


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Rosuvastatin is a selective and competitive inhibitor of HMG-CoA reductase, the rate-limiting enzyme that converts 3-hydroxy-3-methylglutaryl coenzyme A to mevalonate, a precursor for cholesterol. The primary site of action of rosuvastatin is the liver, the target organ for cholesterol lowering.
Rosuvastatin increases the number of hepatic LDL receptors on the cell-surface, enhancing uptake and catabolism of LDL and it inhibits the hepatic synthesis of VLDL, thereby reducing the total number of VLDL and LDL particles.
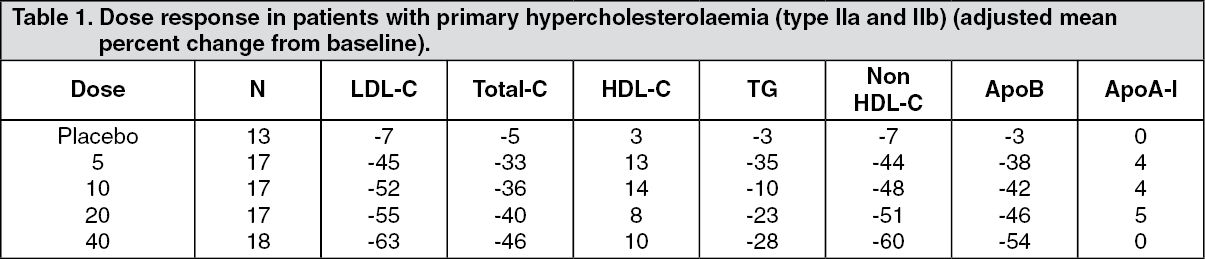
Pharmacodynamic effects: VIVACOR reduces elevated LDL-cholesterol, total cholesterol and triglycerides and increases HDL-cholesterol. It also lowers ApoB, nonHDL-C, VLDL-C, VLDL-TG and increases ApoA-I (see Table 1). VIVACOR also lowers the LDL-C/HDL-C, total C/HDL-C and non-HDL-C/HDL-C and the ApoB/ApoA-I ratios. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageA therapeutic effect is obtained within 1 week following treatment initiation and 90% of maximum response is achieved in 2 weeks. The maximum response is usually achieved by 4 weeks and is maintained after that.
Clinical efficacy: VIVACOR is effective in adults with hypercholesterolaemia, with and without hypertriglyceridaemia, regardless of race, sex, or age and in special populations such as diabetics, or patients with familial hypercholesterolaemia.
From pooled phase III data, VIVACOR has been shown to be effective at treating the majority of patients with type IIa and IIb hypercholesterolaemia (mean baseline LDL-C about 4.8 mmol/l) to recognised European Atherosclerosis Society (EAS; 1998) guideline targets; about 80% of patients treated with 10 mg reached the EAS targets for LDL-C levels (<3 mmol/l).
In a large study, 435 patients with heterozygous familial hypercholesterolaemia were given VIVACOR from 20 mg to 80 mg in a force-titration design. All doses showed a beneficial effect on lipid parameters and treatment to target goals. Following titration to a daily dose of 40 mg (12 weeks of treatment), LDL-C was reduced by 53%. 33% of patients reached EAS guidelines for LDL-C levels (<3 mmol/l).
In a force-titration, open label trial, 42 patients with homozygous familial hypercholesterolaemia were evaluated for their response to VIVACOR 20-40 mg. In the overall population, the mean LDL-C reduction was 22%.
In the METEOR study, the effect of rosuvastatin 40 mg on the progression of atherosclerosis was assessed by B-mode ultrasound of the carotid arteries. In this multi-center, double blind, placebo-controlled clinical trial, 984 subjects at low risk for coronary heart disease (defined as Framingham risk <10% over ten years) and with a mean LDL-C of 154.5 mg/dL but with subclinical atherosclerosis as detected by CIMT (Carotid Intima Media Thickness) were randomized in a 5:2 ratio to treatment with either rosuvastatin 40 mg or placebo for 2 years. Rosuvastatin significantly slowed the progression of carotid atherosclerosis compared to placebo. The difference in the rate of change in the maximum CIMT of all 12 carotid artery sites between rosuvastatin-treated patients and placebo-treated patients was -0.0145 mm/year (95% CI -0.0196, -0.0093; p<0.0001). The change from baseline for the rosuvastatin group was -0.0014 mm/year (95% CI -0.0041, 0.0014), but was not significantly different from zero (p=0.3224). The beneficial effects of rosuvastatin were consistent across all 4 secondary CIMT endpoints. There was significant progression in the placebo group (+0.0131 mm/year; 95% CI 0.0087, 0.0174; p<0.0001). In the rosuvastatin group, 52.1% of patients demonstrated an absence of disease progression (i.e. regressed) compared to 37.7% of patients in the placebo group (p=0.0002). Rosuvastatin 40 mg was well-tolerated and the data were consistent to the established safety profile for rosuvastatin.
In clinical studies with a limited number of patients, VIVACOR has been shown to have additive efficacy in lowering triglycerides when used in combination with fenofibrate and in increasing HDL-C levels when used in combination with niacin (see Precautions).
Rosuvastatin has not been proven to prevent the associated complications of lipid abnormalities, such as coronary heart disease as mortality and morbidity studies with VIVACOR have not yet been completed.
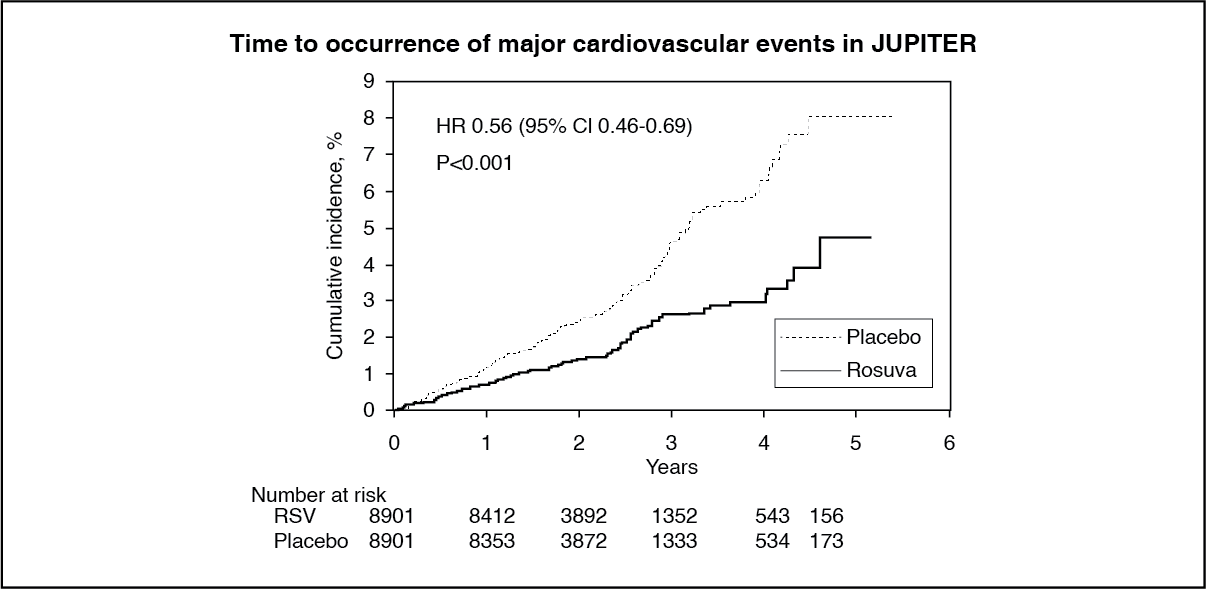
In the Justification for the Use of Statins in Primary Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER) study, the effect of VIVACOR (rosuvastatin calcium) on the occurrence of major atherosclerotic cardiovascular (CV) disease events was assessed in 17,802 men (≥50 years) and women (≥60 years) who had no established cardiovascular disease, LDL-C levels <130 mg/dL (3.3 mmol/l) and hs-CRP levels ≥2 mg/L. The study population had an estimated baseline coronary heart disease risk of 11.3% over 10 years based on the Framingham risk criteria and included a high percentage of patients with additional risk factors such as hypertension (58%), low HDL-C levels (23%), cigarette smoking (16%) or a family history of premature CHD (12%). Study participants were randomly assigned to placebo (n=8,901) or rosuvastatin 20 mg once daily (n=8,901) and were followed for a mean duration of 2 years.
The primary endpoint was a composite endpoint consisting of the time-to-first occurrence of any of the following CV events: CV death, non-fatal myocardial infarction, non-fatal stroke, unstable angina or an arterial revascularization procedure.
Rosuvastatin significantly reduced the risk of CV events (252 events in the placebo group vs. 142 events in the rosuvastatin group) with a statistically significant (p<0.001) relative risk reduction of 44% (see figure). The benefit was apparent within the first 6 months of treatment. The risk reduction was consistent across multiple predefined population subsets based on assessments of age, sex, race, smoking status, family history of premature CHD, body mass index, LDL-C, HDL-C or hsCRP levels at the time of entry into the study. There was a statistically significant 48% reduction in the combined endpoint of CV death, stroke and myocardial infarction (HR: 0.52, 95% CI: 0.40-0.68, p<0.001), a 54% reduction in fatal or nonfatal myocardial infarction (HR: 0.46, 95% CI: 0.30-0.70) and a 48% reduction in fatal or nonfatal stroke. Total mortality was reduced 20% in the rosuvastatin group (HR: 0.80, 95% CI: 0.67-0.97, p=0.02). (See figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe safety profile for subjects taking rosuvastatin 20 mg was generally similar to that of subjects taking placebo. There were 1.6% of rosuvastatin and 1.8% of placebo subjects who withdrew from the trial due to an adverse event, irrespective of treatment causality. The most common adverse reactions that led to treatment discontinuation were: myalgia (0.3% rosuvastatin, 0.2% placebo), abdominal pain (0.03% rosuvastatin, 0.02% placebo) and rash (0.03% rosuvastatin, 0.03% placebo). Adverse reactions reported in ≥2% of patients and at a rate greater than or equal to placebo were myalgia (7.6% rosuvastatin, 6.6% placebo), constipation (3.3% rosuvastatin, 3.0% placebo) and nausea (2.4% rosuvastatin, placebo 2.3%).
In JUPITER, there was a statistically significant increase in the frequency of diabetes mellitus reported by investigators; 2.8% of patients in the rosuvastatin group and 2.3% of patients in the placebo group (HR: 1.27, 95% CI: 1.05-1.53, p=0.015). The difference between treatment groups (rosuvastatin versus placebo) in mean HbA1c change from baseline was approximately 0.1%. A post hoc analysis of this study suggests that the risk of development of diabetes on rosuvastatin therapy is limited to patients already at high risk of developing diabetes. The cardiovascular and mortality benefits of rosuvastatin therapy exceeded the diabetes hazard in the trial population as a whole as well as in participants at increased risk of developing diabetes (see Precautions and Adverse Reactions).
Children and Adolescents with Hypercholesterolaemia: In a double blind, randomized, multi-centre, placebo-controlled, 12-week study (n=176, 97 male and 79 female) followed by a 40-week (n=173, 96 male and 77 female), open label, rosuvastatin dose titration phase, 10-17 years of age (Tanner stage II-V, females at least 1 year post-menarche) with heterozygous familial hypercholesterolaemia received rosuvastatin 5, 10 or 20 mg or placebo daily for 12 weeks and then all received rosuvastatin daily for 40 weeks. At study entry, approximately 30% of the patients were 10-13 years and approximately 17%, 18%, 40%, and 25% were Tanner stage II, III, IV, and V respectively.
Rosuvastatin reduced LDL-C (primary endpoint), total cholesterol and ApoB levels. Results are shown in Table 2 as follows. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAt the end of the 40 week, open label, titration to goal, dosing up to a maximum of 20 mg once daily, 70 of 173 patients (40.5%) had achieved the LDL-C goal of less than 110 mg/dL (2.8 mmol/L).
After 52 weeks of study treatment, no effect on growth or sexual maturation was detected (see Precautions).
Rosuvastatin was also studied in a 2-year open-label, titration-to-goal study in 198 children with heterozygous familial hypercholesterolaemia aged 6 to 17 years (88 male and 110 female, Tanner stage <II-V). The starting dose for all patients was 5 mg rosuvastatin once daily. Patients aged 6 to 9 years (n=64) could titrate to a maximum dose of 10 mg once daily and patients aged 10 to 17 years (n=134) to a maximum dose of 20 mg once daily.
After treatment, 74 of 197 patients (37.6%) in this study achieved the LDL-C goal of less than 110 mg/dL (2.8 mmol/L). All age groups showed statistically significant reductions in LDL-C from baseline values.
Rosuvastatin 5 mg, 10 mg, and 20 mg also achieved statistically significant mean changes from baseline for the following secondary lipid and lipoprotein variables: HDL-C, TC, non-HDL-C, LDL-C/HDL-C, TC/HDL-C, TG/HDL-C, non-HDL-C/HDL-C, ApoB, ApoB/ApoA-1. These changes were each in the direction of improved lipid responses and were sustained over 2 years.
No effect on growth or sexual maturation was detected after 24 months of treatment.
Pharmacokinetics: Absorption: Maximum rosuvastatin plasma concentrations are achieved approximately 5 hours after oral administration. The absolute bioavailability is approximately 20%.
Distribution: Rosuvastatin is taken up extensively by the liver which is the primary site of cholesterol synthesis and LDL-C clearance. The volume of distribution of rosuvastatin is approximately 134 L. Approximately 90% of rosuvastatin is bound to plasma proteins, mainly to albumin.
Metabolism: Rosuvastatin undergoes limited metabolism (approximately 10%). In vitro metabolism studies using human hepatocytes indicate that rosuvastatin is a poor substrate for cytochrome P450-based metabolism. CYP2C9 was the principal isoenzyme involved, with 2C19, 3A4 and 2D6 involved to a lesser extent. The main metabolites identified are the N-desmethyl and lactone metabolites. The N-desmethyl metabolite is approximately 50% less active than rosuvastatin whereas the lactone form is considered clinically inactive. Rosuvastatin accounts for greater than 90% of the circulating HMG-CoA reductase inhibitor activity.
Excretion: Approximately 90% of the rosuvastatin dose is excreted unchanged in the faeces (consisting of absorbed and non-absorbed active substance) and the remaining part is excreted in urine. Approximately 5% is excreted unchanged in urine. The plasma elimination half-life is approximately 19 hours. The elimination half-life does not increase at higher doses. The geometric mean plasma clearance is approximately 50 litres/hour (coefficient of variation 21.7%). As with other HMG-CoA reductase inhibitors, the hepatic uptake of rosuvastatin involves the membrane transporter OATP-C. This transporter is important in the hepatic elimination of rosuvastatin.
Linearity: Systemic exposure of rosuvastatin increases in proportion to dose. There are no changes in pharmacokinetic parameters following multiple daily doses.
Special populations: Age and sex: There was no clinically relevant effect of age or sex on the pharmacokinetics of rosuvastatin in adults. The exposure in children and adolescents with heterozygous familial hypercholesterolaemia appears to be similar to or lower than that in adult patients with dyslipidemia.
Race: Pharmacokinetic studies show an approximate 2-fold elevation in median AUC and Cmax in Asian subjects compared with Caucasians. A population pharmacokinetic analysis revealed no clinically relevant differences in pharmacokinetics among Caucasian, Hispanic and Black or Afro-Caribbean groups.
Renal insufficiency: In a study in subjects with varying degrees of renal impairment, mild to moderate renal disease had no influence on plasma concentration of rosuvastatin or the N-desmethyl metabolite. Subjects with severe impairment (CrCl <30 ml/min) had a 3-fold increase in plasma concentration and a 9-fold increase in the N-desmethyl metabolite concentration compared to healthy volunteers. Steady-state plasma concentrations of rosuvastatin in subjects undergoing haemodialysis were approximately 50% greater compared to healthy volunteers.
Hepatic insufficiency: In a study with subjects with varying degrees of hepatic impairment there was no evidence of increased exposure to rosuvastatin in subjects with Child-Pugh scores of 7 or below. However, two subjects with Child-Pugh scores of 8 and 9 showed an increase in systemic exposure of at least 2-fold compared to subjects with lower Child-Pugh scores. There is no experience in subjects with Child-Pugh scores above 9.
Genetic polymorphisms: Disposition of HMG-CoA reductase inhibitors, including rosuvastatin, involves OATP1B1 and BCRP transporter proteins. In patients with SLCO1B1 (OATP1B1) and/or ABCG2 (BCRP) genetic polymorphisms there is a risk of increased rosuvastatin exposure. Individual polymorphisms of SLCO1B1 c.521CC and ABCG2 c.421AA are associated with an approximate 1.6-fold higher rosuvastatin exposure (AUC) or 2.4-fold higher exposure, respectively, compared to the SLCO1B1 c.521TT or ABCG2 c.421CC genotypes.
Toxicology: Preclinical safety data: Preclinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity and carcinogenicity potential. In a rat pre- and postnatal study, reproductive toxicity was evident from reduced litter sizes, litter weight and pup survival. These effects were observed at maternotoxic doses at systemic exposures several times above the therapeutic exposure level.