Malignant Pleural Mesothelioma: The table as follows provides the frequency and severity of undesirable effects that have been reported in > 5% of 168 patients with mesothelioma who were randomised to receive cisplatin and pemetrexed, and 163 patients with mesothelioma randomised to receive single-agent cisplatin. In both treatment arms, these chemonaive patients were fully supplemented with folic acid and vitamin B
12. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Frequency estimate: very common (≥1/10), common (≥1/100 and <1/10).
For the purpose of this table a cut off of 5% was used for inclusion of all events where the reporter considered a possible relationship to pemetrexed and cisplatin.
Clinically relevant CTC toxicities that were reported in ≥1% and ≤5% of the patients that were randomly assigned to receive cisplatin and pemetrexed include: renal failure, infection, pyrexia, febrile neutropenia, increased AST, ALT, and GGT, urticaria and chest pain.
Clinically relevant CTC toxicities that were reported in <1% of the patients that were randomly assigned to receive cisplatin and pemetrexed include arrhythmia and motor neuropathy.
Locally advanced or metastatic non-small cell lung cancer after prior chemotherapy: The table as follows provides the frequency and severity of undesirable effects that have been reported in > 5% of 265 patients randomly assigned to receive single-agent pemetrexed with folic acid and vitamin B
12 supplementation, and 276 patients randomly assigned to receive single-agent docetaxel. All patients were diagnosed with locally advanced or metastatic non-small cell lung cancer and received prior chemotherapy. (See Table 6.)
Click on icon to see table/diagram/image
Frequency estimate: very common (≥1/10), common (≥1/100 and <1/10).
For the purpose of this table a cut off of 5% was used for inclusion of all events where the reporter considered a possible relationship to pemetrexed.
Clinically relevant CTC toxicities that were reported in ≥1% and ≤5% of the patients that were randomly assigned to pemetrexed include: infection without neutropenia, febrile neutropenia, allergic reaction/hypersensitivity, increased creatinine, motor neuropathy, sensory neuropathy, erythema multiforme, and abdominal pain.
Clinically relevant CTC toxicities that were reported in < 1% of that patients that were randomly assigned to pemetrexed include supraventricular arrhythmias.
Clinically relevant Grade 3 and Grade 4 laboratory toxicities were similar between integrated Phase 2 results from three single-agent pemetrexed studies (N=164) and the Phase 3 single-agent pemetrexed study described previously, with the exception of neutropenia (12.8% versus 5.3%, respectively) and alanine transaminase elevation (15.2% versus 1.9%, respectively). These differences were likely due to differences in the patient population, since the Phase 2 studies included both chemonaive and heavily pre-treated breast cancer patients with pre-existing liver metastases and/or abnormal baseline liver function tests.
Locally advanced or metastatic non-small cell lung cancer: The table as follows provides the frequency and severity of undesirable effects considered possibly related to study drug that have been reported in > 5% of 839 patients with non-small cell lung cancer (NSCLC) who were randomised to receive cisplatin and pemetrexed and 830 patients with NSCLC who were randomised to receive cisplatin and gemcitabine. All patients received study therapy as initial treatment for locally advanced or metastatic NSCLC and patients in both treatment groups were fully supplemented with folic acid and vitamin B
12. (See Table 7.)
Click on icon to see table/diagram/image
Frequency estimate: very common (≥1/10), common (≥1/100 and <1/10).
For the purpose of this table, a cut off of 5% was used for inclusion of all events where the reporter considered a possible relationship to pemetrexed and cisplatin.
Clinically relevant toxicity that was reported in ≥1% and ≤ 5% of the patients that were randomly assigned to receive cisplatin and pemetrexed include: AST increase, ALT increase, infection, febrile neutropenia, renal failure, pyrexia, dehydration, conjunctivitis, and creatinine clearance decrease. Clinically relevant toxicity that was reported in < 1% of the patients that were randomly assigned to receive cisplatin and pemetrexed include: GGT increase, chest pain, arrhythmia, and motor neuropathy.
Clinically relevant toxicities with respect to gender were similar to the overall population in patients receiving pemetrexed plus cisplatin.
Locally advanced or metastatic non-small cell lung cancer after prior platinum-based chemotherapy: The table as follows provides the frequency and severity of undesirable effects considered possibly related to study drug that have been reported in > 5% of 800 patients randomly assigned to receive single-agent pemetrexed and 402 patients randomly assigned to receive placebo in the single-agent pemetrexed maintenance-(JMEN: N=663) and continuation pemetrexed maintenance (PARAMOUNT: N=539) studies.
All patients were diagnosed with Stage IIIB or IV NSCLC and had received prior platinum-based chemotherapy. Patients in both study arms were fully supplemented with folic acid and vitamin B
12. (See Table 8.)
Click on icon to see table/diagram/image
Clinically relevant CTC toxicity of any grade that was reported in ≥1 % and ≤5% of the patients that were randomly assigned to pemetrexed include: febrile neutropenia, infection, decreased platelets, decreased creatinine clearance, diarrhoea, constipation, oedema, alopecia, increased creatinine, pruritus/itching, fever (in the absence of neutropenia), ocular surface disease (including conjunctivitis), increased lacrimation, decreased glomerular filtration rate, dizziness and motor neuropathy. Clinically relevant CTC toxicity that was reported in < 1% of the patients that were randomly assigned to pemetrexed include: allergic reaction/hypersensitivity erythema multiforme, renal failure, supraventricular arrhythmia and pulmonary embolism.
Safety was assessed for patients who were randomised to receive pemetrexed (N=800). The incidence of adverse reactions was evaluated for patients who received ≤ 6 cycles of pemetrexed maintenance (N=568), and compared to patients who received > 6 cycles of pemetrexed (N=232).
Increases in adverse reactions (all grades) were observed with longer exposure; however, no statistically significant differences in any individual Grade 3/4/5 adverse reaction were seen.
Others: Serious cardiovascular and cerebrovascular events, including myocardial infarction, angina pectoris, cerebrovascular accident, and transient ischaemic attack, have been uncommonly reported during clinical studies with pemetrexed, usually when given in combination with another cytotoxic agent.
Most of the patients in whom these events have been observed had pre-existing cardiovascular risk factors.
Pancytopenia has been uncommonly reported during clinical trials with pemetrexed.
In clinical trials, cases of colitis (including intestinal and rectal bleeding, sometimes fatal, intestinal perforation, intestinal necrosis and typhlitis) have been reported uncommonly in patients treated with pemetrexed.
In clinical trials, cases of interstitial pneumonitis with respiratory insufficiency, sometimes fatal, have been reported uncommonly in patients treated with pemetrexed.
Uncommon cases of oedema have been reported in patients treated with pemetrexed.
Oesophagitis/radiation oesophagitis has been uncommonly reported during clinical trials with pemetrexed.
Sepsis, sometime fatal, has been commonly reported during clinical trials with pemetrexed.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image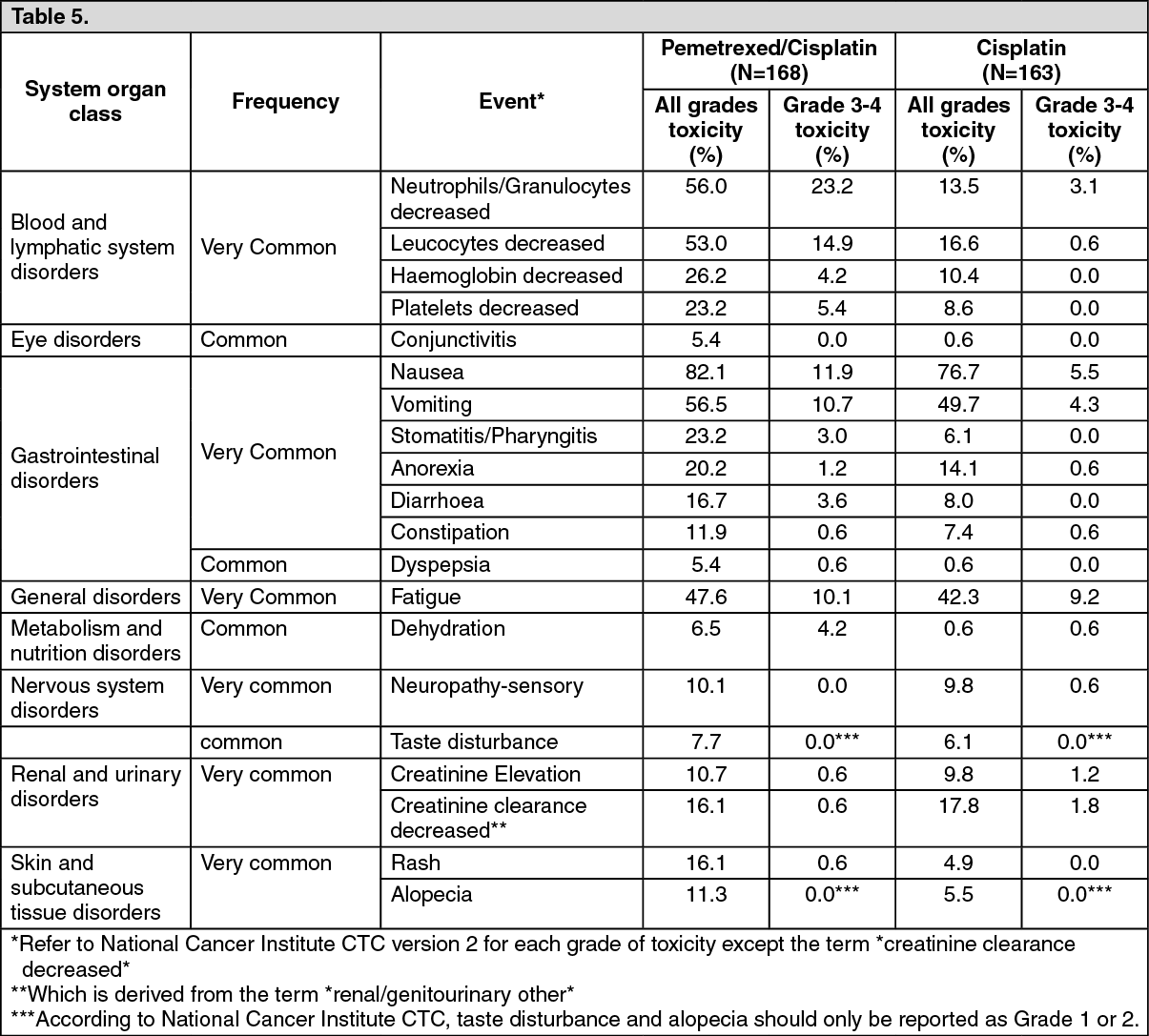 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image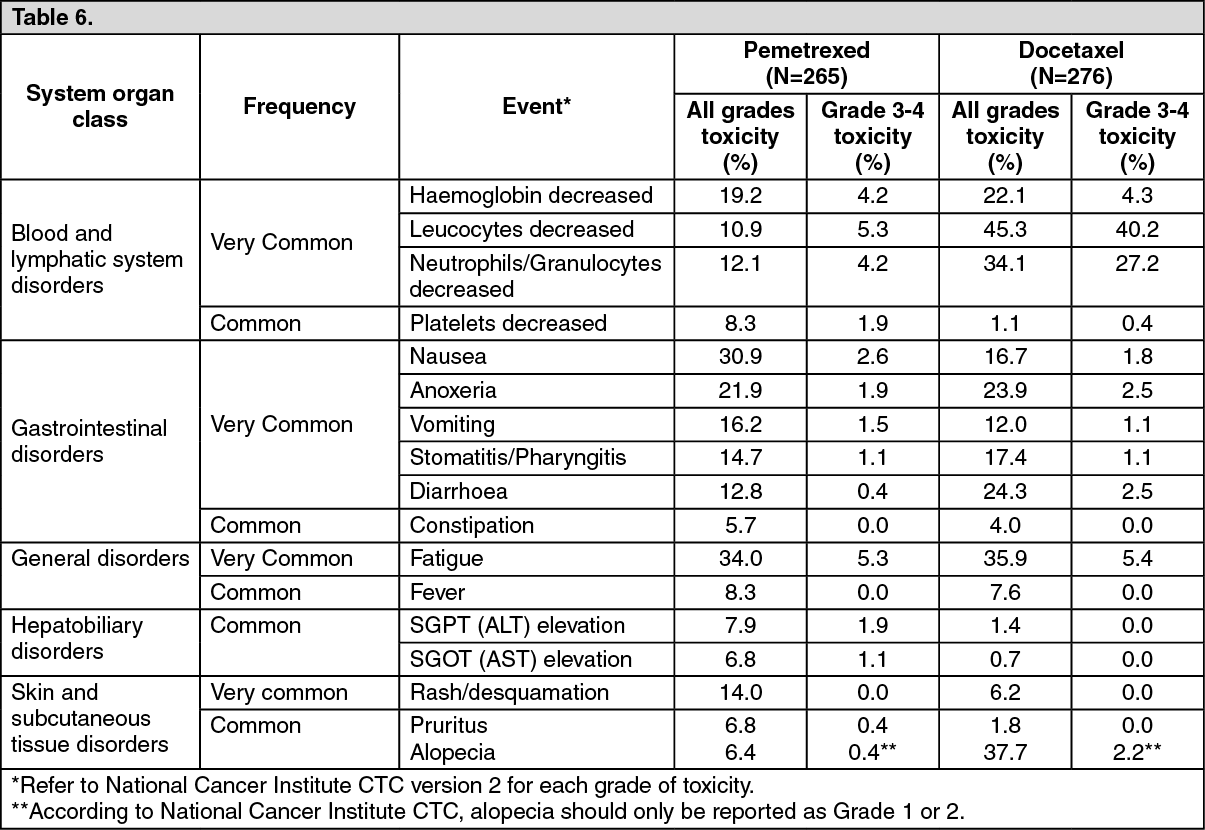 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image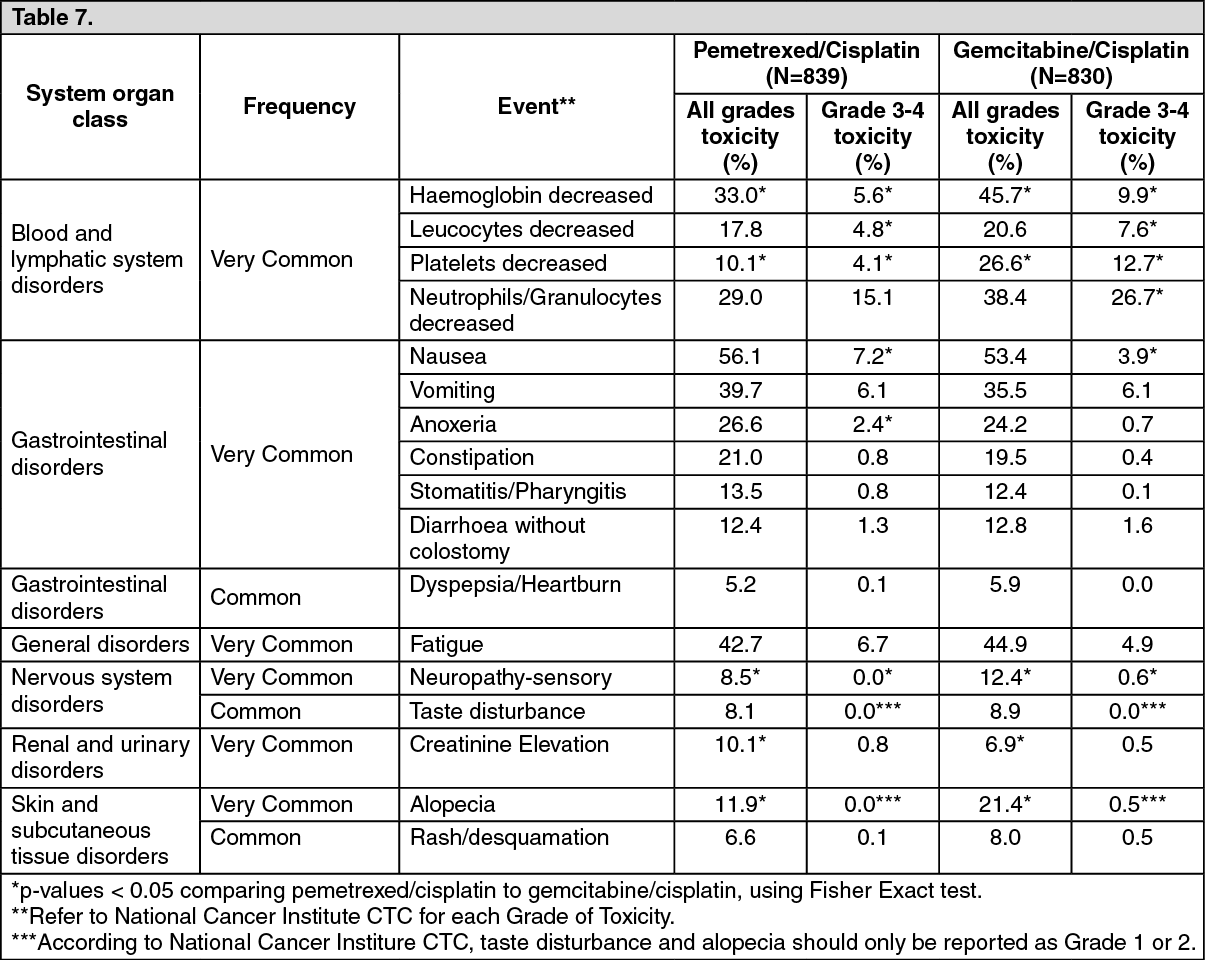 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image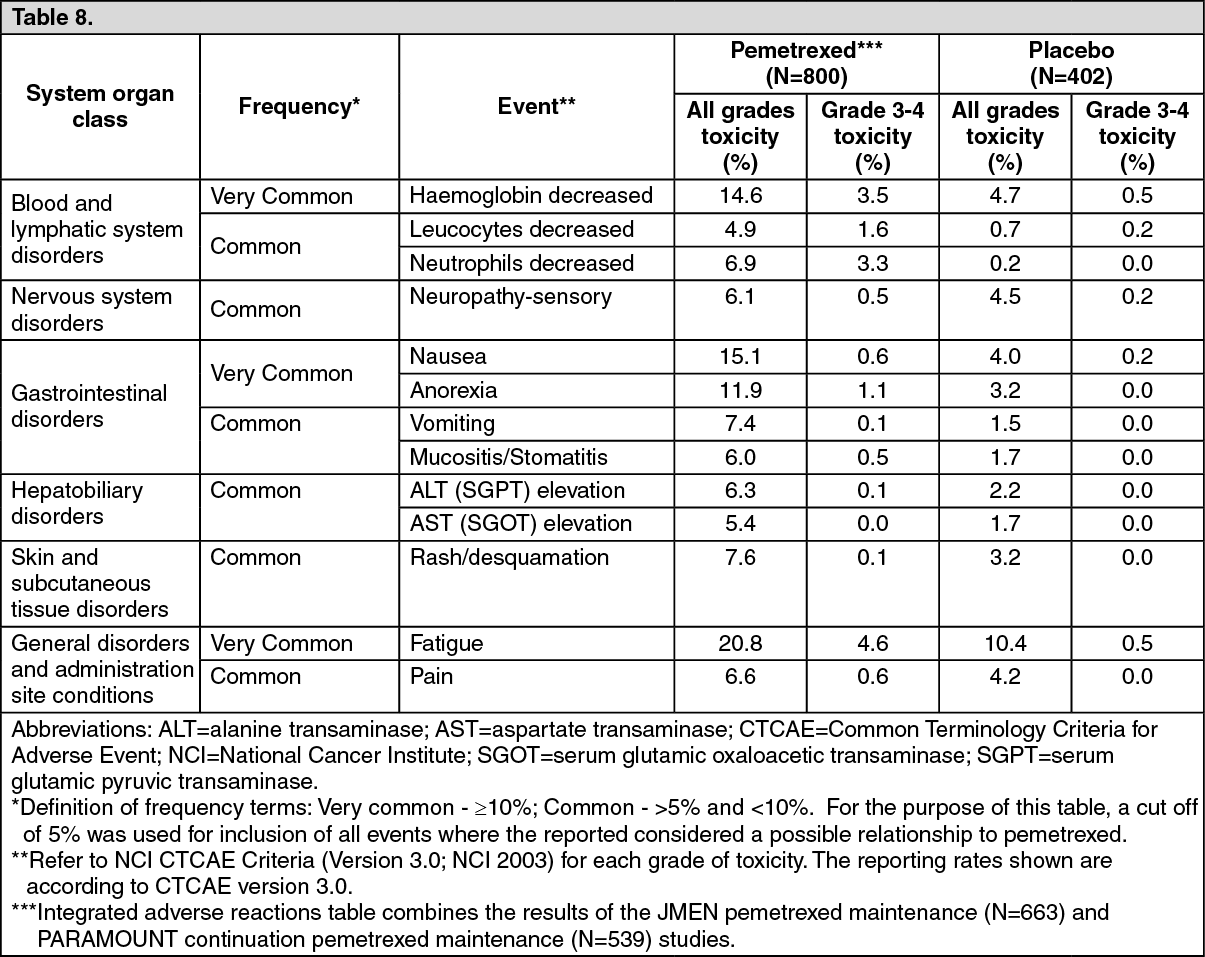 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out