In general, the incidence and severity of side effects are considered to be related to the dose, the dosing frequency, the method of administration and the duration of exposure.
Most adverse reactions are reversible if detected early. When adverse reactions do occur, the drug should be reduced in dosage or discontinued and appropriate corrective measures should be taken. This includes the use of calcium folinate (see Dosage & Administration and Precautions). Methotrexate therapy should only be resumed with particular caution, after careful consideration of the need for treatment and with increased vigilance for the possible recurrence of toxicity.
Most serious adverse reactions of methotrexate include bone marrow suppression, pulmonary toxicity, hepatotoxicity, renal toxicity, neurotoxicity, thromboembolic events, anaphylactic shock and Stevens-Johnson syndrome.
Most frequently observed adverse reactions of methotrexate include gastrointestinal disorders (e.g. stomatitis, dyspepsia, abdominal pain, nausea, loss of appetite) and abnormal liver function tests (e.g. increased Alanine aminotransferase (ALAT), Aspartate aminotransferase (ASAT), bilirubin, alkaline phosphatase). Other frequently occurring adverse reactions are leukopenia, anaemia, thrombocytopenia, headache, tiredness, drowsiness, pneumonia, interstitial alveolitis/pneumonitis often associated with eosinophilia, oral ulcers, diarrhoea, exanthema, erythema and pruritus.
The most relevant adverse reaction is suppression of the haematopoietic system and gastrointestinal disorders.
In the antineoplastic treatment, myelosuppression and mucositis are the predominant dose-limiting toxic effects of methotrexate. The severity of these reactions depends on the dose, mode and duration of application of methotrexate. Mucositis generally appears about 3 to 7 days after methotrexate application, leucopenia and thrombocytopenia follow a few days later. In patients with unimpaired elimination mechanisms, myelosuppression and mucositis are generally reversible within 14 to 28 days.
Adverse reactions for the various systems are as follows:
Skin and subcutaneous tissue disorders: Exanthema, Stevens-Johnson Syndrome, toxic epidermal necrolysis, erythematous rashes, pruritus, urticaria, photosensitivity, pigmentary changes, erythema multiforme, onycholysis, increased pigmentation, petechia, allergic vasculitis, hidradenitis, alopecia, depigmentation, ecchymosis, telangiectasia, acne, furunculosis, painful damage to psoriatic lesions, skin ulceration, herpetiform eruptions of the skin, hyperpigmentation of the nails and acute paronychia. Skin exfoliation and dermatitis exfoliative (frequency not known).
The recall phenomenon has been reported in both radiation and solar damaged skin. Lesions of psoriasis may worsen with concomitant UV therapy. Radiation dermatitis and sunburn may be "recalled".
Blood and the lymphatic system disorders: Megaloblastic anaemia, hematopoietic disorders, eosinophilia, lymphoproliferative disorder (partly reversible), lymphadenopathy, bone marrow depression (especially at high-dose of methotrexate) is most frequently manifested by thrombocytopenia (which are usually reversible), neutropenia, leukopenia, pancytopenia, agranulocytosis, anaemia, aplastic anaemia, immunosuppression, lymphoproliferative disorders (frequency very rare) or any combination may occur. Infection or hypogammaglobulinaemia, haemorrhage from various sites. Bone marrow depression may lead to decreased resistance to infection and sepsis.
Gastrointestinal disorder: Mucositis, stomatitis, gingivitis, hematemesis, melena, pancreatitis, enteritis, gastrointestinal ulceration (including oral ulcers) and bleeding, malabsorption, toxic mega-colon, dyspepsia, abdominal pain, anorexia, nausea, vomiting, diarrhoea.
Gastrointestinal disorders frequently require dosage adjustment. Ulcerative stomatitis and diarrhoea require interruption of therapy; otherwise hemorrhagic enteritis and death from intestinal perforation may occur.
Hepatobiliary disorders: Hepatic toxicity resulting in increase of transaminases (ASAT, ALAT), alkaline phosphatase and bilirubin, decrease in serum albumin, acute hepatitis, periportal fibrosis or hepatic cirrhosis, hepatic failure, fatty degeneration of liver, reactivation of chronic hepatitis or death.
Renal and urinary disorders: Renal failure, uraemia, ulceration of the urinary bladder, disturbed micturition, oliguria, haematuria, dysuria, anuria, proteinuria, electrolyte disturbance, nephropathy.
Respiratory, thoracic and mediastinal disorders: Pneumonia, acute or chronic interstitial alveolitis/pneumonia which can be fatal and is often associated with eosinophilia, acute pulmonary oedema, interstitial/pulmonary fibrosis, chronic interstitial obstructive pulmonary disease, pharyngitis, pleurisy, non-productive cough, thoracic pain, dyspnoea, pleural effusion, bronchial asthma, respiratory paralysis.
In the treatment of rheumatoid arthritis, Methotrexate induced lung disease is a potentially serious adverse drug reaction which may occur acutely at any time during therapy. It is not always fully reversible.
Epistaxis (frequency not known) has been reported. Pulmonary alveolar haemorrhage (frequency not known) has been reported for methotrexate used in rheumatologic and related indications.
Nervous system disorders: Headaches, fatigue, drowsiness, dizziness, vertigo, lethargy, aphasia, irritability, hemiparesis, paresis, convulsions, encephalopathy/leukoencephalopathy.
Leukoencephalopathy has been reported especially following intravenous Methotrexate in high doses, or low doses following cranial-spinal radiation.
Cerebral oedema, transient subtle cognitive dysfunction, dysarthria, unusual cranial sensations.
Pain, muscular asthenia, changes in sense of taste (metallic taste), meningism, acute aseptic meningitis, paralysis.
Paraesthesia, hypoaesthesia (frequency very rare).
Psychiatric disorders: Depression, confusion, mood alterations, insomnia, psychoses.
Cardiac disorder: Percardial effusion, pericarditis, pericardial tamponade.
Vascular disorders: Thromboembolic events (arterial thrombosis, cerebral thrombosis, deep vein thrombosis, retinal vein thrombosis, thrombophlebitis, pulmonary embolus), vasculitis, hypotension.
Eye disorders: Conjunctivitis, blurred/impaired vision, retinopathy.
Neoplasms benign, malignant and unspecified (including cysts and polyps): Lymphoma, which can be reversible, Methotrexate may trigger tumour lysis syndrome in patients with rapidly growing tumour.
Reproductive system and breast disorder: Gynecomastia, decreased libido/impotence, defective oogenesis or spermatogenesis, transient oligospermia, infertility, menstrual dysfunction, vaginal bleeding, vaginal ulceration, inflammation of the vagina, vaginal discharge.
Infections and infestations: Respiratory or cutaneous bacterial infections, herpes zoster infections, opportunistic infections,
Pneumocystis carinii/
jiroveci pneumonia and other lung infection, reactivation of inactive chronic infection.
Musculoskeletal, connective tissue and bone disorders: Osteoporosis, stress fractures, arthralgia/myalgia, increased rheumatic nodules. Osteonecrosis of jaw (frequency not known) (secondary to lymphoproliferative disorders).
Endocrine disorders: Diabetes mellitus.
Immune system disorders: Allergic reaction, anaphylactic reaction, anaphylactic shock.
Ear and labyrinth disorders: Tinnitus.
General disorders and administration site conditions: Fever, chills, wound healing impairment, asthenia. Oedema (frequency not known).
Other: Increased risk of toxic reactions in radiotherapy (soft tissue necrosis, osteonecrosis).




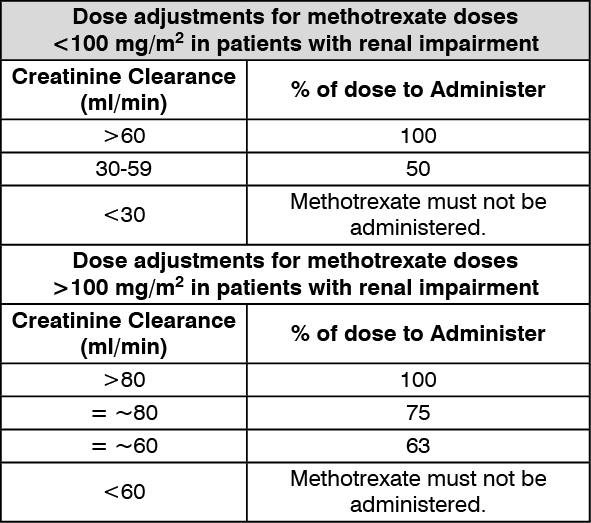 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
