The following section describes the undesirable effects reported for levodopa/carbidopa and for entacapone used in combination with levodopa/DDC inhibitor.
Levodopa/Carbidopa: Undesirable effects that occur frequently with levodopa/carbidopa are those due to the central neuropharmacological activity of dopamine. These reactions can usually be diminished by levodopa dosage reduction. The most common undesirable effects are dyskinesias including choreiform, dystonic and other involuntary movements. Muscle twitching and blepharospasm may be taken as early signs to consider levodopa dosage reduction. Nausea, also related to enhanced central dopaminergic activity, is a common adverse effect of levodopa/carbidopa.
Other undesirable effects associated with levodopa/carbidopa therapy are mental changes, including paranoid ideation and psychotic episodes; depression, with or without development of suicidal tendencies; and cognitive dysfunction. Adding of entacapone to levodopa/DDC inhibitor therapy (carbidopa or benserazide) ie, initiation of Stalevo treatment in an entacapone-naive patient, may aggravate some of these mental changes (see table, Psychiatric Disorders).
Less frequent undesirable effects of levodopa/carbidopa therapy are irregular heart rhythm and/or palpitations, orthostatic hypotensive episodes, bradykinetic episodes (the 'on-off' phenomenon), anorexia, vomiting, dizziness and somnolence.
Gastrointestinal bleeding, development of duodenal ulcer, hypertension, phlebitis, leucopenia, haemolytic and nonhaemolytic anaemia, thrombocytopenia, agranulocytosis, chest pain, dyspnoea and paraesthesia have occurred rarely with levodopa/carbidopa.
Convulsions have occurred rarely with levodopa/carbidopa; however a causal relationship to levodopa/carbidopa therapy has not been established.
Other undesirable effects that have been reported with levodopa and may, therefore, also be potential undesirable effects of Stalevo, include:
Metabolism and Nutrition Disorders: Weight gain or loss, oedema.
Psychiatric Disorders: Confusion, insomnia, nightmares, hallucinations, delusions, agitation, anxiety, euphoria.
Nervous System Disorders: Ataxia, numbness, increased hand tremor, muscle twitching, muscle cramp, trismus, activation of latent Horner's syndrome. Falling and gait abnormalities are also potential undesirable effects.
Eye Disorders: Diplopia, blurred vision, dilated pupils, oculogyric crises.
Gastrointestinal Disorders: Dry mouth, bitter taste, sialorrhoea, dysphagia, bruxism, hiccups, abdominal pain and distress, constipation, diarrhoea, flatulence, burning sensation of the tongue.
Skin and Subcutaneous Tissue Disorders: Flushing, increased sweating, dark sweat, rash, hair loss.
Renal and Urinary Disorders: Urinary retention, urinary incontinence, dark urine, priapism.
Miscellaneous: Weakness, faintness, fatigue, headache, hoarseness, malaise, hot flushes, sense of stimulation, bizarre breathing patterns, NMS, malignant melanoma.
Entacapone: The most frequent adverse reactions caused by entacapone relate to the increased dopaminergic activity and occur most commonly at the beginning of the treatment. Reduction of levodopa dosage decreases the severity and frequency of the reactions. The other major class of adverse reactions are gastrointestinal symptoms eg, nausea, vomiting, abdominal pain, constipations and diarrhoea. Urine may be discoloured reddish-brown by entacapone, but this is a harmless phenomenon.
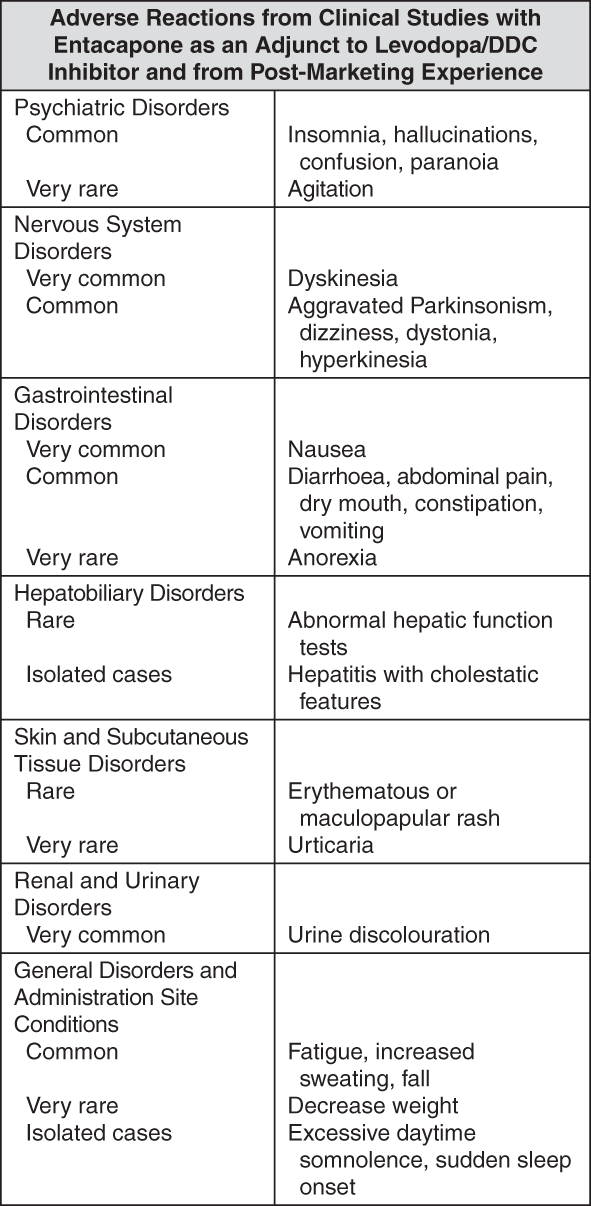
The following adverse reactions, listed in the following table, have been accumulated both from clinical studies with entacapone as an adjunct to levodopa/DDC inhibitor and since the introduction of entacapone into the market for the combination use of entacapone with levodopa/DDC inhibitor.
Adverse reactions are ranked under headings of frequency, the most frequent first, using the following convention: Very common (≥1/10); common (≥1/100, <1/10); uncommon (≥1/1000, <1/100); rare (≥1/10,000, <1/1000); very rare (<1/10,000), including isolated reports. Within each frequency grouping, adverse reactions are ranked in order of decreasing seriousness. (See table.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Entacapone used in combination with levodopa has been associated with isolated cases of excessive daytime somnolence and sudden sleep onset episodes (see Effects on the Ability to Drive or Operate Machinery under Precautions).
Laboratory Tests: The following laboratory abnormalities have been reported with levodopa/carbidopa treatment and should, therefore, be borne in mind when treating patients with Stalevo:
Commonly, levels of BUN, creatinine and uric acid are lower during administration of levodopa/carbidopa than with levodopa alone. Transient abnormalities include elevated values of blood urea, AST (SGOT), ALT (SGPT), LDH, bilirubin and alkaline phosphatase.
Decreased haemoglobin, haematocrit, elevated serum glucose and white blood cells, bacteria and blood in the urine have been reported.
Positive Coombs' tests have been reported, both for levodopa/carbidopa and for levodopa alone, but haemolytic anaemia is extremely rare.
Levodopa/carbidopa may cause false-positive result when a dipstick is used to test for urinary ketone; this reaction is not altered by boiling the urine sample. The use of glucose oxidase methods may give false-negative results for glycosuria.




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image




 Sign Out
Sign Out
