All patients should be premedicated prior to PAXOLL administration in order to prevent severe hypersensitivity reactions. Such premedication may consist of dexamethasone 20 mg PO administered approximately 12 and 6 hours before PAXOLL, diphenhydramine (or its equivalent) 50 mg I.V. 30 to 60 minutes prior to PAXOLL, and cimetidine (300 mg) or ranitidine (50 mg) I.V. 30 to 60 minutes before PAXOLL. In patients previously treated with chemotherapy for ovarian cancer, the recommended regimen is PAXOLL 175 mg/m
2 administered intravenously over 3 hours every 3 weeks. For patients with carcinoma of the breast, PAXOLL at a dose of 175 mg/m
2 administered intravenously over 3 hours every 3 weeks has been shown to be effective after failure of chemotherapy for metastatic disease or relapse within 6 months of adjuvant chemotherapy. In patients previously untreated with chemotherapy for non-small cell lung carcinoma (NSCLC), the recommended regimen is 175 mg/m
2 administered intravenously over 3 hours every 3 weeks follow by a platinum compound. A more myelosuppressive regimen of PAXOLL may be 135 mg/m
2 administered intravenously over 24 hours every 3 weeks follow by a platinum compound. For patients with AIDS related Kaposi's sarcoma, PAXOLL administered at a dose of 135 mg/m
2 given intravenously over 3 hours every 3 weeks or at a dose of 100 mg/m
2 given intravenously
over 3 hours every 2 weeks is recommended (dose intensity 45-50 mg/m
2/week). Based upon the immunosuppression in patients with advanced HIV disease, the following modifications are recommended in these patients: Reduce the dose of dexamethasone as one of the three premedication drugs to 10 mg PO (instead of 20 mg PO); Initiate or repeat treatment with PAXOLL only if the neutrophil count is at least 1000 cells/mm
3; Reduce the dose of subsequent courses of PAXOLL by 20% for patients who experience severe neutropenia (neutrophil <500 cells/mm
3 for a week or longer. For the therapy of patients with solid tumors (ovary and breast), courses of PAXOLL should not be repeated until the neutrophil count is at least 1,500 cells/mm
3 and the platelet count is at least 100,000 cells/mm
3 and PAXOLL should not be given to patients with AIDS related Kaposi's sarcoma if the baseline or subsequent neutrophil count is less than 1000 cells/mm
3 patients who experience severe neutropenia (neutrophil <500 cells/mm
3 for week or longer) or severe peripheral neuropathy during PAXOLL therapy should have dosage reduced by 20% for subsequent courses of PAXOLL. The incidence of neurotoxicity and the severity of neutropenia increase with dose.
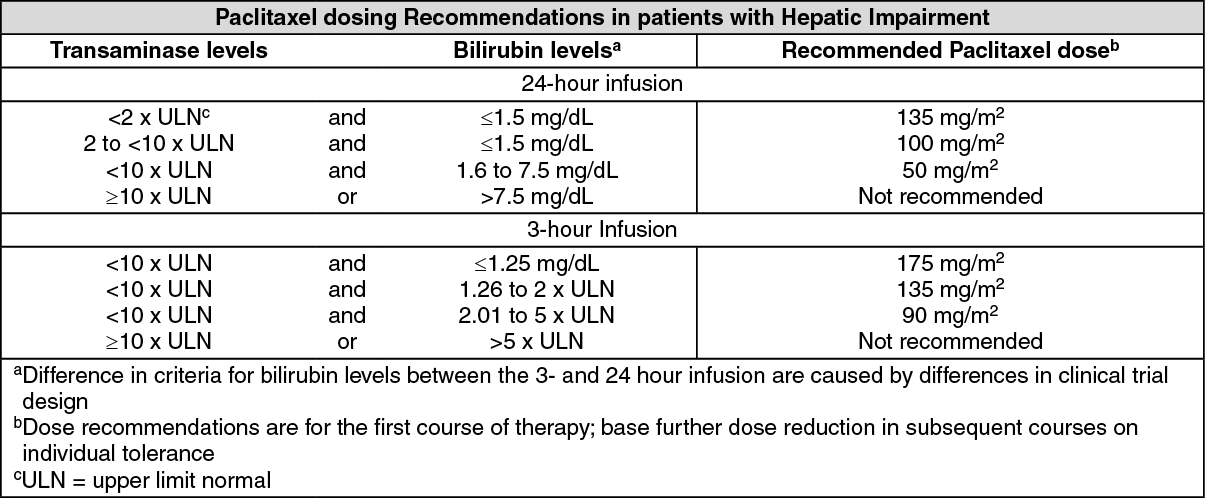
Patients with hepatic impairment may be at increased risk of toxicity particularly grade 3 to 4 myelosuppression. Recommendations for dosage adjustment for the first course of therapy are shown in the table for 3-and 24-hour infusion. Monitor patients closely for the development of profound myelosuppression.
 Click on icon to see table/diagram/image
Preparation for Intravenous Administration:
Click on icon to see table/diagram/image
Preparation for Intravenous Administration: PAXOLL must be diluted prior to infusion PAXOLL should be diluted in 0.9% Sodium Chloride Injection USP; 5% Dextrose Injection USP; 5% Dextrose and 0.9% Sodium Chloride Injection USP or 5% Dextrose in Ringer's Injection to a final concentration of 0.3 to 1.2 mg/mL. The solutions are physically and chemically stable for up to 27 hours at ambient temperature (approximately 25°C) and room lighting conditions. Upon preparation, solution may show haziness, which is attributed to the formulation vehicle.
Stability: Unopened vials of PAXOLL injection are stable until the date indicated on the package when stored between 20°C-25°C (68°-77°F), in the original package. Neither freezing nor refrigeration adversely affects the stability of the product. Upon refrigeration components in the PAXOLL vial may precipitate, but will redissolve upon reaching room
temperature with little or no agitation. There is no impact on product quality under these circumstances. If the solution remains cloudy or if an insoluble precipitate is noted, the vial should be discarded. Solutions for infusion prepared as recommended are stable at ambient temperature (approximately 25°C) and lighting conditions for up to 27 hours.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out