


 Sign Out
Sign Out

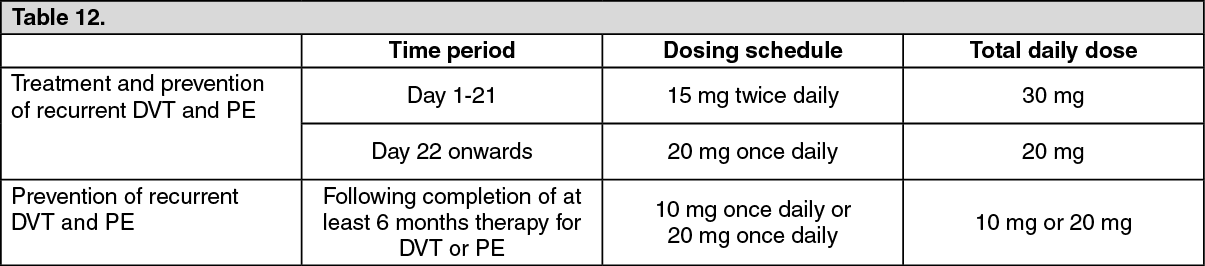
Short duration of therapy (at least 3 months) should be considered in patients with DVT or PE provoked by major transient risk factors (i.e. recent major surgery or trauma). Longer duration of therapy should be considered in patients with provoked DVT or PE not related to major transient risk factors, unprovoked DVT or PE, or a history of recurrent DVT or PE.
When extended prevention of recurrent DVT and PE is indicated (following completion of at least 6 months therapy for DVT or PE), the recommended dose is 10 mg once daily. In patients in whom the risk of recurrent DVT or PE is considered high, such as those with complicated comorbidities, or who have developed recurrent DVT or PE on extended prevention with Rivaxored 10 mg once daily, a dose of Rivaxored 20 mg once daily should be considered.
The duration of therapy and dose selection should be individualised after careful assessment of the treatment benefit against the risk for bleeding (see Precautions). (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTo support the dose switch from 15 mg to 20 mg after Day 21 a first 4 weeks treatment initiation pack of Rivaxored for treatment of DVT/PE is available.
If a dose is missed during the 15 mg twice daily treatment phase (day 1 - 21), the patient should take Rivaxored immediately to ensure intake of 30 mg Rivaxored per day. In this case two 15 mg tablets may be taken at once. The patient should continue with the regular 15 mg twice daily intake as recommended on the following day.
If a dose is missed during the once daily treatment phase, the patient should take Rivaxored immediately, and continue on the following day with the once daily intake as recommended. The dose should not be doubled within the same day to make up for a missed dose.
Prevention of VTE in adult patients undergoing elective hip or knee replacement surgery: 10 mg: The recommended dose is 10 mg rivaroxaban taken orally once daily. The initial dose should be taken 6 to 10 hours after surgery, provided that haemostasis has been established.
The duration of treatment depends on the individual risk of the patient for venous thromboembolism which is determined by the type of orthopaedic surgery.
For patients undergoing major hip surgery, a treatment duration of 5 weeks is recommended.
For patients undergoing major knee surgery, a treatment duration of 2 weeks is recommended.
If a dose is missed the patient should take Rivaxored immediately and then continue the following day with once daily intake as before.
Prevention of stroke and systemic embolism: 15 mg and 20 mg: The recommended dose is 20 mg once daily, which is also the recommended maximum dose.
Therapy with rivaroxaban should be continued long term provided the benefit of prevention of stroke and systemic embolism outweighs the risk of bleeding (see Precautions).
If a dose is missed the patient should take Rivaxored immediately and continue on the following day with the once daily intake as recommended. The dose should not be doubled within the same day to make up for a missed dose.
Treatment of VTE and prevention of VTE recurrence in children and adolescents: 15 mg and 20 mg: Rivaxored treatment in children and adolescents aged less than 18 years should be initiated following at least 5 days of initial parenteral anticoagulation treatment (see Pharmacology: Pharmacodynamics under Actions).
The dose for children and adolescent is calculated based on body weight.
Body weight from 30 to 50 kg: a once daily dose of 15 mg rivaroxaban is recommended. This is the maximum daily dose.
Body weight of 50 kg or more: a once daily dose of 20 mg rivaroxaban is recommended. This is the maximum daily dose.
For patients with body weight less 30 kg refer to the Summary of Product Characteristics of rivaroxaban granules for oral suspension.
The weight of a child should be monitored and the dose reviewed regularly.
This is to ensure a therapeutic dose is maintained. Dose adjustments should be made based on changes in body weight only.
Treatment should be continued for at least 3 months in children and adolescents. Treatment can be extended up to 12 months when clinically necessary. There is no data available in children to support a dose reduction after 6 months treatment. The benefit-risk of continued therapy after 3 months should be assessed on an individual basis taking into account the risk for recurrent thrombosis versus the potential bleeding risk.
If a dose is missed, the missed dose should be taken as soon as possible after it is noticed, but only on the same day. If this is not possible, the patient should skip the dose and continue with the next dose as prescribed. The patient should not take two doses to make up for a missed dose.
Converting from Vitamin K Antagonists (VKA) to Rivaxored: Prevention of stroke and systemic embolism: VKA treatment should be stopped and rivaroxaban therapy should be initiated when the International Normalised Ratio (INR) is ≤ 3.0. (For 15 mg and 20 mg only.)
Treatment of DVT, PE and prevention of recurrence in adults and treatment of VTE and prevention of recurrence in paediatric patients: VKA treatment should be stopped and Rivaxored therapy should be initiated once the INR is ≤ 2.5.
When converting patients from VKAs to Rivaxored, International Normalised Ratio (INR) values will be falsely elevated after the intake of Rivaxored. The INR is not valid to measure the anticoagulant activity of rivaroxaban, and therefore should not be used (see Interactions).
Converting from Rivaxored to Vitamin K antagonists (VKA): There is a potential for inadequate anticoagulation during the transition from Rivaxored to VKA. Continuous adequate anticoagulation should be ensured during any transition to an alternate anticoagulant. It should be noted that Rivaxored can contribute to an elevated INR.
In patients converting from Rivaxored to VKA, VKA should be given concurrently until the INR is ≥ 2.0. For the first two days of the conversion period, standard initial dosing of VKA should be used followed by VKA dosing, as guided by INR testing. While patients are on both Rivaxored and VKA the INR should not be tested earlier than 24 hours after the previous dose but prior to the next dose of Rivaxored. Once Rivaxored is discontinued INR testing may be done reliably at least 24 hours after the last dose (see Interactions and Pharmacology: Pharmacokinetics under Actions).
Paediatric patients: 15 mg and 20 mg: Children who convert from Rivaxored to VKA need to continue Rivaxored for 48 hours after the first dose of VKA. After 2 days of co-administration an INR should be obtained prior to the next scheduled dose of Rivaxored. Co-administration of Rivaxored and VKA is advised to continue until the INR is ≥ 2.0. Once Rivaxored is discontinued INR testing maybe done reliably 24 hours after the last dose (see previous text and Interactions).
Converting from parenteral anticoagulants to Rivaxored: For adult and paediatric patients currently receiving a parenteral anticoagulant, discontinue the parenteral anticoagulant and start Rivaxored 0 to 2 hours before the time that the next scheduled administration of the parenteral medicinal product (e.g. low molecular weight heparins) would be due or at the time of discontinuation of a continuously administered parenteral medicinal product (e.g. intravenous unfractionated heparin).
Converting from rivaroxaban to parenteral anticoagulants: Discontinue Rivaxored (for 15 mg and 20 mg only) and give the first dose of parenteral anticoagulant at the time the next rivaroxaban dose would be taken.
Special populations: Renal impairment: Adults: Limited clinical data for patients with severe renal impairment (creatinine clearance 15 - 29 ml/min) indicate that rivaroxaban plasma concentrations are significantly increased. Therefore, Rivaxored is to be used with caution in these patients. Use is not recommended in patients with creatinine clearance < 15 ml/min (see Precautions and Pharmacology: Pharmacokinetics under Actions).
For the prevention of VTE in adult patients undergoing elective hip or knee replacement surgery, no dose adjustment is necessary in patients with mild renal impairment (creatinine clearance 50 - 80 ml/min) or moderate renal impairment (creatinine clearance 30 - 49 ml/min) (see Pharmacology: Pharmacokinetics under Actions) (for 10 mg only).
For the treatment of DVT, treatment of PE and prevention of recurrent DVT and PE, no dose adjustment from the recommended dose is necessary in patients with mild renal impairment (creatinine clearance 50 - 80 ml/min) (see Pharmacology: Pharmacokinetics under Actions) (for 10 mg only).
In patients with moderate (creatinine clearance 30 - 49 ml/min) or severe (creatinine clearance 15 - 29 ml/min) renal impairment the following dose recommendations apply: For the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation, the recommended dose is 15 mg once daily (see Pharmacology: Pharmacokinetics under Actions) (for 15 mg and 20 mg only).
For the treatment of DVT, treatment of PE and prevention of recurrent DVT and PE: Patients should be treated with 15 mg twice daily for the first 3 weeks. Thereafter, when the recommended dose is 20 mg once daily, a reduction of the dose from 20 mg once daily to 15 mg once daily should be considered if the patient's assessed risk for bleeding outweighs the risk for recurrent DVT and PE. The recommendation for the use of 15 mg is based on PK modelling and has not been studied in this clinical setting (see Precautions, Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions).
When the recommended dose is 10 mg once daily, no dose adjustment from the recommended dose is necessary.
No dose adjustment is necessary in patients with mild renal impairment (creatinine clearance 50 - 80 ml/min) (see Pharmacology: Pharmacokinetics under Actions). (For 15 mg and 20 mg only.)
Hepatic impairment: Rivaroxaban is contraindicated in patients with hepatic disease associated with coagulopathy and clinically relevant bleeding risk including cirrhotic patients with Child Pugh B and C (see Contraindications and Pharmacology: Pharmacokinetics under Actions).
No clinical data is available in children with hepatic impairment (for 15 mg and 20 mg only).
Elderly population: No dose adjustment (see Pharmacology: Pharmacokinetics under Actions).
Body weight: No dose adjustment (see Pharmacology: Pharmacokinetics under Actions).
For paediatric patients the dose is determined based on body weight (for 15 mg and 20 mg only).
Gender: No dose adjustment (see Pharmacology: Pharmacokinetics under Actions).
Patients undergoing cardioversion: 15 mg and 20 mg: Rivaroxaban can be initiated or continued in patients who may require cardioversion.
For transesophageal echocardiogram (TEE) guided cardioversion in patients not previously treated with anticoagulants, Rivaxored treatment should be started at least 4 hours before cardioversion to ensure adequate anticoagulation (see Pharmacology: Pharmacodynamics and Pharmacokinetics under Actions). For all patients, confirmation should be sought prior to cardioversion that the patient has taken Rivaxored as prescribed. Decisions on initiation and duration of treatment should take established guideline recommendations for anticoagulant treatment in patients undergoing cardioversion into account.
Patients with non-valvular atrial fibrillation who undergo PCI (percutaneous coronary intervention) with stent placement: 15 mg and 20 mg: There is limited experience of a reduced dose of 15 mg Rivaxored once daily (or 10 mg Rivaxored once daily for patients with moderate renal impairment [creatinine clearance 30-49 ml/min]) in addition to a P2Y12 inhibitor for a maximum of 12 months in patients with non-valvular atrial fibrillation who require oral anticoagulation and undergo PCI with stent placement (see Precautions and Pharmacology: Pharmacodynamics under Actions).
Paediatric population: 10 mg: The safety and efficacy of Rivaxored 10 mg tablets in children aged 0 to 18 years have not been established. No data are available. Therefore, Rivaxored 10 mg tablets are not recommended for use in children below 18 years of age.
15 mg and 20 mg: The safety and efficacy of Rivaxored in children aged 0 to < 18 years have not been established in the indication prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation. No data are available. Therefore, it is not recommended for use in children below 18 years of age in indications other than the treatment of VTE and prevention of VTE recurrence.
Children and adolescents with mild renal impairment (glomerular filtration rate 50 - 80 mL/min/1.73 m2): no dose adjustment is required, based on data in adults and limited data in paediatric patients (see Pharmacology: Pharmacokinetics under Actions).
Children and adolescents with moderate or severe renal impairment (glomerular filtration rate < 50 mL/min/1.73 m2): Rivaroxaban is not recommended as no clinical data is available (see Precautions).
Method of administration: Adults: Rivaxored is for oral use.
10 mg: The tablets can be taken with or without food (see Interactions and Pharmacology: Pharmacokinetics under Actions).
15 mg and 20 mg: The tablets can be taken with food (see Pharmacology: Pharmacokinetics under Actions).
Crushing of tablets: For patients who are unable to swallow whole tablets, Rivaxored tablet may be crushed and mixed with water or apple puree immediately prior to use and administered orally. After the administration of crushed Rivaxored 15 mg or 20 mg film-coated tablets, the dose should be immediately followed by food.
The crushed tablet may also be given through gastric tubes (see Pharmacology: Pharmacokinetics under Actions and Special precautions for disposal and other handling under Cautions for Usage).
Children and adolescents weighing 30 kg to 50 kg: 15 mg and 20 mg: Rivaxored is for oral use.
The patient should be advised to swallow the tablet with liquid. It should also be taken with food (see Pharmacology: Pharmacokinetics under Actions). The tablets should be taken approximately 24 hours apart.
In case the patient immediately spits up the dose or vomits within 30 minutes after receiving the dose, a new dose should be given. However, if the patient vomits more than 30 minutes after the dose, the dose should not be re-administered and the next dose should be taken as scheduled.
The tablet must not be split in an attempt to provide a fraction of a tablet dose.