


 Sign Out
Sign Out



Pharmacology: Pharmacodynamics: Clinical Studies: Mechanism of action: Qdenga contains live attenuated dengue viruses.
The primary mechanism of action of Qdenga is to replicate locally and elicit neutralizing antibodies to confer protection against dengue disease caused by any of the four dengue virus serotypes. Qdenga activates multiple arms of the immune system, including binding antibodies, complement fixing antibodies, functional antibodies to dengue nonstructural protein 1 (NS1), and cell mediated immune responses (CD4+, CD8+, and natural killer cells).
Clinical efficacy: The clinical efficacy of Qdenga was assessed in study DEN-301, a pivotal Phase 3, double-blind, randomized, placebo-controlled study conducted across 5 countries in Latin America (Brazil, Colombia, Dominican Republic, Nicaragua, Panama) and 3 countries in Asia (Sri Lanka, Thailand, the Philippines). A total of 20,099 children aged between 4 and 16 years were randomized (2:1 ratio) to receive Qdenga or placebo, regardless of previous dengue infection.
The mean age of the per protocol trial population was 9.6 years (standard deviation of 3.5 years) with 12.7% subjects in the 4-5 years, 55.2% in the 6-11 years and 32.1% in the 12-16 years age-groups. Of these, 46.5% were in Asia and 53.5% were in Latin America, 49.5% were females and 50.5% were males.
The dengue serostatus at baseline (before the first injection) was assessed in all subjects by Micro Neutralization Test (MNT50) to allow Vaccine Efficacy (VE) assessment by baseline serostatus. The baseline dengue seronegativity rate for the overall per protocol population was 27.7%.
Efficacy was assessed using active surveillance across the entire study duration. Any subject with febrile illness (defined as fever ≥38°C on any 2 of 3 consecutive days) was required to visit the study site for dengue fever evaluation by the investigator. Subjects/guardians were reminded of this requirement at least weekly to maximize the detection of all symptomatic virologically-confirmed dengue (VCD) cases. Febrile episodes were confirmed by a validated, quantitative dengue RT-PCR to detect specific dengue serotypes.
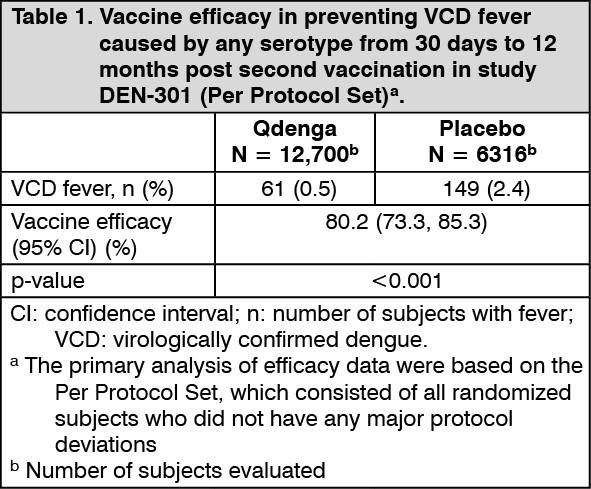
Clinical efficacy data for subjects 4 to 16 years of age: The Vaccine Efficacy (VE) results, according to the primary endpoint (VCD fever occurring from 30 days to 12 months after the second vaccination) are shown in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
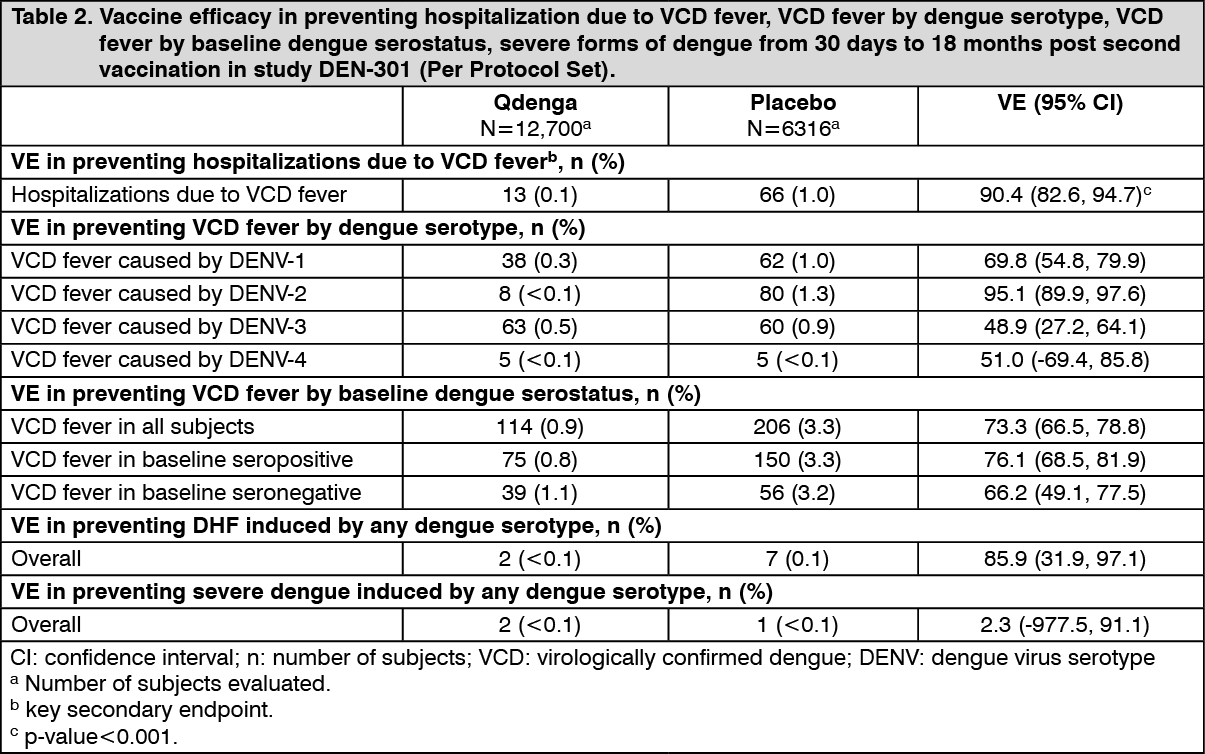
Click on icon to see table/diagram/imageVE results according to the secondary endpoints, preventing hospitalization due to VCD fever, preventing VCD fever by serostatus, by serotype and preventing severe VCD fever are shown in Table 2. For severe VCD fever, two types of endpoints were considered: clinically severe VCD cases and VCD cases that met the 1997 WHO criteria for Dengue Haemorrhagic Fever (DHF). The criteria used in Trial DEN-301 for the assessment of VCD severity by an independent "Dengue Case severity Adjudication Committee" (DCAC) were based on the WHO 2009 guidelines. The DCAC assessed all cases of hospitalisation due to VCD utilizing predefined criteria which included an assessment of bleeding abnormality, plasma leakage, liver function, renal function, cardiac function, the central nervous system, and shock. In Trial DEN-301 VCD cases meeting the WHO 1997 criteria for DHF were identified using a programmed algorithm, i.e., without applying medical judgment. Broadly, the criteria included presence of fever lasting 2 to 7 days, haemorrhagic tendencies, thrombocytopenia, and evidence of plasma leakage. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRapid onset of protection was seen with an exploratory VE of 81.1% (95% CI: 64.1%, 90.0%) against VCD fever caused by all serotypes combined from first vaccination until second vaccination.
Clinical efficacy for subjects 17 to 60 years of age: No clinical efficacy study has been conducted in subjects from 17 years of age. The clinical efficacy of Qdenga in subjects from 17 years of age is based on bridging of immunogenicity data from clinical efficacy in subjects from 4-16 years of age (see Immunogenicity data for subjects 18 to 60 years of age in non-endemic areas as follows).
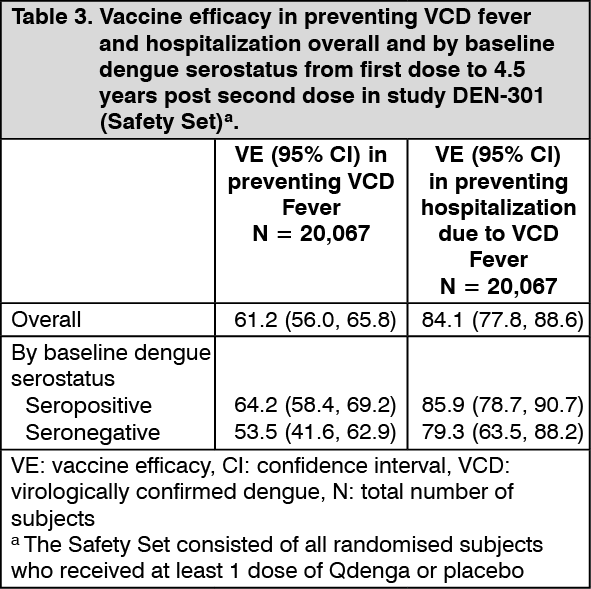
Long term protection: In study DEN-301, a number of exploratory analyses were conducted to estimate long term protection from first dose up to 4.5 years after the second dose (Table 3). (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditionally, VE in preventing DHF caused by any serotype was 70.0% (95% CI: 31.5%, 86.9%) and in preventing clinically severe VCD cases caused by any serotype was 70.2% (95% CI: -24.7%, 92.9%).
Up to four and a half years after the second dose, VE in preventing VCD was shown for all four serotypes in baseline dengue seropositive subjects. In baseline seronegative subjects, VE was shown for DENV-1 and DENV-2, but not suggested for DENV-3 and could not be shown for DENV-4 due to lower incidence of cases.
Immunogenicity: During clinical development, immunogenicity data were collected in 9 studies with 3877 subjects who received 2 doses of Qdenga 3 months apart; 2796 of these subjects lived in dengue endemic areas and 1081 subjects lived in non-endemic areas.
Neutralizing antibody titers for each serotype were measured with the microneutralization test (MNT50) and presented as Geometric Mean Titers (GMTs).
In the tables as follows, the dengue serostatus at baseline (before the first injection) was identified as: Dengue seropositive if the MNT50 titer was ≥10 (the lower limit of detection, LLOD), against at least one serotype; Dengue seronegative if the MNT50 titer was < the LLOD against all 4 serotypes.
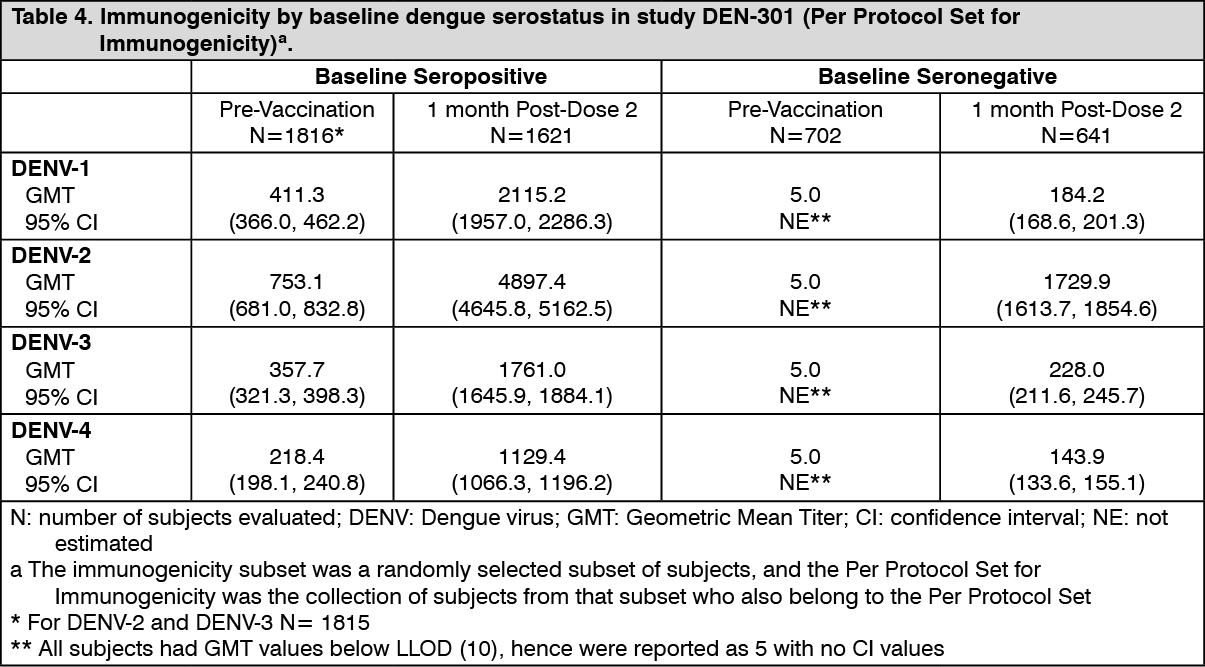
Immunogenicity data for subjects 4 to 16 years of age in endemic areas: The GMTs by baseline dengue serostatus in subjects 4 to 16 years of age in study DEN-301 are shown in Table 4. (See Table 4.)
 Click on icon to see table/diagram/image
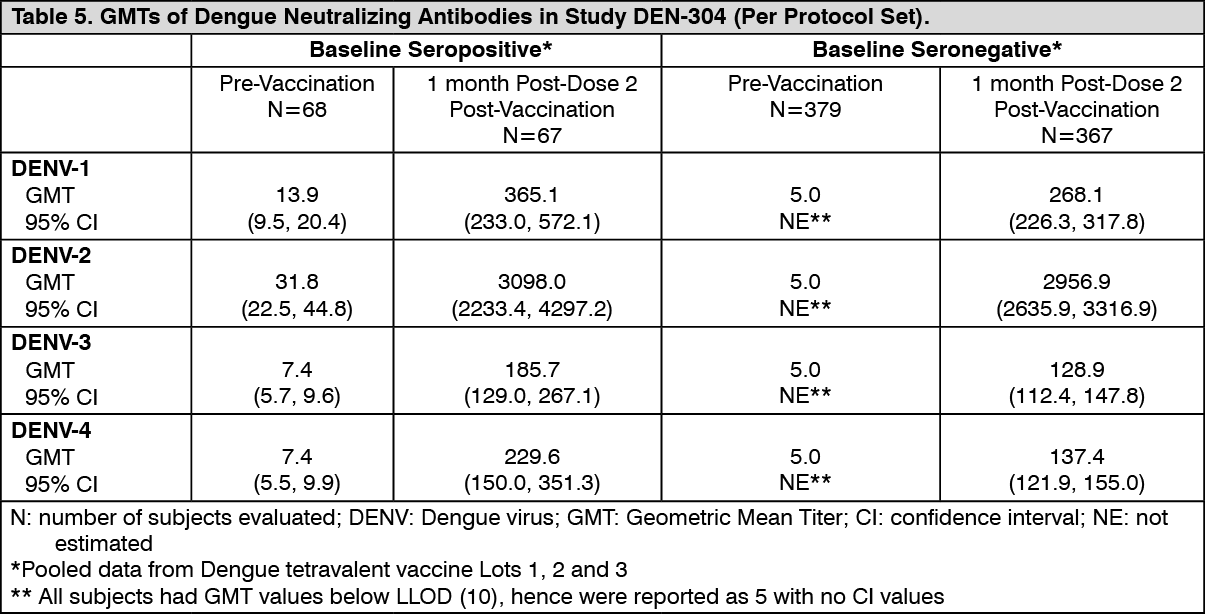
Click on icon to see table/diagram/imageImmunogenicity data for subjects 18 to 60 years of age in non-endemic areas: The immunogenicity of Qdenga in adults 18 to 60 years of age was assessed in DEN-304, a Phase 3 double-blind, randomized, placebo-controlled study in a non-endemic country (US). The post-dose 2 GMTs are shown in Table 5. (See Table 5.)
 Click on icon to see table/diagram/image
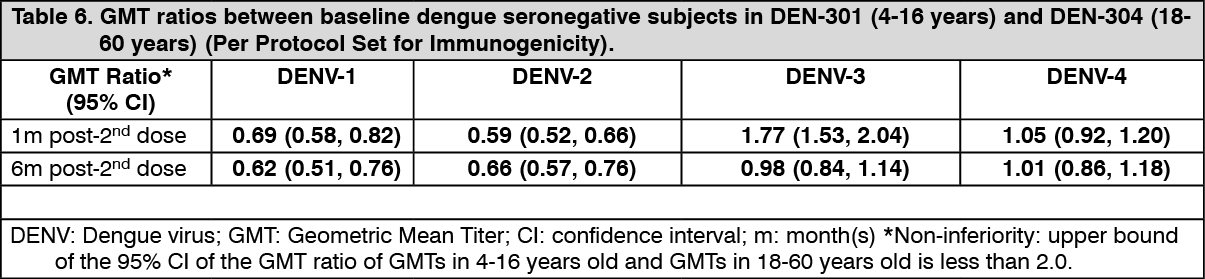
Click on icon to see table/diagram/imageThe bridging of efficacy is based on immunogenicity data and results from a non-inferiority analysis, comparing post-vaccination GMTs in the baseline dengue seronegative populations of DEN-301 and DEN-304 (Table 6). Protection against dengue disease is expected in adults although the actual magnitude of efficacy relative to that observed in children and adolescents is unknown. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLong-term persistence of antibodies: The long-term persistence of neutralizing antibodies was shown in study DEN-301, with titers remaining well above the pre-vaccination levels for all four serotypes, up to 51 months after the first dose.
Pharmacokinetics: No pharmacokinetic studies have been performed with Qdenga.
Toxicology: Nonclinical Safety Data: Carcinogenesis, Mutagenesis, Impairment of Fertility: Animal Toxicology and/or Pharmacology: Non-clinical safety data revealed no special hazard for humans based on conventional studies of single dose, local tolerance, repeated dose toxicity, and toxicity to reproduction and development.
In a distribution and shedding study, there was no shedding of Qdenga RNA in feces and urine, confirming a low risk for vaccine shedding to the environment or transmission from vaccinees. A neurovirulence study shows that Qdenga is not neurotoxic.