Each film-coated tablet contains 80 mg of febuxostat.
Excipients/Inactive Ingredients: Each film-coated tablet contains 220 mg of lactose (as monohydrate).
Tablet core: Lactose monohydrate, Microcrystalline cellulose, Croscarmellose sodium, Colloidal silicon dioxide, Hydroxypropyl cellulose, Talcum and Magnesium stearate.
Tablet coating: Opadry II, 85F58789, white containing: Polyvinyl alcohol, Polyethylene glycol/Macrogol, Titanium dioxide and Talc, Yellow iron oxide and Simethicone emulsion.
Pharmacology: Pharmacodynamics: Febuxostat is a xanthine oxidase inhibitor, which is selective for xanthine oxidase, the enzyme that catalyzes the conversion of hypoxanthine to xanthine and xanthine to uric acid. By blocking uric acid production, febuxostat decreases serum concentration of uric acid. Febuxostat has no effect on other enzymes involved in purine and pyrimidine synthesis and metabolism, namely guanine deaminase, hypoxanthine-guanine phosphoribosyltransferase, purine nucleoside phosphorylase, orotate phosphoribosyltransferase and orotidine-5 V-monophosphate decarboxylase.
Pharmacokinetics: Absorption: Febuxostat is well (about 85%) and rapidly absorbed after oral doses which time of peak plasma concentration (tmax) is 1.5 hours. Cmax increases proportionally with dose within the dose range of 10-240 mg. The absolute availability of febuxostat has not been directly determined. Although dosage with a high-fat meal decreases peak plasma concentration, this is not thought clinically significant, and febuxostat may be taken with or without food.
Distribution: Febuxostat is highly bound (98-99%) to plasma proteins, mainly to albumin and has a low to moderate Vss/F (steady state volume of distribution) of 48 ± 23 L.
Metabolism: Febuxostat is metabolized directly by glucuronidation (up to 40%) mainly via uridine diphosphate-glucuronosyltransferase (UGT), namely UGT1A1, UGT1A8, UGT1A9 forming the febuxostat-acyl glucuronide. About 35% of febuxostat is metabolised by oxidation via cytochrome P450, including CYP1A1, CYP1A2, CYP2C8 and CYP2C9.
Elimination: Febuxostat is excreted in urine and faeces. Approximately 49% of the total drug is recovered in the urine. About 30% of the dose excreted in urine is the glucuronide, being the parent drug about 3% and approximately 12% is excreted as oxidative metabolites. Besides excreted in urine, about 45% of dose is recovered in faeces. Approximately 25% of the dose is excreted in faeces as the oxidised metabolites and about 12% as unchanged febuxostat.
Treatment of chronic hyperuricaemia in conditions where urate deposition has already occurred (including a history, or presence of, tophus and/or gouty arthritis).
Prevention and treatment of hyperuricaemia in adult patients undergoing chemotherapy for haematologic malignancies at intermediate to high risk of tumour lysis syndrome (TLS).
This drug is indicated in adults.
Recommended Dose: Gout: The recommended oral dose is 80 mg once daily without regard to food. If serum uric acid is >6 mg/dL after 2-4 weeks, increasing dose to 120 mg once daily may be considered.
Tumour Lysis Syndrome: The recommended oral dose is 120 mg once daily without regard to food. The administration should be started 2 days before the beginning of cytotoxic therapy and continued for 7-9 days according to chemotherapy duration as per clinical judgment.
Elderly: No dose adjustment is required in the elderly.
Paediatric population: The safety and the efficacy of this drug in children aged below the age of 18 years have not been established.
Renal impairment: Dosage adjustment is not needed in patients with mild to moderate renal impairment (creatinine clearance of 30-89 mL/minute) and in patients with severe renal impairment (creatinine clearance of 15-29 mL/minute), the maximum recommended dosage is 40 mg once daily.
Hepatic impairment: Dosage adjustment is not needed in patients with mild to moderate hepatic impairment (Child-Pugh class A or B) and the efficacy and safety of this drug has not been studied in patients with severe hepatic impairment (Child Pugh class C).
Mode of Administration: Administered orally without regard to meals or antacids.
No dose-limiting toxicities were reported following administration of doses up to 300 mg/day for 7 days. Symptomatic and supportive treatment should be initiated in patients with overdosage.
Do not use this drug concomitantly with azathioprine or mercaptopurine.
Do not use in patients with hypersensitivity to febuxostat or to any of the excipients.
Acute gout: An increased frequency of acute gout attacks (gout flare) may occur after initiation of febuxostat due to increased mobilization of urate from tissue deposits in response to reduction in serum uric acid concentrations, resulted in an increased frequency of acute gout attacks after initiation of febuxostat. For gout flare prophylaxis, NSAIDs or colchicine should be considered; these agents may be started when febuxostat therapy is initiated for up to 6 months. If a gout flare occurs during febuxostat administration, febuxostat may be continued, and the gout flare managed as appropriate.
Cardiovascular events: Treatment of febuxostat in patients with ischaemic heart disease or congestive heart failure is not recommended. Due to studies, a higher rate of cardiovascular thromboembolic events (cardiovascular deaths, nonfatal myocardial infarction, nonfatal stroke) was reported in patients receiving febuxostat than in patients receiving allopurinol. Patients receiving febuxostat should be monitored for signs and symptoms of myocardial infarction and stroke.
However, the study of long-term cardiovascular safety of febuxostat compared with allopurinol in patients with gout found that febuxostat is non-inferior to allopurinol therapy with respect to the primary cardiovascular endpoint which was a composite of hospitalization for non-fatal myocardial infarction or biomarker-positive acute coronary syndrome; non-fatal stroke; or cardiovascular death and its long-term use is not associated with an increased risk of death or serious adverse events compared with allopurinol.
Treatment in patients receiving chemotherapy for haematologic malignancies at intermediate to high risk of tumour lysis syndrome may require cardiac monitoring.
Hepatic effects: Serum aminotransferase (i.e., AST, ALT) concentrations exceeding 3 times the upper limit of normal (ULN) and hepatic failure have been reported in patients receiving febuxostat.
Liver function test (serum ALT, AST, alkaline phosphatase, and total bilirubin concentrations) should be performed prior to initiation of febuxostat therapy and repeated promptly in patients with manifestations suggestive of liver damage, such as fatigue, anorexia, right upper abdominal discomfort, dark-colored urine, or jaundice. If aminotransferase concentrations are elevated (ALT exceeding 3 times the ULN), febuxostat therapy should be interrupted and the cause of the abnormalities investigated. If an alternate etiology is not found, febuxostat therapy should not be restarted.
Dermatologic and hypersensitivity reactions: Serious dermatologic and hypersensitivity reactions (including Stevens-Johnson syndrome, erythema multiforme, toxic epidermal necrolysis, and drug reaction with eosinophilia and systemic symptoms (DRESS)), and hypersensitivity reactions have been reported in patients receiving febuxostat. Febuxostat should be used with caution in patients with history of dermatologic reactions to allopurinol.
Febuxostat should be discontinued if serious dermatologic reactions (e.g., rash; peeling or blistering of the skin; swelling or blistering of the lips, eyes, or mouth) are suspected.
Thyroid disorders: An increase in thyroid-stimulating hormone (TSH) concentrations (>5.5 µIU/mL) with treatment with febuxostat (5.5%) was reported. About 8% and 4% of subjects treated with febuxostat and allopurinol, respectively, showed raised TSH levels with no effect on free T4 and, consequently, this side effect may not be of any clinical relevance.
Pregnancy: Data are inadequate regarding use of febuxostat in pregnant women. Animal reproduction studies using febuxostat have not revealed evidence of fetal harm at exposure greater than those attained with maximum recommended human dosage.
Lactation: Febuxostat is distributed into milk in rats at concentrations up to approximately 7 times plasma concentrations of the drug. It is not known whether febuxostat distributes into human milk, affects the breast-fed infant, or affects milk production.
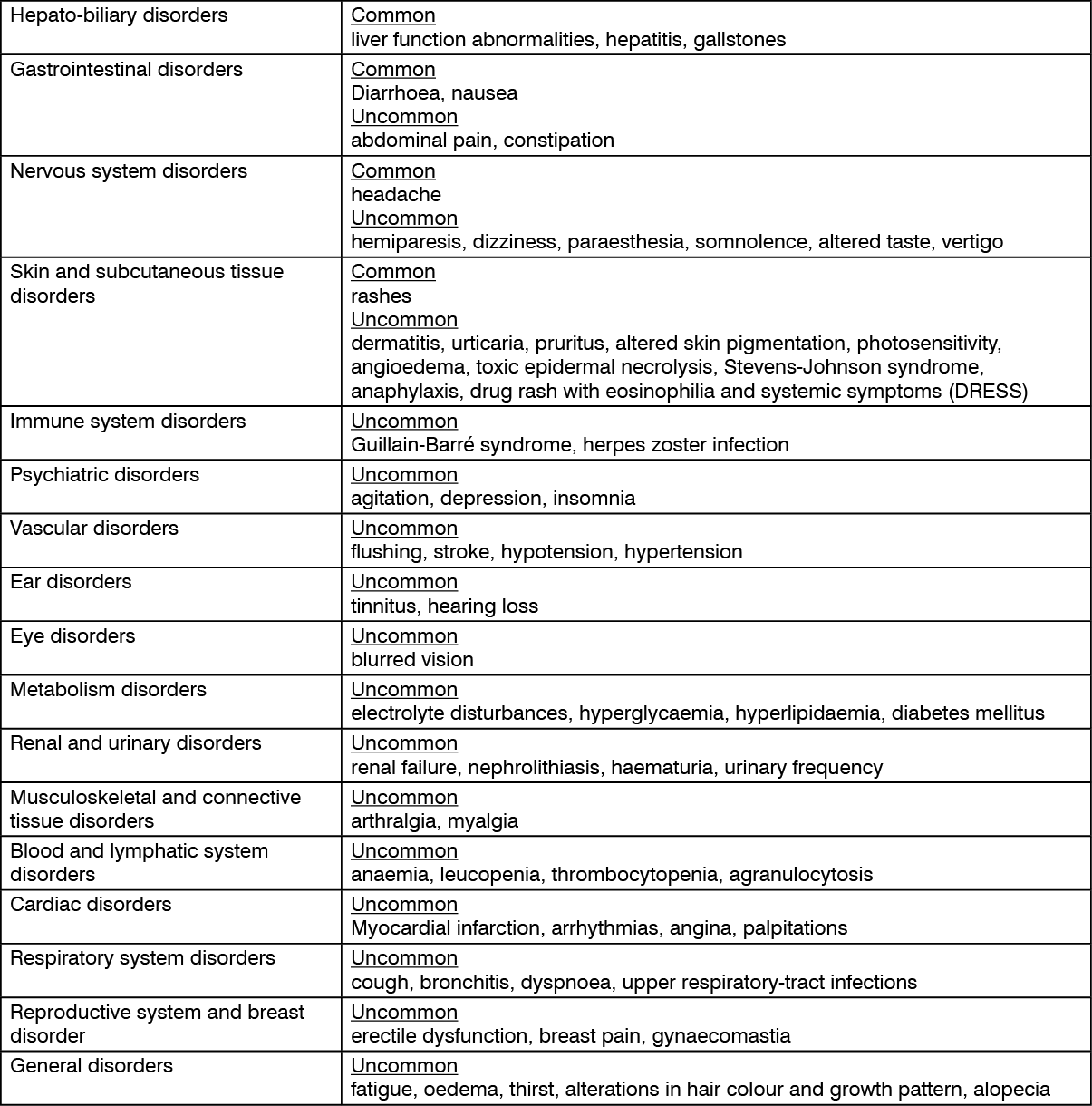
See table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Drugs affecting hepatic microsomal or other enzymes: Drug interactions generally are not expected between febuxostat and inhibitors or inducers of particular enzyme isoforms.
Drugs metabolized by hepatic microsomal enzymes: Febuxostat does not inhibit CYP1A2, CYP2C9, CYP2C19, or CYP3A4, but is a weak inhibitor of CYP2D6. Febuxostat does not induce CYP1A2, CYP2B6, CYP2C9, CYP2C19, CYP3A4. Pharmacokinetic interactions are unlikely between febuxostat and substrates of these isoenzymes.
Despiramine: Effects of febuxostat on desipramine pharmacokinetics are not considered clinically important; dosage adjustment is not expected to be necessary.
Drugs metabolized by xanthine oxidase: Febuxostat is a xanthine oxidase inhibitor and may increase plasma concentrations of drugs metabolized by xanthine oxidase, resulting in toxicity.
Azathioprine and Mercaptopurine: Concomitant use of febuxostat with azathioprine and mercaptopurine is contraindicated since increased plasma concentrations of azathioprine and mercaptopurine have been reported when these drugs were administered concomitantly with allopurinol, another xanthine oxidase inhibitor. Drug interaction studies between febuxostat and azathioprine or mercaptopurine are not available.
Theophylline: Following concomitant administration of febuxostat (80 mg once daily) and theophylline in healthy individuals, peak plasma concentrations were not altered, thus theophylline dosage adjustments are not necessary when febuxostat and theophylline are used concomitantly.
Antacid: Pharmacokinetic interaction is unlikely.
Antineoplastic agents: Studies data are not available regarding safety of febuxostat in patients receiving antineoplastic agents.
Colchicine: Clinically important pharmacokinetic interaction is unlikely; dosage adjustment is not needed.
Hydrochlorothiazide: Clinically important pharmacokinetic interaction is unlikely; dosage adjustment is not needed.
Nonsteroidal Anti-inflammatory Agents (NSAIDs): Indomethacin: Clinically important pharmacokinetic interaction is unlikely; dosage adjustment is not needed.
Naproxen: Clinically important pharmacokinetic interaction is unlikely; dosage adjustment is not needed.
Warfarin: Pharmacokinetic interaction is unlikely; dosage adjustment is not needed.
M04AA03 - febuxostat ; Belongs to the class of preparations inhibiting uric acid production. Used in the treatment of gout.
Uxoric FC tab 80 mg
10 × 10's



 Sign Out
Sign Out