Pharmacotherapeutic Group: Antiglaucoma preparations and miotics, beta-blocking agents.
ATC Code: S01ED51.
Pharmacology: Pharmacodynamics: Tapcom: Intraocular pressure (IOP) lowering effect. Ocular administration of this product in a single dose to monkeys showed statistically significant IOP lowering effect. The effect was significantly greater than that of monotherapy containing individual active ingredients (i.e. 0.0015% tafluprost ophthalmic solution and 0.5% timolol ophthalmic solution).
Mechanism of action: Tafluprost carbonic acid, an active form of tafluprost, is an agonist to prostanoid FP receptor, and timolol maleate is a non-selective blocker to β adrenaline receptor. These active ingredients of this product lower IOP by the different modes of action.
Tafluprost acid form, an active metabolite of tafluprost, showed high affinity for the prostanoid FP receptor (Ki=0.40 nM). Aqueous humor dynamics in monkeys was evaluated using fluorophotometry, two-level constant pressure perfusion and
125I-
131I labeled albumin perfusion methods following the repeated administration of 0.005% tafluprost ophthalmic solution once daily for 3 to 5 days. Uveoscleral outflow was significantly increased without any change in aqueous production.
Mechanism of action of timolol maleate is not clear but it was suggested that the effect is caused mainly by decreasing aqueous production, which was demonstrated by the fluorophotometry study in monkeys and healthy subjects and the tonography test in glaucoma patients.
Tapcom-S: TAPCOM-S is a fixed combination of two active substances tafluprost and timolol. These two active substances lower intraocular pressure (IOP) by complementary mechanisms of action and the combined effect results in additional IOP reduction compared to either compound alone.
Tafluprost is a fluorinated analogue of prostaglandin F
2α. Tafluprost acid, the biologically active metabolite of tafluprost, is a highly potent and selective agonist of the human prostanoid FP receptor. Pharmacodynamic studies in monkeys indicate that tafluprost reduces intraocular pressure by increasing the uveoscleral outflow of aqueous humour.
Timolol maleate is a non-selective beta-adrenergic receptor blocking agent. The precise mechanism of action of timolol maleate in lowering intraocular pressure is not clearly established at this time, although a fluorescein study and tonography studies indicate that the predominant action may be related to reduced aqueous formation. However, in some studies a slight increase in outflow facility was also observed.
Tapcom: Effect on ocular blood flow: A repeated instillation of tafluprost ophthalmic solution 0.0015% into rabbit eyes once daily for 28 days significantly increased the blood flow in the optic nerve head, measured with laser speckle method.
A single dose instillation of tafluprost ophthalmic solution 0.0015% into eyes of healthy adults significantly increased the blood flow rate in the paraoptic nerve head retinal artery and the tissue blood flow at the paraoptic nerve head retina.
Tafluprost acid form, an active metabolite, showed high affinity for the prostanoid FP receptor (Ki=0.40 nM). Aqueous humor dynamics in monkeys was evaluated using fluorophotometry, two-level constant pressure perfusion and
125I-
131I labeled albumin perfusion methods following the repeated administration of 0.005% tafluprost ophthalmic solution once daily for 3 to 5 days. Uveoscleral outflow significantly increased without any change in aqueous production.
Effect on ocular blood flow: A repeated instillation of this product into rabbit eyes once daily for 28 days significantly increased the blood flow in the optic nerve head, measured with laser speckle method.
A single dose instillation of this product into eyes of healthy adults significantly increased the blood flow rate in the paraoptic nerve head retinal artery and the blood flow at the paraoptic nerve head retina.
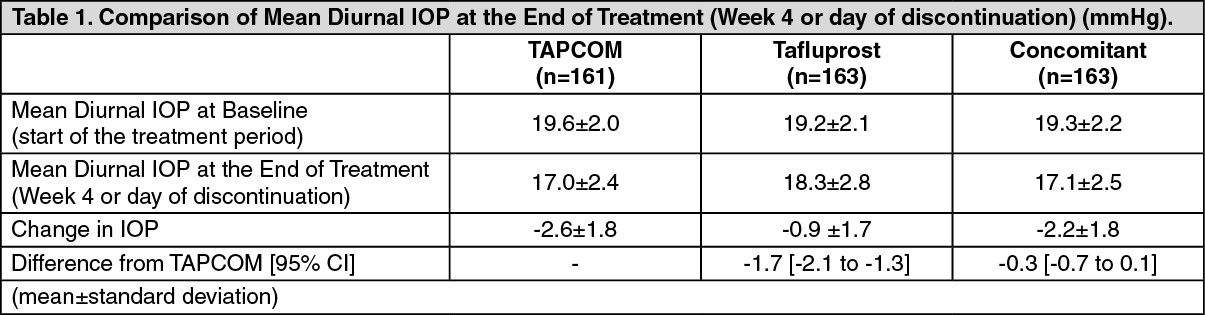
Clinical Studies: Tapcom: In a randomized masked comparison study in 487 patients with primary open angle glaucoma or ocular hypertension, using Tafluprost ophthalmic solution 0.0015% (once daily) (here after Tafluprost group) or concomitant Tafluprost ophthalmic solution 0.0015% (once daily) and Timolol ophthalmic solution 0.5% (twice daily) (here after Concomitant group) as a comparator, after instillation of Tafluprost ophthalmic solution 0.0015% (once daily) during 4 weeks of run-in period and instillation of TAPCOM (once daily) or each control drug in a double-masked manner during 4 weeks of treatment period, the superiority
of TAPCOM to Tafluprost group (p<0.001) and the non-inferiority to Concomitant group was confirmed (ANCOVA with baseline IOP as covariate). TAPCOM was confirmed to be non-inferior to Concomitant group in IOP
lowering (see Table 1 and Figure 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In a randomized masked comparison study in 166 patients with primary open angle glaucoma or ocular hypertension using Timolol ophthalmic solution 0.5% (twice daily) (here after Timolol group) as a comparator, after instillation of Timolol ophthalmic solution 0.5% (twice daily) during 4 weeks of run-in period and instillation of TAPCOM (once daily) or control drug in a double-masked manner during 4 weeks of treatment period, the superiority of TAPCOM to Timolol group was confirmed (p<0.001) (ANCOVA with baseline 1OP as covariate) (see Table 2 and Figure 2).
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In a long-term administration study in 136 patients with primary open angle glaucoma including normal tension glaucoma or ocular hypertension, TAPCOM was instilled during 52 weeks of treatment period following 4 weeks of run-in period with using Tafluprost ophthalmic solution 0.0015% (once daily). Timolol ophthalmic solution 0.5% (twice daily), or concomitant Tafluprost ophthalmic solution 0.0015% (once daily) and Timolol ophthalmic solution 0.5% (twice daily). In case of switching from Tafluprost ophthalmic solution 0.0015% (once daily) and Timolol ophthalmic solution 0.5% (twice daily), the IOP change form baseline (Week 0) was statistically significant at all measurement points (p<0.001). In case of switching from concomitant Tafluprost ophthalmic solution 0.0015% (once daily) and Timolol ophthalmic solution 0.5% (twice daily), no significant change in IOP was observed
throughout the treatment period compared with baseline (Week 0) and the time course of IOP remained stable during the 52 weeks (see Figure 3).
Click on icon to see table/diagram/image
Tapcom-S: In a 6-month study (n=400) in patients with open-angle glaucoma or ocular hypertension and mean untreated IOPs between 24-26 mmHg, the IOP lowering effect of TAPCOM-S (once daily in the morning) was compared to concomitant administration of 0.0015% tafluprost (once daily in the morning) and 0.5% timolol (twice daily). TAPCOM-S was non-inferior to the effect of concomitantly used 0.0015% tafluprost and 0.5% timolol at all time points and visits with the generally used non-inferiority margin of 1.5 mmHg. The mean diurnal IOP decrease from baseline was 8 mmHg in both arms at the primary endpoint of 6 months (decreases ranging between 7 to 9 mmHg in both arms at the different time points during the day over the study visits).
Another 6-month study (n=564) compared TAPCOM-S with the respective monotherapies in patients with open-angle glaucoma or ocular hypertension and mean untreated IOPs between 26-27 mmHg. Patients insufficiently controlled either with 0.0015% tafluprost (IOP 20 mmHg or greater on treatment) or 0.5% timolol (IOP 22 mmHg or greater on treatment) were randomized to be treated with TAPCOM-S or the same monotherapy. The mean diurnal IOP reduction of TAPCOM-S was statistically superior to that of tafluprost given once daily in the morning or timolol given twice daily, at visits 6 weeks, 3 months (primary efficacy endpoint) and 6 months. The mean diurnal IOP decrease from baseline of TAPCOM-S at 3 months was 9 mmHg, in comparison to 7 mmHg observed for both monotherapies. IOP decreases with TAPCOM-S at the different time points during the day over the visits ranged between 8 to 9 mmHg in the tafluprost monotherapy comparison group and between 7 to 9 mmHg in the timolol monotherapy comparison group.
Combined data from TAPCOM-S patients with high baseline IOP of 26 mmHg (mean diurnal) or above in these two pivotal studies (n=168) showed that the mean diurnal reduction in the IOP was 10 mmHg at the primary end point (3 or 6 months) ranging between 9 and 12 mmHg at the different time points during the day.
The European Medicines Agency has waived the obligation to submit the results of studies with TAPCOM-S in all subsets of the paediatric population.
Pharmacokinetics: Tapcom: This product is containing tafluprost and timolol maleate. Tafluprost is rapidly metabolized tafluprost acid which is an active form after ocular instillation.
Plasma concentrations: One drop of this product (once daily). 0.0015% tafluprost ophthalmic solution (once daily), 0.5% timolol ophthalmic solution (twice daily), and a combination of 0.0015% tafluprost ophthalmic solution (once daily)/0.5% timolol ophthalmic solution (twice daily) were instilled to both eyes of 32 healthy adult volunteers for 7 days and plasma concentrations of timolol and tafluprost acid which is an active metabolite of tafluprost were measured.
The C
max of tafluprost acid on the first and seventh day in the repeated instillation of this product were similar levels to that with the single use of tafluprost and the combination of tafluprost/timolol. The C
max and AUC
inf of timolol on the first and seventh day in the repeated instillation of this product were similar levels to that with the single use of timolol and the combination of tafluprost/timolol.
Pharmacokinetic parameters in once-daily repeated instillation of this product for 7 days. (See Table 3.)
Click on icon to see table/diagram/image
Ocular tissue distribution in animals: (For reference: Rats): The concentration profiles of tafluprost acid and timolol in aqueous humor following a single ocular instillation of this product to rats were similar to those in combination with a single ocular instillation of 0.5% timolol ophthalmic solution and 0.0015% tafluprost ophthalmic solution with 5-minute interval.
Biotransformation and elimination: Tafluprost acid, which is an active metabolite and rapidly generated by the hydrolysis of tafluprost following ocular instillation, is metabolized by -oxidation and then excreted into urine and bile, i.e. most of administered tafluprost is eliminated by metabolism. Timolol is absorbed after ocular instillation and metabolized by CYP2D6. Timolol is mainly excreted into urine but approximately 17% of dose is excreted as an unchanged form in urine.
Tapcom-S: Absorption: Plasma concentrations of tafluprost acid and timolol were investigated in healthy volunteers after single and repeated ocular dosing for eight days of TAPCOM-S (once daily), 0.0015% tafluprost (once daily) and 0.5% timolol (twice daily). Tafluprost acid plasma concentrations peaked at 10 minutes after dosing and declined below the lower limit of detection (10 pg/ml) before 30 minutes after TAPCOM-S dosing. Accumulation of tafluprost acid was negligible and the tafluprost acid mean AUC
0-last (monotherapy: 4.45±2.57 pg·h/ml; TAPCOM-S: 3.60±3.70 pg·h/ml) and the mean C
max (monotherapy: 23.9±11.8 pg/ml; TAPCOM-S: 18.7±11.9 pg/ml) were both slightly lower with TAPCOM-S as compared to tafluprost monotherapy on Day 8. Timolol plasma concentrations peaked at median T
max values of 15 and 37.5 minutes after TAPCOM-S dosing on Days 1 and 8, respectively. The Day 8 timolol mean AUC
0-last (monotherapy: 5750±2440 pg·h/ml; TAPCOM-S:4560±2980 pg·h/ml) and the mean C
max (monotherapy: 1100±550 pg/ml; TAPCOM-S: 840±520 pg/ ml) were both somewhat lower with TAPCOM-S compared to timolol monotherapy. The lower plasma timolol exposure with TAPCOM-S appears to be due to once-daily dosing for TAPCOM-S versus twice daily dosing with timolol monotherapy. Tafluprost and timolol are absorbed through the cornea. In rabbits, corneal penetration of tafluprost from TAPCOM-S was similar to that of tafluprost monopreparation after a single instillation while the penetration of timolol was slightly less from the TAPCOM-S compared to timolol monopreparation. For tafluprost acid, AUC
4h was 7.5 ng·h/ml following administration of TAPCOM-S and 7.7 ng·h/ml following administration of tafluprost monopreparation. For timolol, AUC
4h was 585 ng·h/ml and 737 ng·h/ml following administration of TAPCOM-S and timolol monopreparation, respectively. T
max for tafluprost acid was 60 minutes for both TAPCOM-S and tafluprost monopreparation, while for timolol T
max was 60 minutes for TAPCOM-S and 30 minutes for timolol monopreparation.
Distribution: Tafluprost: In monkeys, there was no specific distribution of radiolabelled tafluprost in the iris-ciliary body or choroid including retinal pigment epithelium, which suggested low affinity for melanin pigment. In a whole body autoradiography study in rats, the highest concentration of radioactivity was observed in the cornea followed by the eyelids, sclera and the iris. Outside the eye radioactivity was distributed to the lacrimal apparatus, palate, oesophagus and gastrointestinal tract, kidney, liver, gall bladder and urinary bladder. The binding of tafluprost acid to human serum albumin
in vitro was 99% at 500 ng/ml tafluprost acid.
Timolol: The peak level of timolol-related radioactivity in the aqueous humor was reached after 30 minutes following a single application of
3H-radiolabelled timolol (0.5% solution: 20 μl/eye) to both eyes in rabbits. Timolol is eliminated from the aqueous humor much faster than from the pigmented tissues iris and ciliary body.
Metabolism: Tafluprost: The principal metabolic pathway of tafluprost in human, which was tested
in vitro, is the hydrolysis to the pharmacologically active metabolite, tafluprost acid, which is further metabolized by glucuronidation or beta-oxidation. Products of beta-oxidation, 1,2-dinor and 1,2,3,4-tetranor tafluprost acids, which are pharmacologically inactive, may be glucuronidated or hydroxylated. Cytochrome P450 (CYP) enzyme system is not involved in the metabolism of tafluprost acid. Based on the study in rabbit corneal tissue and with purified enzymes, the main esterase responsible for the ester hydrolysis to tafluprost acid is carboxyl esterase. Butylcholine esterase but not acetylcholine esterase may also contribute to the hydrolysis.
Timolol: Timolol is metabolized in the liver primarily by CYP2D6 enzyme into inactive metabolites, which are excreted primarily through the kidneys.
Elimination: Tafluprost: Following once daily administration of
3H-tafluprost (0.005% ophthalmic solution; 5 μl/eye) for 21 days to both eyes in rats, approximately 87% of the total radioactive dose was recovered in the excreta. Percent of the total dose excreted in urine was approximately 27-38% and approximately 44-58% of the dose was excreted in the feces.
Timolol: Apparent elimination half-life from the human plasma is about 4 hours. Timolol is extensively metabolised in the liver and the metabolites are excreted in the urine in addition to 20 % unchanged timolol following oral administration.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image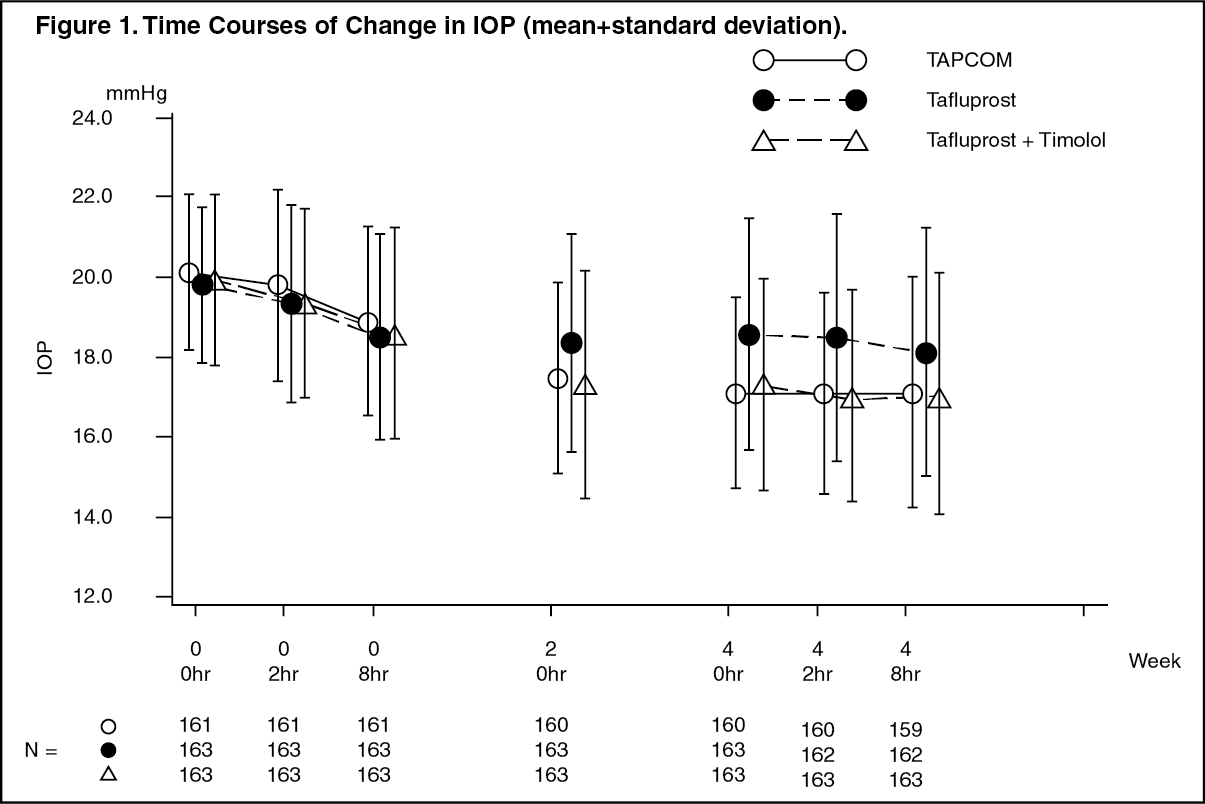 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image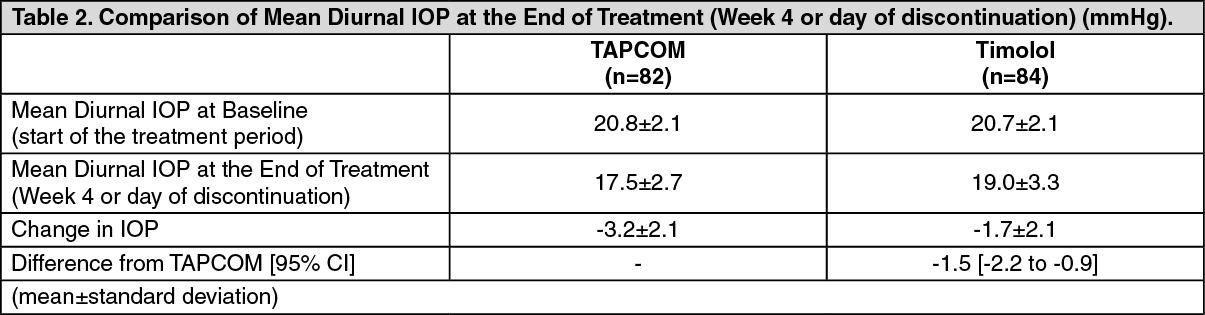 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image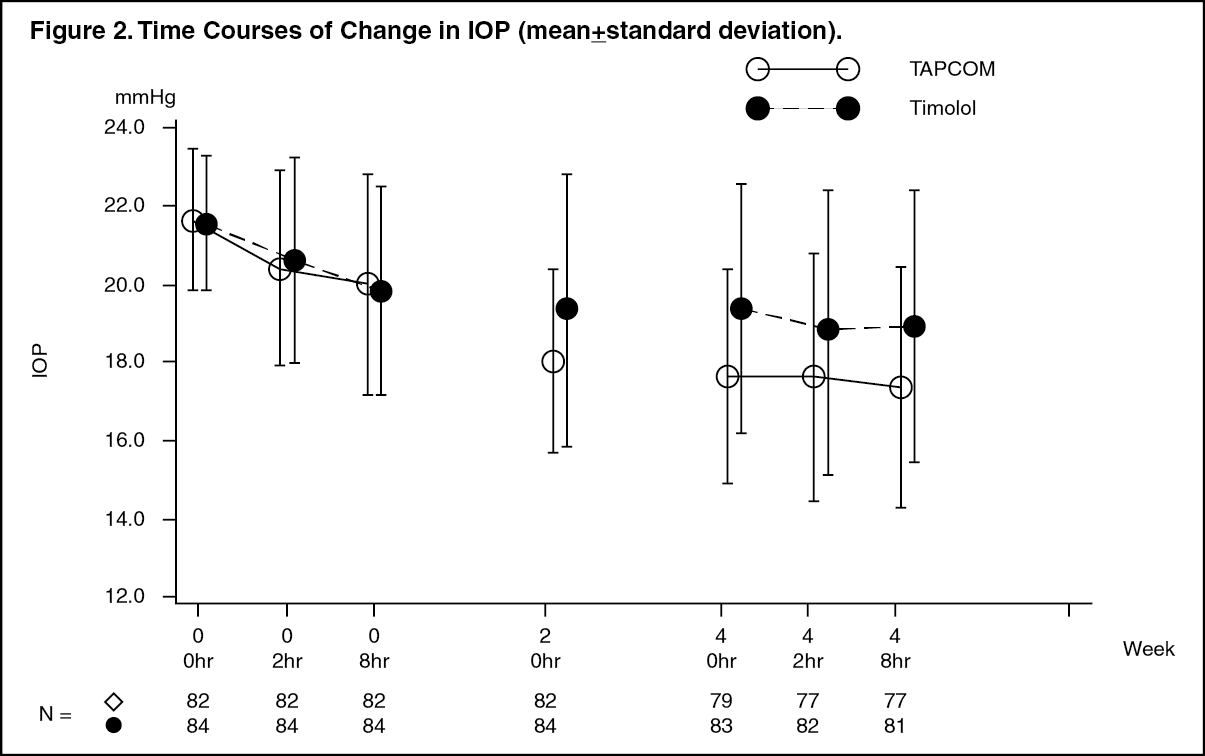 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image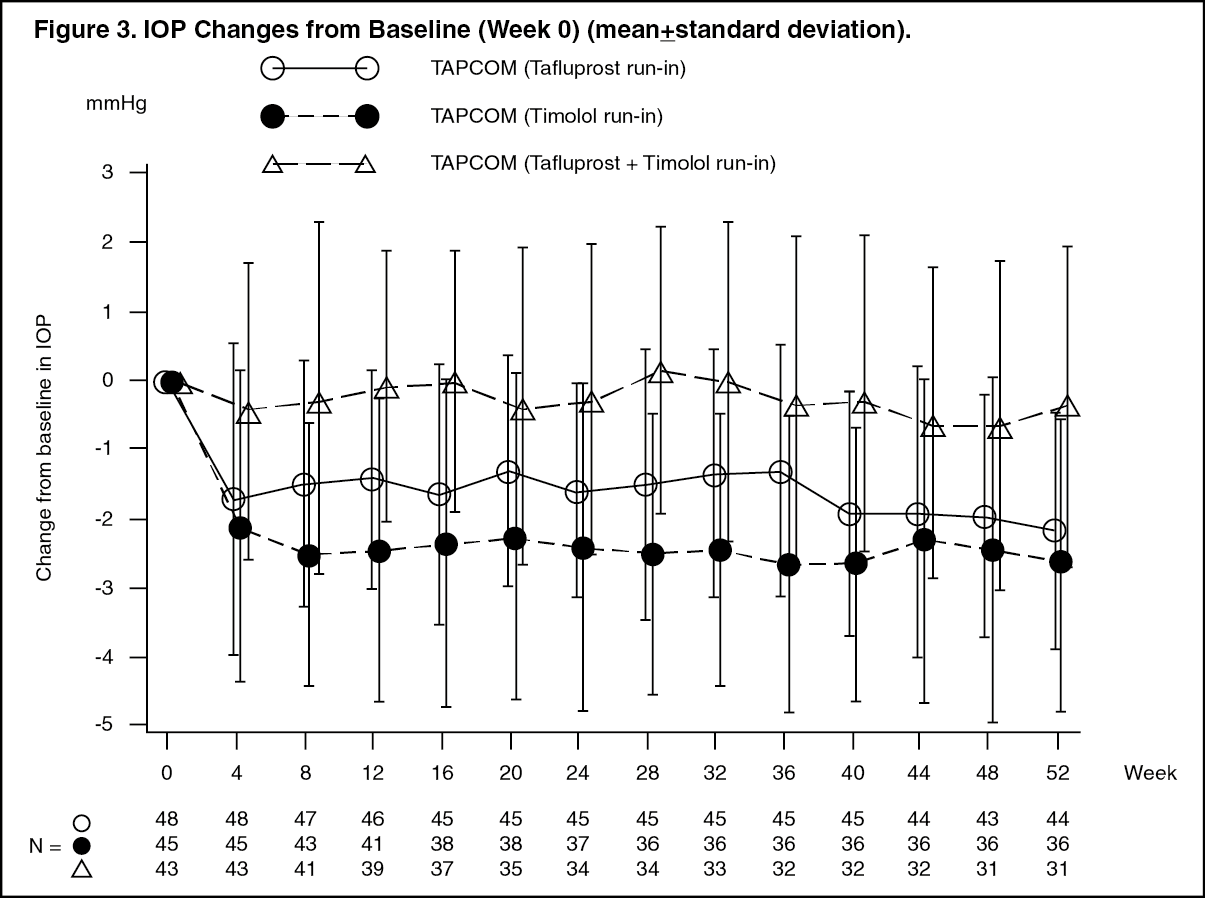 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out