The information highlighted (if any) are the most recent updates for this brand.
SUROTIN (10 MG TABLET): Each film-coated tablet contains Rosuvastatin calcium equivalent to Rosuvastatin 10 mg.
SUROTIN (20 MG TABLET): Each film-coated tablet contains Rosuvastatin calcium equivalent to Rosuvastatin 20 mg.
Pharmacology: Pharmacodynamics: Rosuvastatin calcium is synthetic heptenoic acid-derivative antilipemic agent. The drug is a selective, competitive inhibitor of 3-hydroxymethylglutaryl-CoA (HMG-CoA) reductase, an enzyme that catalyzes the conversion of HMG-CoA to mevalonate (an early and rate-limiting step in cholesterol biosynthesis). Rosuvastatin reduces total cholesterol, LDL-cholesterol, apolipoprotein B (apo B), non-HDL-cholesterol and triglyceride concentrations and increases HDL-cholesterol concentrations in patients with primary hyperlipidemia or mixed dyslipidemia. Rosuvastatin also reduces triglyceride concentration in patients with primary hypertriglyceridemia.
Pharmacokinetics: Rosuvastatin is incompletely absorbed from the gastrointestinal tract, with an absolute bioavailability of about 20%. Peak plasma concentrations occur about 5 hours after an oral dose. It is about 90% bound to plasma protein.
Rosuvastatin undergoes limited metabolized; approximately 10% of a radiolabeled dose is recovered as metabolite. The major metabolite is N-desmethyl rosuvastatin, which is formed principally by cytochrome P-450 (CYP) isoenzyme 2C9.
Based on in vitro studies, N-desmethyl rosuvastatin has approximately 17-50% of the HMG-CoA reductase inhibitory activity of the parent drug. The parent drug accounts for greater than 90% of the active plasma HMG-CoA reductase inhibitory activity.
Rosuvastatin and its metabolites are mainly eliminated in feces (90%) following oral administration. The elimination half-life of Rosuvastatin is approximately 19 hours.
Prevention of cardiovascular events: Rosuvastatin is used as an adjunct to non drug therapies in patients without clinical evidence of coronary heart disease (CHD) who have an increased risk of atherosclerotic cardiovascular disease based on age (men 50 years of age or older, women 60 years of age or older), high-sensitivity C-reactive protein (hsCRP) concentrations of 2 mg/L or greater, and at least on additional cardiovascular disease risk factor (e.g., hypertension, low HDL-cholesterol concentrations, smoking, family history of premature CHD).
Rosuvastatin is used to reduce total mortality and the risk of major cardiovascular events (cardiovascular death, stroke, myocardial infarction (MI), unstable angina, or undergoing arterial revascularization procedures).
Rosuvastatin is used to reduce progression of coronary atherosclerosis as adjunct to dietary therapy.
Dyslipidemias: Rosuvastatin is used as an adjunct to dietary therapy for the management of primary hyperlipidemia or mixed dyslipidemia, hypertriglyceridemia, primary dysbetalipoproteinemia and homozygous familial hypercholesterolemia.
Rosuvastatin is used as an adjunct to diet to reduce total cholesterol, LDL-C and apolipoprotein B (apo B) levels in patients with heterozygous familial hypercholesterolemia who are 6-17 years of age.
Mode of administration: Patients should be place on a standard cholesterol-lowering diet before receiving this drug and should continue on this diet during treatment.
The dose should be individualized according to the goal of therapy and patient response, using current consensus guidelines.
The recommended start dose is 5 or 10 mg once daily. Rosuvastatin is administered orally at any time of day, with or without food.
Recommended Dose: When initiating Rosuvastatin therapy or switching from another statin, the appropriate initial dosage of Rosuvastatin should be use; dosage may then be carefully adjusted according to individual requirements (i.e., percent reduction in LDL-cholesterol concentration) and response.
Adults: Prevention of cardiovascular disease: Initiation dosage is 5 to 40 mg once daily.
Patients who have risk of cardiovascular disease: Patient who have LDL-cholesterol levels ≥ 190 mg/dL: High-intensity therapy: The recommended dose is 20-40 mg once daily.
Patients 40-75 years with type 1 or 2 diabetes: Moderate-intensity therapy: The recommended dose is 5-10 mg once daily.
Patients with type 1 or 2 diabetes, age 40-75 years and an estimated 10 year ASCVD risk ≥ 7.5%: High-intensity therapy: The recommended dose is 20-40 mg once daily.
Patient 40-75 years and an estimated 10 year ASCVD risk ≥ 7.5%: Moderate to high intensity therapy: The recommended dose is 5-40 mg once daily.
Atherosclerotic cardiovascular disease patients (ASCVD) (e.g., coronary heart disease, stroke/TIA or peripheral arterial disease and: Age ≤ 75 years: High-intensity therapy: The recommended dose is 20-40 mg once daily.
Age ≥ 75 years or not a candidate for high-intensity therapy: The recommended dose is 5-10 mg once daily.
Dyslipidemias: The usual initial dosage of Rosuvastatin in adults is 10-20 mg once daily.
The usual dosage range of Rosuvastatin in adults is 5-40 mg once daily.
The 40 mg daily dosage of Rosuvastatin should be used only for those patients who have not achieved their LDL-cholesterol goal with the 20 mg daily dosage.
Following initiation and/or titration of Rosuvastatin dosage, lipoprotein concentrations should be determined within 2-4 weeks and dosage adjusted accordingly.
The recommended initial dose of Rosuvastatin in adults with homozygous familial hypercholesterolemia is 20 mg once daily.
Dosage in pediatric patients: The usual dosage range of Rosuvastatin for the management of heterozygous familial hypercholesterolemia in boys and girls 6-9 years of age is 5-10 mg once daily.
The usual dosage range of Rosuvastatin for the management of heterozygous familial hypercholesterolemia in boys and girls 10-17 years of age is 5-20 mg once daily.
The recommended starting dose is 5 mg once daily. Increased plasma concentration of Rosuvastatin has been seen in Asian subjects.
Dosage in renal impairment: No dose adjustment in patient with CrCl ≥ 30 mL/minute/1.73 m2.
Rosuvastatin is contraindicated in patients with severe renal impairment (CrCl < 30 mL/minute/1.73 m2).
Dosage in hepatic impairment: In patients with Child-Pugh scores of 7 or below, there was no increase in systemic exposure to Rosuvastatin. However, increased systemic exposure has been observed in subjects with Child-Pugh scores of 8 and 9.
Rosuvastatin is contraindicated in patients with active liver disease.
Dosage in elderly: Although there are no specific dosage recommendation for geriatric patients, caution is recommended when Rosuvastatin is used in these patients.
Overdose and Treatment: There is no specific treatment in the event of overdose. In the event of overdose, the patient should be treated symptomatically and supportive measures instituted as required. Liver function and CK levels should be monitored. Hemodialysis is unlikely to be of benefit.
This drug is contraindicated: In patients with hypersensitivity to Rosuvastatin or any ingredients in the formulation; in patients with active liver disease, including unexplained, persistent elevations in hepatic aminotransferase (transaminase) concentrations; in women who are or may become pregnant; in nursing women; in patients with severe renal impairment (creatinine clearance < 30 ml/min/1.73 m2); in patients with myopathy; in patients receiving concomitant cyclosporin.
1. Rosuvastatin is contraindicated in nursing women and women who are or may become pregnant.
2. Rosuvastatin is contraindicated in patient with active liver disease.
3. If sign of myalgia, back pain occurred, discontinue medication and inform physicians immediately.
4. It is recommended that liver function tests be performed before and at 6, 12 weeks following the initiation of therapy. In patients with long term use of Rosuvastatin, liver function test should be performed every 6 months or as directed by physicians. Rosuvastatin should be discontinued and consult your physician if the level of serum transaminase is 3 times greater than the upper normal limit.
5. Concomitant use of Rosuvastatin and warfarin or digoxin may increase warfarin or digoxin concentrations. Use with caution.
6. Increased risk of myopathy or rhabdomyolysis when co-administered with drug e.g. azole antifungals (e.g., ketoconazole, itraconazole), macrolides antibacterial (e.g., erythromycin, clarithromycin), HIV protease inhibitors (e.g., indinavir, ritonavir, nelfinavir, saquinavir), verapamil, diltiazem, gemfibrozil, nicotinic acid, cyclosporine, amiodarone.
7. Increased risk of rhabdomyolysis in geriatric patients, hepatic or renal dysfunction, chronic alcoholic patients and patients with hypothyroidism.
8. Use with caution when co-administered with colchicine especially in geriatric patients or patients with renal dysfunction due to the risk of myopathy or rhabdomyolysis.
9. This drug may increase risk of hyperglycemia.
Hepatic effect of Rosuvastatin; increase in serum aminotransferase [i.e., AST (SGOT), ALT (SGPT)] concentration have been reported in patients receiving statins, including Rosuvastatin. These increases usually were transient and resolved or improved with continued therapy or after interruption of therapy.
Liver function test should be performed prior to initiation of Rosuvastatin therapy. And liver function test should be repeated as clinically indicated (e.g., presence of manifestations suggestion of liver damage).
If serious liver injury with clinical manifestations and/or hyperbilirubinemia or jaundice occurs, Rosuvastatin therapy should be promptly interrupted. If an alternate etiology is not found, Rosuvastatin therapy should not be restarted.
Rosuvastatin should be used with caution in patients who consume substantial amounts of alcohol and/or have a history of chronic liver disease.
Rosuvastatin is contraindicated in patients with active liver disease, including unexplained, persistent elevations in serum aminotransferase concentration.
Myopathy and rhabdomyolysis with acute renal failure secondary to myoglobinuria have been reported in patients receiving statins, including Rosuvastatin. These adverse effects can occur at any dosage, but the risk is increased with the highest dosage of Rosuvastatin (40 mg daily).
Rosuvastatin should be used with caution in patients with predisposing factors for myopathy (e.g., advance age (65 years old), renal impairment, inadequately treated hypothyroidism). The risk of myopathy may be increased when Rosuvastatin is used concomitantly with other antilipemic agents (niacin or certain is used fibric-acid derivatives [i.e., gemfibrozil]), cyclosporine or other myotoxic drugs (e.g., colchicine).
It is reasonable to obtain baseline CK concentrations in adult at increased risk of developing adverse musculoskeletal effect before initialing statin therapy. During statin therapy, it is reasonable to measure CK concentration in adults experiencing muscle symptoms (e.g., pain, tenderness, stiffness, cramping, and weakness).
Rosuvastatin should be discontinued if CK concentrations become markedly elevated or if myopathy is diagnosed or suspected. Rosuvastatin therapy should be temporarily withheld in any patients experiencing an acute, serious condition suggestive of myopathy or predisposing to the development of renal failure secondary to rhabdomyolysis (e.g., sepsis, hypotension, dehydration, major surgery, trauma, severe metabolic, endocrine, or electrolyte disorder, uncontrolled seizures).
Proteinuria and hematuria has been reported in patients receiving Rosuvastatin. This finding was more frequent in patients taking Rosuvastatin 40 mg when compared to lower doses.
Pregnancy: Pregnancy category: X.
Use of Rosuvastatin is contraindicated in pregnancy because cholesterol products are essential for fetal development; therefore, suppression of cholesterol biosynthesis by Rosuvastatin during pregnancy may cause fetal harm.
Lactation: It is not known if Rosuvastatin is excreted into breast milk. Because of the potential for serious adverse reactions from Rosuvastatin in a nursing infant, the drug is contraindicated in nursing women.
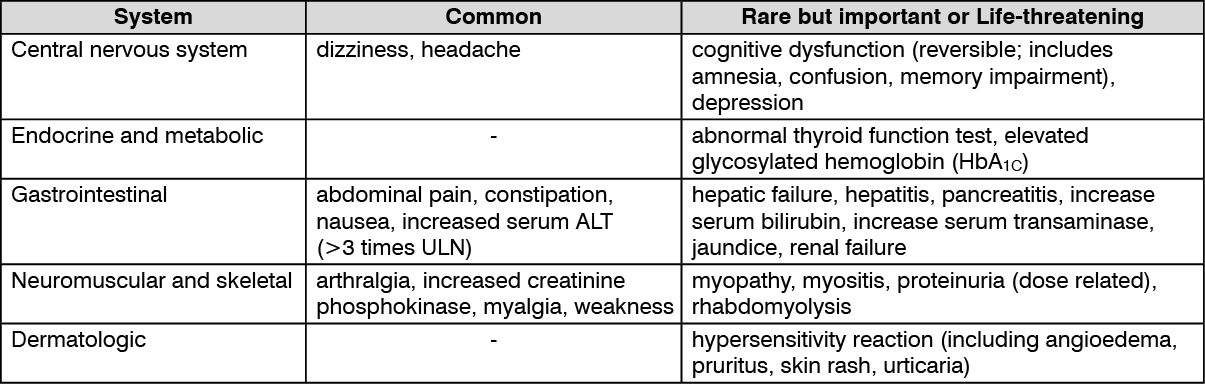
See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Rosuvastatin is minimally (approximately 10%) metabolized by cytochrome P-450 (CYP), isoenzyme 2C9. Clearance of Rosuvastatin is not dependent on metabolism by CYP3A4 to a clinically important extent.
Antacid: Administration of Rosuvastatin and an antacid containing aluminum hydroxide and magnesium hydroxide decreased Rosuvastatin peak plasma concentration by 50%, such effect was considered clinically important. Therefore, if Rosuvastatin and an aluminum hydroxide and magnesium hydroxide are used concomitantly, the antacid should be administered at least 2 hours after Rosuvastatin.
Cyclosporine: Concomitant use of Rosuvastatin and cyclosporine may increase the risk of myopathy. Following concomitant use of Rosuvastatin and cyclosporine, Rosuvastatin peak plasma concentration was clinically significantly increased. If used concomitantly with cyclosporin, dosage of Rosuvastatin should be limited to 5 mg once daily.
HIV Protease Inhibitors: Concomitant use of Rosuvastatin with certain ritonavir-boosted HIV protease inhibitors (e.g., atazanavir, fosamprenavir, lopinavir) would increase peak plasma concentration of Rosuvastatin. Caution and dose adjustment are advised if Rosuvastatin is used concomitantly with ritonavir-boosted HIV protease inhibitors.
Fibric acid derivative: Fenofibrate: Concomitant use of Rosuvastatin and fenofibrate may increase the risk of myopathy. Following concomitant use of Rosuvastatin and fenofibrate, Rosuvastatin peak plasma concentration was increased; such effect was not considered clinically important. However, caution is advised if Rosuvastatin is used concomitantly with fenofibrate.
Gemfibrozil: Concomitant use of Rosuvastatin and gemfibrozil may increase the risk of myopathy. Following concomitant use of Rosuvastatin and gemfibrozil, Rosuvastatin peak plasma concentration was increased by approximate 2 fold, such effect considered clinically important. Concomitant use should be avoided, if used concomitantly with gemfibrozil; dosage of Rosuvastatin should not exceed 10 mg once daily.
Oral contraceptive: Concomitant use of Rosuvastatin and oral contraceptive (ethinyl estradiol, norgestrel) resulted of increase ethinyl estradiol, norgestrel peak plasma concentration.
Warfarin: Concomitant use of Rosuvastatin and coumarin derivative anticoagulants e.g., Warfarin has been shown to substantially increase international normalised ratio (INR). If Rosuvastatin is used concomitantly with coumarin derivative anticoagulants, INR should be stable prior to initiating Rosuvastatin and should be monitored frequently enough during early therapy to ensure that no substantial alteration in INR occurs.
Other drugs: Niacin: Concomitant use of Rosuvastatin and niacin may increase the risk of myopathy. Caution is advised if Rosuvastatin is used concomitantly with antilipemic dosage of niacin.
Erythromycin: Concomitant use of Rosuvastatin and erythromycin decreased plasma concentrations of Rosuvastatin.
Azole antifungal: Concomitant use of Rosuvastatin and azole antifungal (i.e., fluconazole, itraconazole) increase plasma concentrations of Rosuvastatin but concomitant use Rosuvastatin and ketoconazole may decreased plasma concentrations of Rosuvastatin.
Digoxin: Concomitant use of Rosuvastatin and digoxin increase plasma concentrations of digoxin by 4%.
C10AA07 - rosuvastatin ; Belongs to the class of HMG CoA reductase inhibitors. Used in the treatment of hyperlipidemia.
Surotin FC tab 10 mg
3 × 10's
Surotin FC tab 20 mg
3 × 10's








 Sign Out
Sign Out