Pharmacology: Pharmacodynamics: Mechanism of Antihypertensive Action: In the absorption process in the body, candesartan cilexetil is rapidly hydrolyzed to the active metabolite candesartan, which exerts its antihypertensive action primarily by inhibiting the potent vasoconstrictor effect of angiotensin II through its antagonistic action at the angiotensin II type 1 (AT
1) receptor in vascular smooth muscle, thereby reducing peripheral vascular resistance. In addition, inhibitory effect on the release of aldosterone from adrenal gland mediated by AT
1 receptor is considered to play a role in the antihypertensive action. Amlodipine besilate acts as a dihydropyridine calcium channel antagonist, and is characterized by gradual onset of action and continuous effect.
Dihydropyridine calcium channel antagonist selectively binds to the membrane potential-dependent L-type calcium channels and reduces calcium influx into cells, causing relaxation of coronary or peripheral vascular smooth muscle.
Effect on the Renin-Angiotensin System: When candesartan cilexetil was administered repeatedly at a once daily dose of 1-12 mg to 74 hypertensive patients (56 with essential hypertension, 18 with hypertension accompanied by renal dysfunction), plasma renin activity and the plasma levels of angiotensin I and II were elevated.
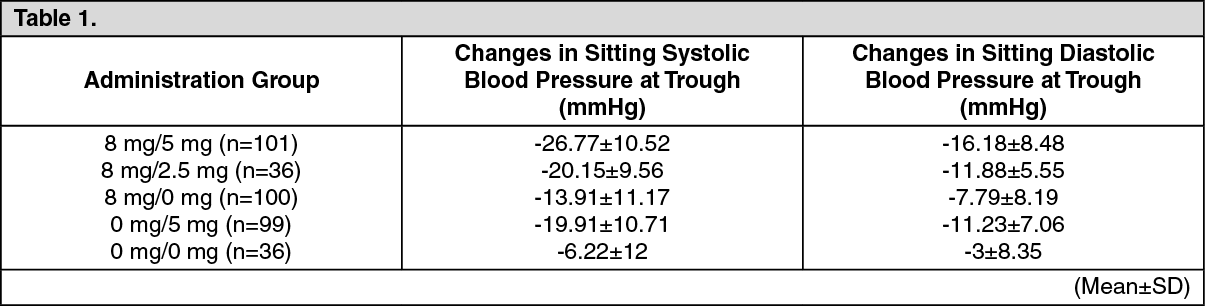
Clinical Studies: The result of double blind comparative study in patients with essential hypertension where a once daily dose of 8 mg/5 mg, 8 mg/2.5 mg, 8 mg/0 mg, or 0 mg/5 mg of candesartan cilexetil/amlodipine was administered for 12 weeks is as follows.
Significant differences in sitting diastolic blood pressure at trough and sitting systolic blood pressure at trough were observed in 8 mg/5 mg group compared to both 8 mg/0 mg and 0 mg/5 mg groups and in 8 mg/2.5 mg group compared to 8 mg/0 mg group (see Table 1).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In the long-term study (52 weeks) of concomitant use of candesartan cilexetil and amlodipine besilate, hypotensive effect persisted, the effect did not decrease, and stable control of blood pressure was obtained.
Once daily without setting the administration timing, before or after meals (see Pharmacokinetics).
Pharmacokinetics: Blood Concentration: After a single oral administration of a candesartan cilexetil/amlodipine 8 mg/5 mg combination tablet to healthy adults, active metabolite candesartan and inactive metabolite M-II and unchanged amlodipine were detected in the blood, but the unchanged candesartan cilexetil was undetected. Changes of blood concentrations of active metabolite candesartan and amlodipine are as indicated in Figures 1 and 2 and in Table 2. (See Figures 1 and 2, Table 2.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Effect of Meals: When a candesartan cilexetil/amlodipine 8 mg/5 mg combination tablet was administered to 12 healthy adults after meal, the C
max of active metabolite candesartan were about 2.1 times higher (under fasting: 78.9 ng/mL, after meal: 160.0 ng/mL) and the C
max of active metabolite candesartan were about 1.2 times higher (under fasting: 1,171.1 ng·hr/mL, after meal: 1,286.7 ng·hr/mL) than those under fasting conditions. No changes were observed in the C
max and AUC of amlodipine.
Bioequivalence: When the administration of a candesartan cilexetil/amlodipine 8 mg/5 mg combination tablet to healthy adults was compared with the concomitant use of each components, the bioequivalency of each components was confirmed both under fasting conditions or after meals. C
max and AUC of each component under fasting conditions or after meals are as indicated in Tables 3 and 4. (See Tables 3 and 4.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Urinary Excretion: After a single oral administration of a candesartan cilexetil/amlodipine 8 mg/5 mg combination tablet to 12 healthy adults, unchanged candesartan cilexetil was not detected in the urine, but the active metabolite candesartan, inactive metabolite M-II and unchanged amlodipine were excreted in the urine. The 48-hr cumulative excretion rates in the urine were 11.9% for candesartan and M-II combined, and 4.8% for unchanged amlodipine.
Metabolism: Candesartan cilexetil is metabolized to an active metabolite candesartan by carboxylesterase, and a part of it is further metabolized to inactive metabolite M-II by CYP2C9. However, compared with the blood concentration and urinary excretion of candesartan, those of M-II after administration of this drug to patients with essential hypertension are lower, indicating that the influence of genetic polymorphism of CYP2C9 on the blood concentration of candesartan is negligible.
Candesartan does not inhibit the metabolic activity of CYP1A1, 1A2, 2A6, 2B6, 2C8, 2C9-Arg, 2C19, 2D6, 2E1 and 3A4 (
in vitro).
Amlodipine is mainly metabolized by CYP3A4, and unchanged component as well as 9 metabolites are detected in the urine.
Population Pharmacokinetics (PPK) Analysis Using Blood Candesartan Concentration Levels: 2,886 time point samples of blood candesartan concentration obtained from total of 224 cases - 168 healthy male adults, 30 patients with essential hypertension and elderly essential hypertension, 18 hypertensive patients with renal dysfunction and 8 hypertensive patients with hepatic dysfunction were used to study relationship between sex/age/bodyweight/hepatic function parameter [AST (GOT), ALT (GPT)]/renal function parameter (serum creatinine, BUN)/blood albumin level/existence of hypertension and candesartan clearance/distribution volume/relative bioavailability. It is suggested that clearance in patients with hepatic dysfunction [AST (GOT) >40 or ALT (GPT) >35] decreases by 45%.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image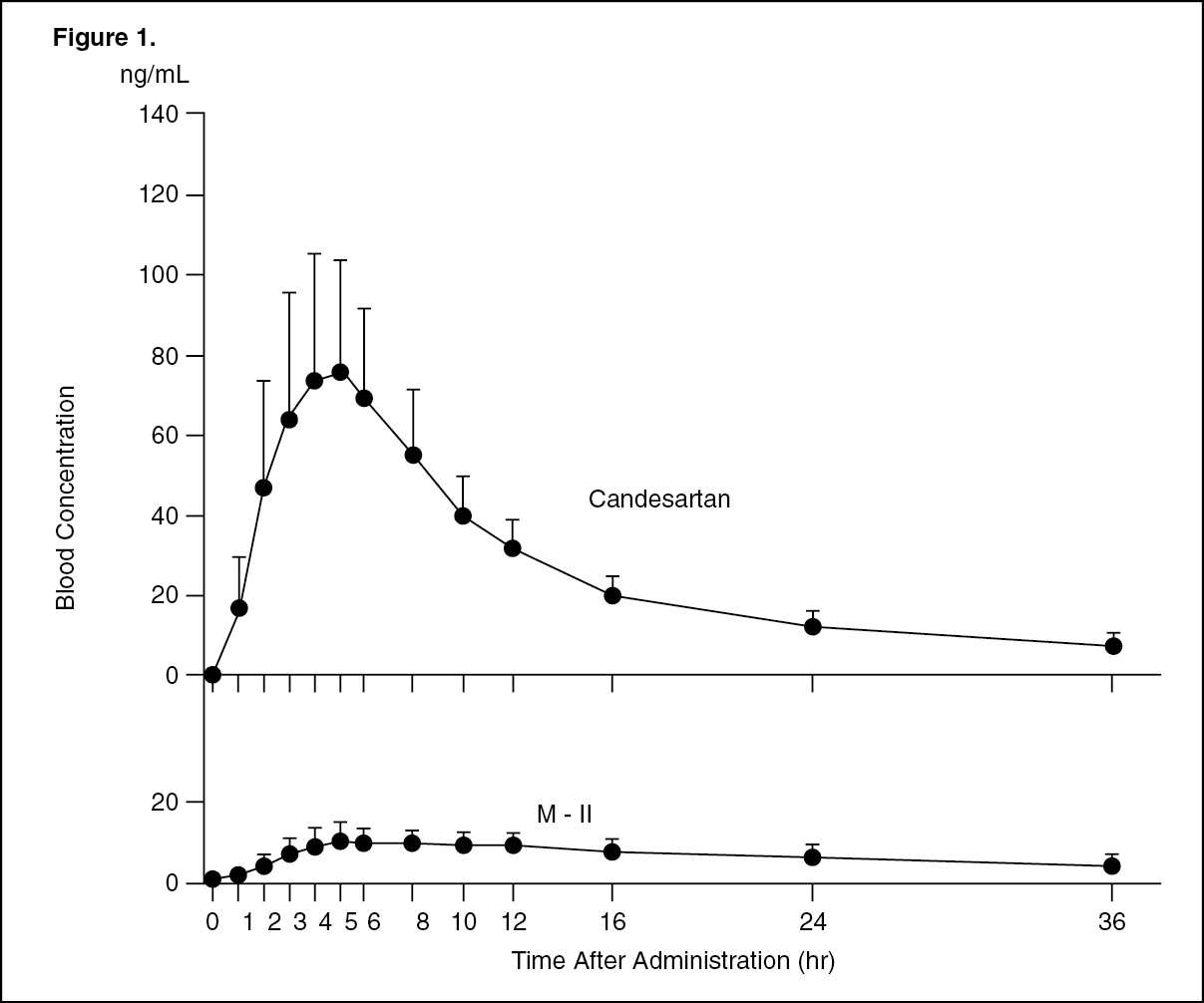 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image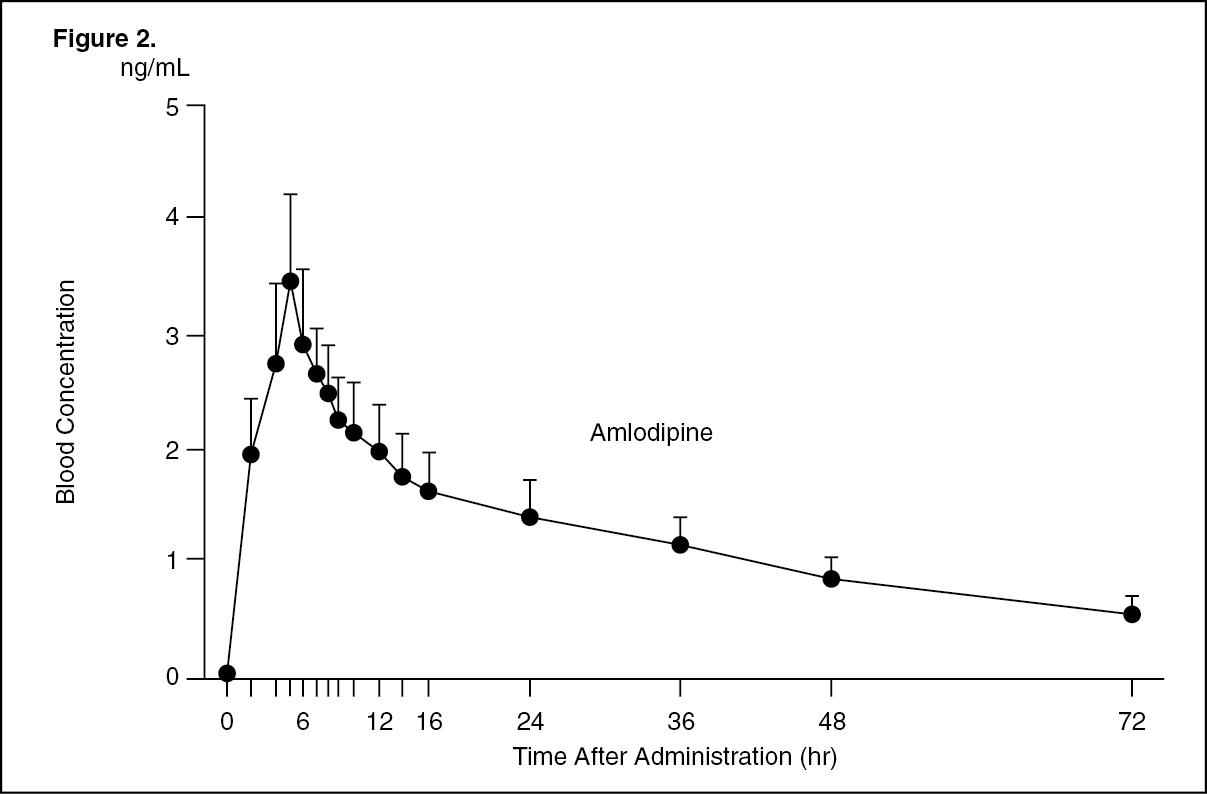 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
