteins in gram-negative organisms.
Active substance efflux pumps.
More than one of these mechanisms of resistance may co-exist in a single bacterial cell. Depending on the mechanism(s) present, bacteria may express cross-resistance to several or all other beta-lactams and/or antibacterial active substances of other families.
Gram-negative micro-organisms containing inducible chromosomally encoded beta-lactamases, like
Enterobacter spp.,
Serratia spp.,
Citrobacter spp., and
Providencia spp., should be regarded as resistant for cefditoren pivoxil in spite of apparent in vitro susceptibility.
Breakpoints: The recommended MIC breakpoints for cefditoren, which allow susceptible micro-organisms to be distinguished from intermediately susceptible micro-organisms, and intermediately susceptible organisms from resistant micro-organisms are: Susceptible ≤ 0.5 µg/ml, Resistant ≥ 2 µg/ml (or > 1 µg/ml according to recent criteria).
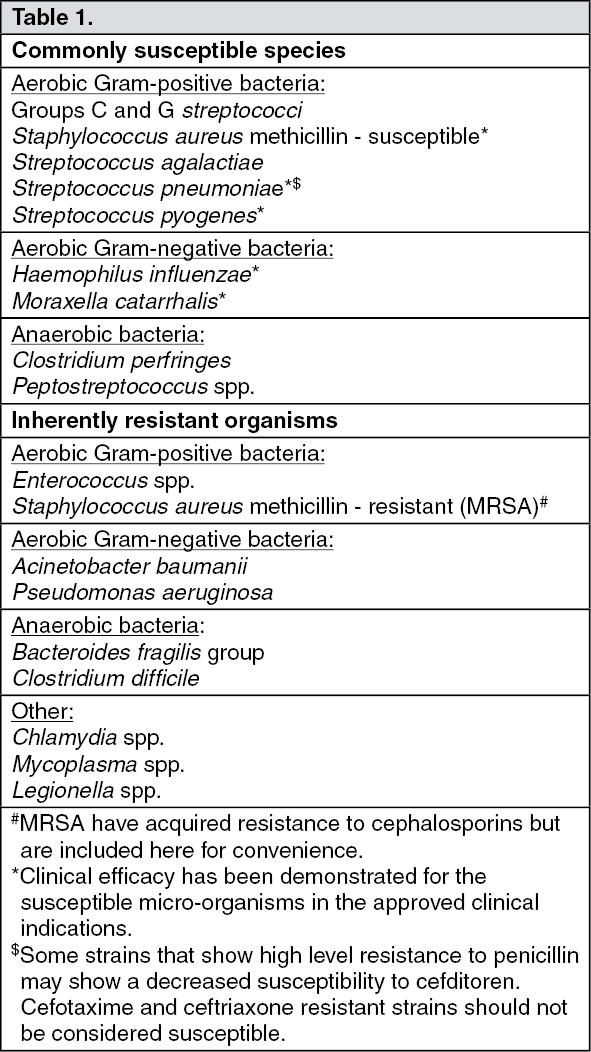
The prevalence of acquired resistance may vary geographically and with time for selected species and local information on resistance is desirable, particularly when treating severe infections. As necessary, expert advice should be sought when the local prevalence of resistance is such that the utility of the agent in at least some types of infections is questionable. (See Table 1.)
 Click on icon to see table/diagram/image
Clinical Studies:
Click on icon to see table/diagram/image
Clinical Studies: Fine granules for oral susp: Clinical results of MEIACT granules, that has been confirmed to be bioequivalent to this product, were as follows. Clinical trials were conducted in medical institutions nationwide to investigate the efficacy of MEIACT granules. The results obtained in 443 patients treated with this product are summarized as follows: Superficial suppurative diseases:
The efficacy rate was 93.1% (54/58) in patients with impetigo contagiosa, phlegmon, lymphadenitis (lymphangitis), suppurative perionychia (paronychia) and subcutaneous abscess.
Infections in surgical fields: The efficacy rate was 100% (1/1) in a patient with perianal abscess.
Respiratory tract infections:
The efficacy rate was 97.9% (277/283) in patients with pharyngolaryngitis (throat abscess), acute bronchitis, tonsillitis (peritonsillitis, peritonsillar abscess) and pneumonia.
Urinary tract infections: The efficacy rate was 94.6% (35/37) in patients with urinary tract infections (pyelonephritis and cystitis).
Scarlet fever: The efficacy rate was 100% (36/36) in patients with scarlet fever.
Pertussis:
The efficacy rate was 100% (11/11) in patients with pertussis.
Otorhinologic infections: The efficacy rate was 100% (18/18) in patients with otitis media and sinusitis.
Pharmacokinetics: Absorption and Distribution: Blood concentration: 100 mg tablet: The serum concentrations (Figure 1) and pharmacokinetic parameters (Table 2) of Cefditoren after oral administration of 100 or 200 mg to healthy adults after meals demonstrated dose dependency. Absorption was better when administered after meals than when given at fasting. (See Figure 1 and Table 2.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Fine granules: When cefditoren was orally administered to pediatric patients with normal renal function at doses of 3 mg/kg or 6 mg/kg after meals, the serum concentrations (Figure 2) and pharmacokinetic parameters (Table 3) of cefditoren demonstrated dose dependency. (See Figure 2 and Table 3.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Body fluid and tissue concentrations: 100 mg tablet: The drug transferred to the sputum, tonsillar tissue, mucous membrane of maxillary sinus, skin tissue, mammary gland tissue, gallbladder tissue, vagina, uterine neck, tarsal gland tissue and wound after tooth extraction. No transfer to the milk was noted.
Fine granules: The drug transferred to the sputum, tonsillar tissue, mucous membrane of maxillary sinus and skin tissue of patients.
Protein binding: 100 mg tablet and Fine granules for oral susp:
In vitro, binding rate to human serum protein determined by ultrafiltration method was 91.5% at concentration of 25 μg/mL.
Metabolism and excretion: 100 mg tablet: Cefditoren pivoxil is metabolized upon absorption and becomes cefditoren which has antibacterial activity, and pivalic acid. Pivalic acid is conjugated with carnitine and excreted into urine as pivaloyl carnitine. Cefditoren is hardly metabolized and is excreted mainly into urine and bile.
100 mg tablet: The urinary excretion rate (0-24 hours) of cefditoren upon oral administration after meals at doses of 100 mg and 200 mg to healthy adults was about 20%. No accumulation of the drug was observed after continuous administration (200 mg x 3 times/day, for 8 days).
Fine granules for oral susp: The urinary excretion rate (0-8 hours) of cefditoren upon oral administration after meals at doses of 3 and 6 mg/kg to pediatric patients with normal renal function were about 20 and 17%, respectively.
Serum concentration and urinary excretion in patients with renal function disorder: 100 mg tablet and Fine granules for oral susp: The serum concentrations (Figure 3) and pharmacokinetic parameters (Table 4) of cefditoren are as follows. Oral administration of 200 mg to adult patients with renal function disorder or to those receiving artificial dialysis after meals demonstrated higher levels in all the cases, showing delay in T
½ in parallel with degree of renal function disorder. (See Figure 3 and Table 4.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Urinary excretion rate lowered in parallel with degree of renal function disorder, showing delay in excretion.
200 mg tablet: Absorption: Following oral administration, cefditoren pivoxil is absorbed in the gastrointestinal tract and is hydrolysed to cefditoren by the action of esterases. The absolute bioavailability of orally administered cefditoren is approximately 15-20%.
The presence of food in the gastrointestinal tract increases the absorption of cefditoren pivoxil, with the C
max and the AUC approximately 50% and 70% higher compared to fasting values.
A 200 mg dose administered with food gives a mean C
max of 2.6 µg/ml after approximately 2.5 hours, while a 400 mg dose gives a mean C
max value of 4.1 µg/ml in approximately the same time period.
Distribution: Plasma protein binding to cefditoren is 88%.
The volume of distribution at steady state is not significantly different from that calculated after a single dose administration and is relatively independent of the administered dose (40-65 litres).
After a single dose administration of 400 mg, penetration in bronchial mucosa and in bronchial secretion was 60% and 20% respectively of the plasma concentration. After the same dose, cefditoren concentrations in skin blister fluid reached 40% and 56% of plasma AUC after 8 and 12 hours, respectively.
Metabolism/Elimination: Following multiple dose administration, pharmacokinetic parameters were similar to those obtained after single dose administration, with no accumulation detected.
Up to 18% of the administered dose of cefditoren is recovered by excretion in urine without being metabolised.
The plasma elimination half-life of cefditoren is between 1 and 1.5 hours. Total clearance adjusted for bioavailability is from 25-30 l/h, while renal clearance is approximately 80-90 ml/min. Studies with labelled cefditoren in healthy volunteers suggest that the non-absorbed fraction is eliminated in faeces, where the majority of the administered cefditoren appears as inactive metabolites.
Cefditoren pivoxil is not detected in faecal extracts or in urine. The pivalate portion is eliminated through renal excretion as the conjugated pivaloylcarnitine.
Special populations: Gender: Pharmacokinetics of cefditoren pivoxil do not show clinically relevant differences between males and females.
Elderly: Plasma levels of cefditoren in elderly subjects (over 65 years) show C
max and AUC that are approximately 26% and 33% higher than in younger adults. However, no dose adjustment is required except in cases of advanced hepatic and/or renal insufficiency.
Renal insufficiency: After multiple doses of cefditoren pivoxil 400 mg to patients with moderate to severe renal impairment, C
max was 2-fold and AUC between 2.5 and 3-fold than those observed in normal healthy volunteers (see Dosage & Administration). There are no data available for patients undergoing dialysis.
Hepatic insufficiency: In mild hepatic insufficiency (Child-Pugh A) to moderate hepatic insufficiency (Child-Pugh B), multiple doses of 400 mg cefditoren pivoxil gave a slight increase in pharmacokinetic parameters compared to normal subjects. No data are available in patients with severe insufficiency (Child-Pugh C) (See Dosage & Administration).
Toxicology: Preclinical safety data: 200 mg tablet:
Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity and toxicity to reproduction.
Studies to evaluate the carcinogenic potential of cefditoren pivoxil have not been performed.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image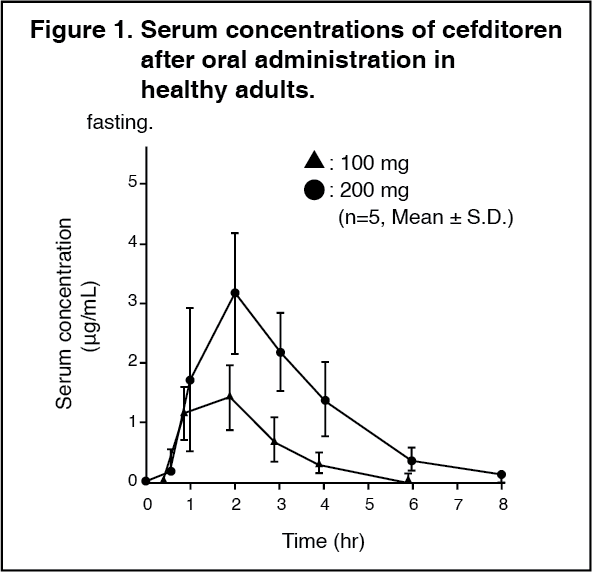 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image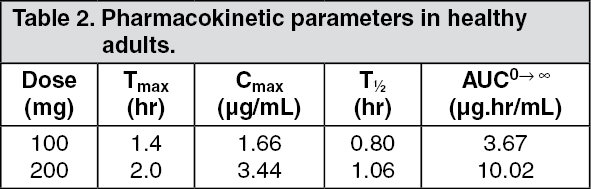 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image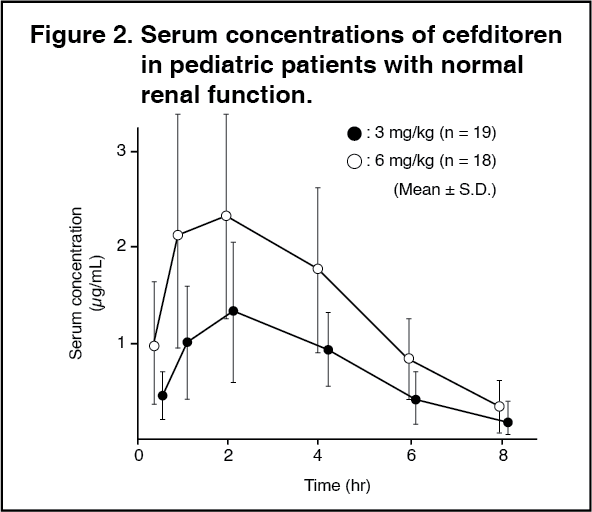 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image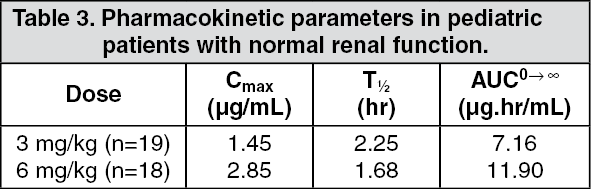 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image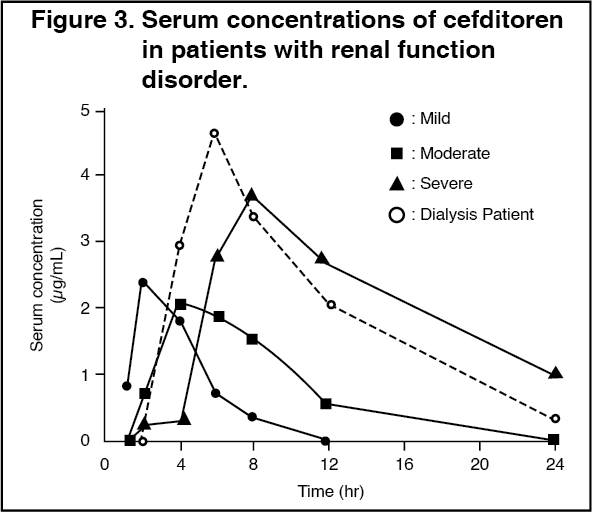 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image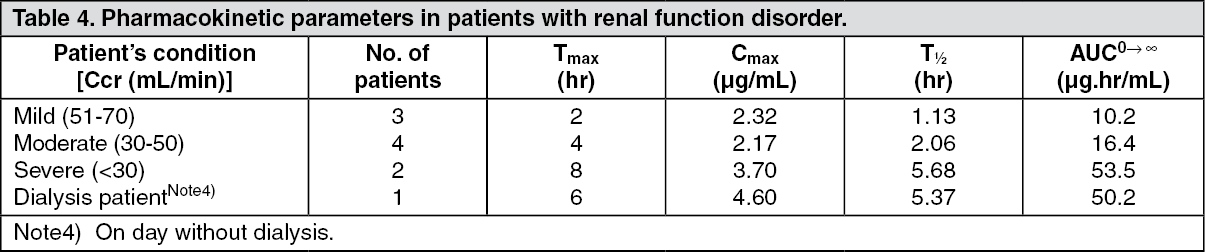 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out