The following adverse reactions are discussed elsewhere in the monograph: Infusion-Related Reactions [see Infusion-Related Reactions under Precautions]; Interstitial Lung Disease/Pneumonitis [see Interstitial Lung Disease/Pneumonitis under Precautions]; Dermatologic Adverse Reactions [see Dermatologic Adverse Reactions under Precautions]; Ocular Toxicity [see Ocular Toxicity under Precautions].
Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
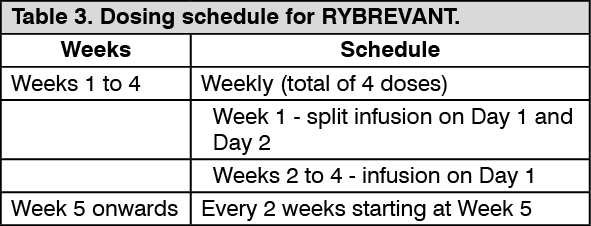
The safety population described in Precautions reflect exposure to RYBREVANT as a single agent in the CHRYSALIS study in 302 patients with locally advanced or metastatic NSCLC who received a dose of 1050 mg (for patients <80 kg) or 1400 mg (for patients ≥80 kg) once weekly for 4 weeks, then every 2 weeks thereafter. Among 302 patients who received RYBREVANT, 36% were exposed for 6 months or longer and 12% were exposed for greater than one year. In the safety population, the most common (≥20%) adverse reactions were rash, infusion-related reaction, paronychia, musculoskeletal pain, dyspnea, nausea, edema, cough, fatigue, stomatitis, constipation, vomiting and pruritus. The most common Grade 3 to 4 laboratory abnormalities (≥2%) were decreased lymphocytes, decreased phosphate, decreased albumin, increased glucose, increased gamma glutamyl transferase, decreased sodium, decreased potassium, and increased alkaline phosphatase.
The data described as follows reflect exposure to RYBREVANT at the recommended dosage in 129 patients with locally advanced or metastatic NSCLC with EGFR exon 20 insertion mutations whose disease had progressed on or after platinum-based chemotherapy. Among patients who received RYBREVANT, 44% were exposed for 6 months or longer and 12% were exposed for greater than one year.
The median age was 62 years (range: 36 to 84 years); 61% were female; 55% were Asian, 35% were White, and 2.3% were Black; and 82% had baseline body weight <80 kg.
Serious adverse reactions occurred in 30% of patients who received RYBREVANT. Serious adverse reactions in ≥2% of patients included pulmonary embolism, pneumonitis/ILD, dyspnea, musculoskeletal pain, pneumonia, and muscular weakness. Fatal adverse reactions occurred in 2 patients (1.5%) due to pneumonia and 1 patient (0.8%) due to sudden death.
Permanent discontinuation of RYBREVANT due to an adverse reaction occurred in 11% of patients. Adverse reactions resulting in permanent discontinuation of RYBREVANT in ≥1% of patients were pneumonia, IRR, pneumonitis/ILD, dyspnea, pleural effusion, and rash.
Dose interruptions of RYBREVANT due to an adverse reaction occurred in 78% of patients. Infusion-related reactions (IRR) requiring infusion interruptions occurred in 59% of patients. Adverse reactions requiring dose interruption in ≥5% of patients included dyspnea, nausea, rash, vomiting, fatigue, and diarrhea.
Dose reductions of RYBREVANT due to an adverse reaction occurred in 15% of patients. Adverse reactions requiring dose reductions in ≥2% of patients included rash and paronychia.
The most common adverse reactions (≥20%) were rash, IRR, paronychia, musculoskeletal pain, dyspnea, nausea, fatigue, edema, stomatitis, cough, constipation, and vomiting. The most common Grade 3 to 4 laboratory abnormalities (≥2%) were decreased lymphocytes, decreased albumin, decreased phosphate, decreased potassium, increased glucose, increased alkaline phosphatase, increased gamma-glutamyl transferase, and decreased sodium.
Table 8 summarizes the adverse reactions in CHRYSALIS. (See Table 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Clinically relevant adverse reactions in <10% of patients who received RYBREVANT included ocular toxicity, ILD/pneumonitis, and toxic epidermal necrolysis (TEN).
Table 9 summarizes the laboratory abnormalities in CHRYSALIS. (See Table 9.)
Click on icon to see table/diagram/image
Immunogenicity: As with all therapeutic proteins, there is the potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies in the studies described as follows with the incidence of antibodies in other studies or to other amivantamab products may be misleading.
In CHRYSALIS, 3 of the 286 (1%) patients who were treated with RYBREVANT and evaluable for the presence of anti-drug antibodies (ADA), tested positive for treatment-emergent anti-amivantamab-vmjw antibodies (one at 27 days, one at 59 days and one at 168 days after the first dose) with titers of 1:40 or less. There are insufficient data to evaluate the effect of ADA on the pharmacokinetics, safety, or efficacy of RYBREVANT.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out