Pharmacotherapeutic group: Drugs used in type 2 diabetes, dipeptidyl peptidase 4 (DPP4) inhibitors. ATC code: A10BH07 evogliptin.
PHARMACOLOGY: Pharmacodynamics: Mechanism of action: Evogliptin tartrate inhibits plasma and tissue DPP4 enzyme activity which inactivates endogenous incretin hormones such as glucagon-like peptide-1 (GLP-1) through proteolytic cleavage of the N-terminus dipeptide, shortly after being secreted from intestinal L-cells (a half life of intact GLP-1, <2~3 min). Inhibition of DPP4 activity results in enhanced the plasma levels of intact GLP-1 according to nutrients ingestion leading to stimulating insulin secretion and consequently lowering blood glucose levels. Evogliptin forms interactions with the S1, S2 and S2 extensive subsites of DPP4 enzyme in a same orientation with sitagliptin. The interaction between evogliptin and DPP4 is reversible. Evogliptin has reduced hypoglycemic risk unlike other insulinogenic oral antidiabetic reagents because endogenous GLP-1 is secreted only when nutrients are ingested and thereby blood glucose rises, which was also confirmed in human trials. Evogliptin is weight neutral unlike sulfonylureas and glitazones that cause weight gain as an adverse effect related to the mechanism of action.
Clinical efficacy and safety: The clinical development program of Evogliptin for its clinical efficacy evaluation consisted of three studies in total: one Phase II Study and two phase III studies. The Phase II Study was a therapeutic exploratory study in type II diabetic patients, and the phase III studies were therapeutic confirmatory studies in type II diabetic patients. All clinical trials were conducted in compliance with the Good Clinical Practice (GCP).
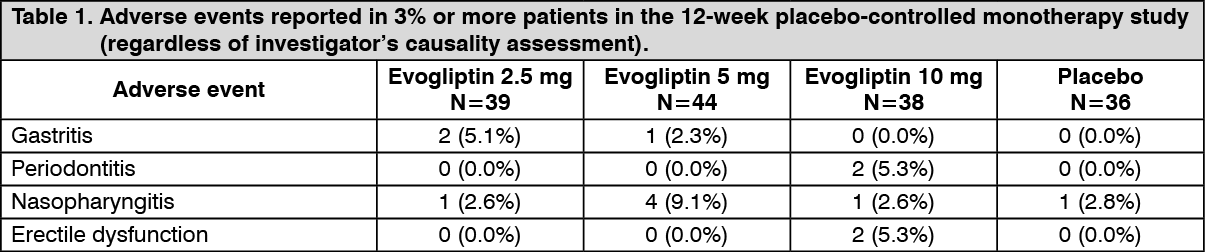
In the Phase II Study [DA1229_DM_II], type II diabetic patients were orally administered with Evogliptin (study drug, a DPP4 inhibitor) 2.5, 5, 10 mg, or placebo (control drug) once daily. The subjects who were found to be eligible at screening were randomized into Evogliptin 2.5 mg group, Evogliptin 5 mg group, Evogliptin 10 mg group or placebo group at 1:1:1:1 ratio. The study was designed as a double-blind trial. The primary efficacy endpoint was HbA1c and secondary efficacy endpoints were FPG, Fasting insulin, Fasting lipid parameters, HbA1c response rate, OGTT parameters, HOMA-β, HOMA-IR, QUICKI, Proinsulin/insulin ratio, Insulinogenic index, body weight and MDG. In the Phase III Combination Therapy Study [DA1229_DMC_III], type II diabetic patients whose glucose level was not sufficiently controlled with Metformin monotherapy were orally administered with either Evogliptin 5 mg (study drug) or Sitagliptin (control drug) in addition to Metformin once daily. The subjects who were found to be eligible at screening were randomized into either Evogliptin 5 mg group or Sitagliptin group at 1:1 ratio. The study was designed as double-blind trial. The primary efficacy endpoint was HbA1c and secondary efficacy endpoints were FPG, Fasting lipid parameters, HbA1c response rate, Rescue therapy rate, Fasting insulin, C-peptide, HOMA-β, HOMA-IR, QUICKI, body weight, MDG and body fat. The Phase III Monotherapy Study [DA1229_DMM_III] enrolled type II diabetic patients whose glucose level was not sufficiently controlled on exercise and diet, and they were orally administered with either Evogliptin 5 mg (study drug) or placebo (control drug) once daily under double-blind conditions. The subjects who were found to be eligible at screening were randomized into either Evogliptin 5 mg group or placebo control group at 1:1 ratio. The study was designed as double-blind trial. The primary efficacy endpoint was HbA1c and secondary efficacy endpoints were FPG, Fasting lipid parameters, HbA1c response rate, Rescue therapy rate, Fasting insulin, C-peptide, proinsulin, GLP-1, GIP, OGTT parameters, HOMA-β, HOMA-IR, QUICKI, Proinsulin/insulin ratio, Insulinogenic index, body weight, MDG and body fat.
[DA1229_DMC_III]: The non inferiority of evogliptin compared to sitagliptin was proven through the primary efficacy evaluation at Week 24 compared to Week 0 when evogliptin (Evogliptin) was co administered to the patients with type 2 diabetes mellitus who have inadequate glycemic control with metformin monotherapy. When it was co-administered with metformin for a long period of time, the change in HbA1c from Week 0 to Week 52 was -0.44 ± 0.65, demonstrating a clinically significant decrease (p <0.0001). In addition, no statistically significant difference was found in the comparison of the incidence of adverse events and adverse drug reactions by the SOC during the parent study period. The Evogliptin/Evogliptin group showed nothing notable in the long term safety evaluation during the entire clinical study period of 52 weeks including the extension study period of 28 weeks, demonstrating its excellent safety and tolerability. Therefore, we believe the efficacy and safety of combination therapy of Evogliptin 5 mg once daily as a new antidiabetic drug was proven in patients with type 2 diabetes mellitus who have inadequate glycemic control with metformin monotherapy.
[DA1229_DMM_III]: The efficacy of Evogliptin 5 mg once daily regimen was proved to be superior to placebo in terms of HbA1c changes from baseline at Week 24, and even during long-term treatment, the change of HbA1c from baseline at Week 52 was -0.36±0.55, which is clinically significant (p<0.0001). In addition, no statistically significant difference was found in the incidence of adverse events and adverse drug reactions during the parent study period. In the long-term safety assessment, no particular finding was observed in the Evogliptin/Evogliptin group during the entire study period of 52 weeks including the extension study period of 28 weeks, demonstrating excellent safety and tolerability. Therefore, we believe that Evogliptin 5 mg once daily was confirmed as the optimal clinical dose and regimen to treat patients with type 2 diabetes mellitus who have inadequate glycemic control on diet and exercise.
Pharmacokinetics: Healthy adults: 1) Single dose administration [DA1229_DM_I]: The maximum Evogliptin concentrations were observed at 3.0-5.5 h (median value) after administration of Evogliptin 1.25, 2.5, 5, 10, 20, 40 and 60 mg, and the average half-lives (t½) were estimated to be 32.5-39.8h. The average Cmax and AUClast values increased as the dose increased. The average fractions excretion by urine (fe) were 0.18, 0.15, 0.17, 0.21, 0.26, 0.28 and 0.28, and the average renal clearance(CLR) levels were 2.9 L/h, 3.1 L/h, 4.1 L/h, 6.5 L/h, 9.2, L/h, 11.3 L/h and 12.3 L/h at dose levels of 1.25, 2.5, 5, 10, 20, 40 and 60 mg, respectively. Applied to the power model, Evogliptin showed linear pharmacokinetics at the 95% confidence interval of the slope of Cmax and AUClast of 0.94~1.07 and of 0.89~1.01. However, when comparing Cmax/dose and AUClast/dose using ANOVA, there were significant differences between dose groups (p=0.0244), not showing dose-linearity. Excluding 40 mg and 60 mg dosing-group, the pharmacokinetic linearity was confirmed between 1.25-20 mg with analysis using ANOVA.
2) Repeat administration study [DA1229_DM_I]: After multiple once a day administrations of Evogliptin, a steady state was achieved by Day 3 (48 h after the first dose) and Evogliptin was eliminated with a mean terminal elimination half-life of approximately 32.9 to 38.8 h at all dose levels. The plasma concentration reached a peak level at 4.0 to 5.0 h after drug administration at a steady state (Day 10).
In the MAD study, statistical analyses with the power regression model demonstrated dose proportionality of Evogliptin for AUClast and Cmax, as the estimates of the slope with a 95% confidence interval (CI) for AUClast and Cmax were 0.78~1.08 and 0.91~1.33, respectively. However, dose-normalized AUClast and Cmax analyses using ANOVA with a significance level of 0.05 did not confirm dose proportionality, as the p values for Cmax,ss/dose and AUCt,ss/dose were 0.080 and 0.0357, respectively.
3) Drug interaction with Metformin [DA1229_DIM_I]: Co-administration of Evogliptin 5 mg plus Metformin 1000 mg showed similar pharmacokinetics to administration of Evogliptin 5 mg alone or Metformin 1000 mg alone.
The extent of DPP-4 inhibition was comparable between co-administration of Evogliptin and Metformin, and administration of Evogliptin 5 mg alone. Evogliptin monotherapy showed a tendency to increase plasma active GLP-1 levels in comparison with pre-treatment of Evogliptin, which was considered due to the inhibition of DPP-IV activity. Following intake of 75 g of glucose, degree of increase of serum glucose, plasma insulin, C-peptide level as well as concentration of plasma glucagon in Evogliptin treatment group were decreased in comparison with those before administration of Evogliptin, which were considered due to the increase of active GLP-1 levels. Total GLP-1 levels in Evogliptin treatment group were decreased in comparison with those before administration of Evogliptin, which were considered due to the negative feedback from increased active GLP-1 levels. Co-administration of Evogliptin plus Metformin showed a tendency to increase active GLP-1 levels greatly in comparison with individual administration of Evogliptin or Metformin alone. It was considered because Metformin increased GLP-1 levels and Evogliptin decreased degradation of GLP-1 by inhibiting DPP-IV activity. Total GLP-1 levels after co-administration of Evogliptin plus Metformin were increased in comparison with those before the administration, which was a similar level with those after administration of Metformin. Following intake of 75 g of glucose, co-administration of Evogliptin plus Metformin showed the lowest degrees of increase in serum glucose and plasma insulin. The lowest degree of increase in C-peptide was found in Metformin monotherapy.
4) Drug interaction with Clarithromycin and Rifampicin [DA1229_DICR_I]: In healthy male adults, clarithromycin, a CYP3A4 inhibitor, approximately doubled AUClast and Cmax of Evogliptin when Evogliptin was administered once (log-transformed geometric mean ratio; 2.02 [90% CI, 1.93 - 2.13] (AUClast), 2.17 [90% CI, 1.97 - 2.38] (Cmax)).
Also, in healthy male adults, rifampicin, a CYP3A4 inducer, decreased AUClast of Evogliptin by about 63% when Evogliptin was administered once (log transformed geometric mean ratio; 0.37 [90% CI, 0.34 - 0.41]) but didn't cause any significant difference in Cmax (log-transformed geometric mean ratio; 1.03 [90% CI, 0.90 - 1.18]).
Since the adverse events that occurred when Evogliptin was concomitantly administered with clarithromycin or rifampicin were not associated with the investigational products and were not serious adverse events, the tolerability and safety of Evogliptin is deemed good when concomitantly administered with clarithromycin or rifampicin.
Renal impaired patients [DA1229_RI_I]: As a result of single oral administration of the study drug evogliptin 5 mg, it was observed that as the renal function decreased, the mean plasma concentration of evogliptin increased and the volume of evogliptin excreted in urine decreased. It was observed that the higher the drug concentration was, the higher the unbound fraction was. But the unbound fraction didn't show clear difference depending on renal function.
As a result of analyzing the pharmacokinetic parameters, it was found that there was a tendency that the lower the renal function was, the higher the pharmacokinetic parameters of evogliptin related to plasma drug exposure (Cmax, AUClast, and AUCinf) were and the lower the apparent clearance (CL/F) and the apparent volume of distribution (Vz/F) were. It was observed that the plasma drug exposure of the severe (Group 1) and moderate (Group 2) renal impairment groups was about 1.8 to 2 times higher compared to the healthy volunteers group (Group 4).
When the subject groups were classified based on MDRD eGFR, the GMRs of Cmax and AUClast and their 90% CIs were 1.52 (1.22 - 1.89), 1.98 (1.59 - 2.46) in the severe renal impairment group and 1.32 (1.08 - 1.61), 1.8 (1.47 - 2.21) in the moderate renal impairment group, respectively. In contrast, the plasma drug exposure observed in the mild renal impairment group was similar to that of the healthy volunteers group. The GMRs of Cmax and AUClast and their 90% CIs were 1.04 (0.85 - 1.27) and 1.2 (0.98 - 1.47) in the mild renal impairment group. The subject groups based on the Cockcroft-Gault eGFR showed similar GMRs of Cmax and AUClast and their 90% CIs.
Toxicology: Preclinical safety data: A safety pharmacology program compliant with GLP and ICH guidelines was conducted with evogliptin tartrate, encompassing central nervous system, respiratory, and cardiovascular systems.
A study of central nervous system effects after oral administration of evogliptin tartrate in rodents included body temperature and general behaviors including neurobehavior. Evogliptin tartrate did not produce any significant effects on general behavior and temperature at doses up to 300 mg/kg.
A study of respiratory function in rats was conducted at oral doses up to 300 mg/kg evogliptin tartrate. There were no statistically significant effects on respiratory parameters such as respiratory rate and tidal volume relative to vehicle controls, except a significant decrease in minute volume at 300 mg/kg 120 minutes after administration.
Studies in the cardiovascular system included evaluation of the human ether-à-go-go related gene (hERG) tail currents and electrocardiographic function in dogs. In the hERG patch clamp assay, the IC50 value of evogliptin tartrate was 143.4 μM (>9,000 folds vs. Cmax at the dose of 5 mg in humans from DA1229_DM_I). In dogs, evogliptin tartrate increased heart rate and changed several ECG parameters (shortened QT, QTcV and RR interval, elongated QRS interval) at 300 mg/kg, but did not affect blood pressure and temperature. These overall effects were restricted to high dose/concentration associated with evogliptin systemic exposure greatly exceeding those observed in humans.
In vitro assessment: Evogliptin is mainly metabolized by CYP3A4. In in vitro studies, evogliptin was not an inhibitor of CYP1A2, 2B6, 2C8, 2C9, 2C19, 2D6, and 3A4 enzymes or an inducer of CYP1A2, 2B6, and 3A4 enzymes. Thus, evogliptin is unlikely to cause interactions with other drugs acting as a substrate of such enzymes. Although evogliptin was proved to be a p-glycoprotein (P-gp) substrate and weak BCRP substrate based on in vitro studies, it did not inhibit transport mediated by these transporters. In addition, evogliptin was not a substrate of OAT1, OAT3, OCT2, OATP1B1, and OATP1B3, and did not inhibit them. Therefore, evogliptin is unlikely to cause interactions with drugs that act as a substrate of such transporters in the clinical dose.
In vivo assessment: Interaction of evogliptin with other drugs: i) Metformin: Multiple administration of evogliptin 5 mg and twice daily Metformin 1,000 mg (a substrate of OCT1 and OCT2) until steady state was reached did not show clinically meaningful change in the pharmacokinetics of evogliptin or Metformin.
ii) Clarithromycin: Multiple administration of a potent CYP3A4 inhibitor, clarithromycin 1,000 mg/day, until steady state was reached and single administration of evogliptin 5 mg showed increased Cmax of evogliptin by 2.1 times and its AUC by 2.0 times. Caution needs to be exercised as pharmacokinetic exposure of evogliptin may increase with concomitant administration of CYP3A4 inhibitors.
iii) Rifampicin: Multiple administration of a potent CYP3A4 inducer, rifampicin 600 mg/day, until steady state was reached and single administration of evogliptin 5 mg showed no significant change in Cmax of evogliptin but showed a decrease in AUC by 63%.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image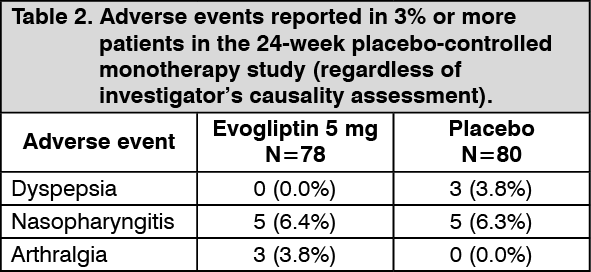 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image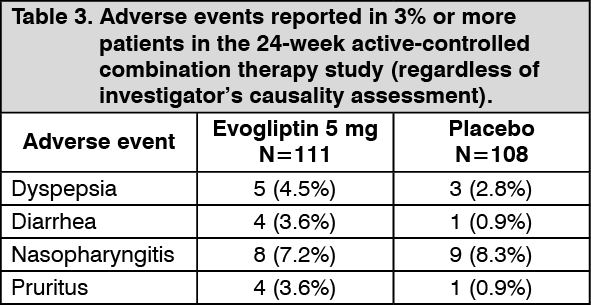 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out