


 Sign Out
Sign Out

Prior to the initiation of treatment, LVEF must be evaluated to ensure that the baseline LVEF is within the institutional limits of normal (see Precautions). LVEF must continue to be monitored during treatment with Tykerb to ensure that LVEF does not decline below the institutional lower limit of normal (see Dose Delay and Dose Reduction: Cardiac Events as follows).
Tykerb should be taken at least 1 hr before or at least 1 hr after food (see Pharmacology: Pharmacokinetics: Absorption under Actions and Interactions).
Missed doses should not be replaced and the dosing should resume with the next scheduled daily dose (see Overdosage).
Consult the full prescribing information of the co-administered medicinal product for relevant details of their dosage and administration, contraindications and safety information.
In Combination with Capecitabine: Recommended Dose: 1250 mg (5 tabs) once daily continuously with capecitabine.
The recommended dose of capecitabine is 2000 mg/m2/day taken in 2 doses 12 hrs apart on days 1-14 in a 21-day cycle (see Pharmacology: Clinical Studies under Actions). Capecitabine should be taken with food or within 30 min after food.
In Combination with Trastuzumab: Recommended Dose: 1000 mg (4 tabs) once daily continuously in combination with trastuzumab.
The recommended dose of trastuzumab is 4 mg/kg administered as an IV loading dose, followed by 2 mg/kg IV weekly (see Pharmacology: Clinical Studies under Actions).
In Combination with Paclitaxel: Recommended Dose: 1500 mg (6 tabs) once daily continuously in combination with paclitaxel.
When co-administered with Tykerb, the recommended dose of paclitaxel is 80 mg/m2 on days 1, 8 and 15 of a 28-day schedule. Alternatively, paclitaxel may be given at a dose of 175 mg/m2 every 21 days (see Pharmacology: Clinical Studies under Actions).
In Combination with an Aromatase Inhibitor: Recommended Dose: 1500 mg (6 tabs) once daily continuously when taken in combination with an aromatase inhibitor.
When Tykerb is co-administered with the aromatase inhibitor letrozole, the recommended dose of letrozole is 2.5 mg once daily. If Tykerb is co-administered with an alternative aromatase inhibitor, please refer to the FPI of the medicinal product for dosing details.
Dose Delay and Dose Reduction: Cardiac Events (see Precautions): Tykerb should be discontinued in patients with symptoms associated with decreased LVEF that are National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) ≥grade 3 or if their LVEF drops below the institutions lower limit of normal. Tykerb may be restarted at a lower dose (reduced from 1000 mg/day to 750 mg/day, from 1250 mg/day to 1000 mg/day or from 1500 mg/day to 1250 mg/day) after a minimum of 2 weeks, and if the LVEF recovers to normal and patient is asymptomatic. Based on current data, the majority of LVEF decreases occur within the first 12 weeks of treatment, however, there is limited data on long-term exposure.
Interstitial Lung Disease/Pneumonitis (see Precautions and Adverse Reactions): Tykerb should be discontinued in patients who experience pulmonary symptoms indicative of interstitial lung disease/pneumonitis which are NCI CTCAE ≥grade 3.
Diarrhea (see Precautions and Adverse Reactions): Tykerb dosing should be interrupted in patients with diarrhea which is NCI CTCAE grade 3 or grade 1 or 2 with complicating features (moderate to severe abdominal cramping, nausea or vomiting greater than or equal to NCI CTCAE grade 2, decreased performance status, fever, sepsis, neutropenia, frank bleeding or dehydration). Tykerb may be reintroduced at a lower dose (reduced from 1000 mg/day to 750 mg/day, from 1250 mg/day to 1000 mg/day or from 1500 mg/day to 1250 mg/day) when diarrhea resolves to ≤grade 1. Tykerb dosing should be permanently discontinued in patients with diarrhea which is NCI CTCAE grade 4.
Other Toxicities: Discontinuation or interruption of dosing with Tykerb may be considered when a patient develops toxicity ≥grade 2 on the NCI CTCAE. Dosing can be restarted at the standard dose of 1000 mg/day, 1250 mg/day or 1500 mg/ day, when the toxicity improves to ≤grade 1. If the toxicity recurs, then Tykerb should be restarted at a lower dose (reduced from 1000 mg/day to 750 mg/day, from 1250 mg/day to 1000 mg/day or from 1500 mg/day to 1250 mg/day).
Population: Renal Impairment: There is no experience of Tykerb in patients with severe renal impairment, however, patients with renal impairment are unlikely to require dose modification of Tykerb given that <2% of an administered dose (lapatinib and metabolites) is eliminated by the kidneys (see Pharmacology: Pharmacokinetics Special Patient Populations under Actions).
Hepatic Impairment: Lapatinib is metabolised in the liver. Moderate and severe hepatic impairment have been associated with 56% and 85% increases in systemic exposure, respectively. Administration of Tykerb to patients with hepatic impairment should be undertaken with caution due to increased exposure to the drug. (See Pharmacology: Pharmacokinetics under Actions and Precautions.)
Patients with severe hepatic impairment (Child-Pugh class C) should have their dose of Tykerb reduced. A dose reduction from 1250 mg/day to 750 mg/day or from 1500 mg/day to 1000 mg/day in patients with severe hepatic impairment is predicted to adjust the AUC to the normal range. However, there is no clinical data with this dose adjustment in patients with severe hepatic impairment (see Pharmacokinetics: Special Patient Populations under Actions and Precautions).
Elderly: There are limited data on the use of Tykerb in patients ≥65 years. (See Table 11.)
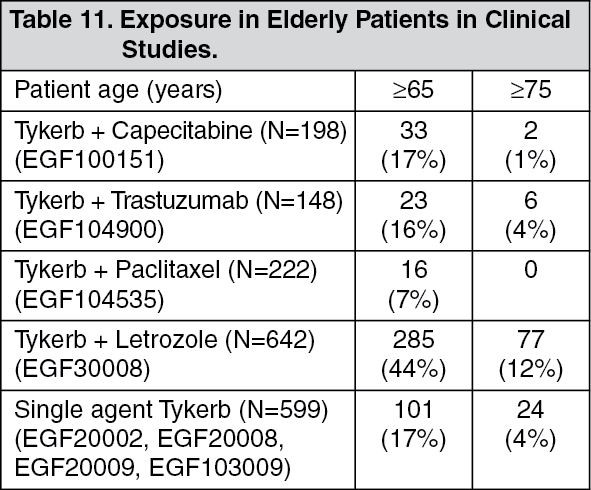 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageNo overall differences in the safety or efficacy of these regimens on the basis of age were observed. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. Greater sensitivity of elderly individuals cannot be ruled out.