The information highlighted (if any) are the most recent updates for this brand.
1 film-coated tablet contains 10 mg, 15 mg and 20 mg rivaroxaban, respectively.
Excipients/Inactive Ingredients: Microcrystalline cellulose, Croscarmellose sodium, Hypromellose 5 cP, Lactose monohydrate, Magnesium stearate, sodium lauryl sulfate.
Film-coating: Ferric oxide red, Hypromellose 15 cP, Macrogol 3350, Titanium dioxide.
Pharmacotherapeutic group: Direct factor Xa inhibitors. ATC Code: B01AF01.
Rivaroxaban is a highly selective direct factor Xa inhibitor with oral bioavailability.
PHARMACOLOGY: Pharmacodynamics: SPAF: Patients who undergo PCI with stent placement: A randomized, open-label, multicenter study (PIONEER AF-PCI) was conducted in 2124 patients with non-valvular atrial fibrillation who underwent PCI with stent placement for primary atherosclerotic disease to compare safety of two rivaroxaban regimens and one VKA regimen. Patients were randomly assigned in a 1:1:1 fashion for an overall 12 month-therapy.
Group 1 received rivaroxaban 15 mg once daily (10 mg once daily in patients with CrCl: 30 to <50 mL/min) plus P2Y12 inhibitor. Group 2 received rivaroxaban 2.5 mg twice daily plus DAPT (dual antiplatelet therapy i.e. clopidogrel 75 mg [or alternate P2Y12 inhibitor] plus low-dose acetylsalicylic acid [ASA]) for 1, 6 or 12 months followed by rivaroxaban 15 mg (or 10 mg for subjects with CrCl: 30 to <50 mL/min) once daily plus low-dose ASA. Group 3 received dose-adjusted VKA plus DAPT for 1, 6 or 12 months followed by dose-adjusted VKA plus low-dose ASA.
The primary safety endpoint, clinically significant bleeding events, occurred in 109 (15.7%), 117 (16.6%), and 167 (24.0%) subjects in group 1, group 2, and group 3, respectively (HR 0.59; 95% CI 0.47-0.76; p<0.001, and HR 0.63; 95% CI 0.50-0.80; p<0.001, respectively). The secondary endpoint (composite of cardiovascular events CV death, MI, or stroke) occurred in 41 (5.9%), 36 (5.1%), and 36 (5.2%) subjects in the group 1, group 2, and group 3 respectively. Each of the rivaroxaban regimens showed a significant reduction in clinically significant bleeding events compared to the VKA regimen in patients with non-valvular atrial fibrillation who underwent a PCI with stent placement.
Treatment and prevention of recurrent DVT and PE: Clinical efficacy and safety: The Xarelto clinical program was designed to demonstrate the efficacy of Xarelto in the initial and continued treatment of acute DVT and PE and prevention of recurrent DVT and PE. Over 12,800 patients were studied in four randomized controlled phase III clinical studies (EINSTEIN DVT, EINSTEIN PE, EINSTEIN Extension and EINSTEIN CHOICE) and additionally a predefined analysis of the pooled Einstein DVT and Einstein PE studies was conducted (see Table 3). The overall combined treatment duration in all studies was up to 21 months.
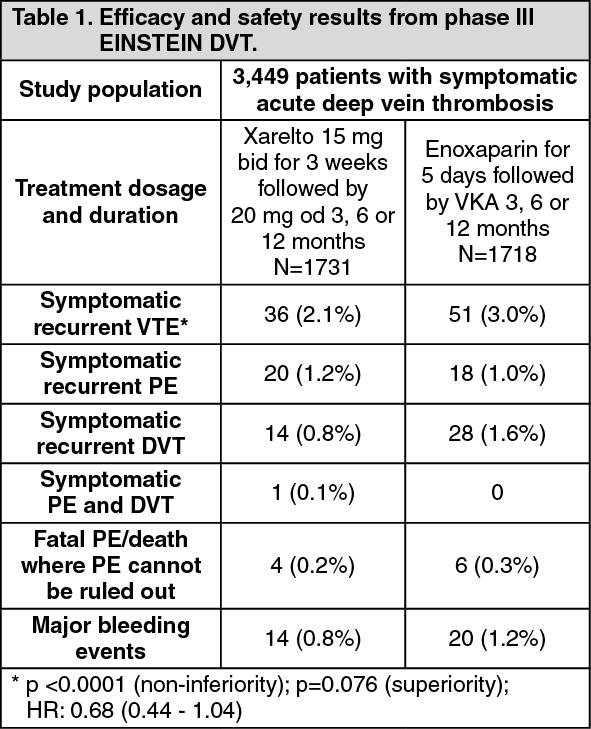
In EINSTEIN DVT, 3,449 patients with acute DVT were studied for the treatment of DVT and the prevention of recurrent DVT and PE. The treatment duration was up to 12 months depending on the clinical judgment of the investigator. For the initial 3 week treatment of acute DVT 15 mg of Xarelto was administered twice daily. This was followed by 20 mg of Xarelto once daily.
In EINSTEIN PE, 4,832 patients with acute PE were studied for the treatment of PE and the prevention of recurrent DVT and PE. The treatment duration was up to 12 months depending on the clinical judgement of the investigator. For the initial treatment of acute PE 15 mg rivaroxaban was administered twice daily for three weeks. This was followed by 20 mg rivaroxaban once daily.
In both the EINSTEIN DVT and the Einstein PE study, the comparator treatment regimen consisted of enoxaparin administered for at least 5 days in combination with vitamin K antagonist treatment until the PT/INR was in therapeutic range (≥2.0). Treatment was continued with a vitamin K antagonist dose-adjusted to maintain the PT/INR values within the therapeutic range of 2.0 to 3.0.
In EINSTEIN Extension, 1,197 patients with DVT or PE were studied for the prevention of recurrent DVT and PE. The treatment duration was up to 12 months depending on the clinical judgment of the investigator. Xarelto 20 mg once daily was compared with placebo.
EINSTEIN DVT, PE and Extension used the same pre-defined primary and secondary efficacy outcomes. The primary efficacy outcome was symptomatic recurrent VTE defined as the composite of recurrent DVT or fatal or non-fatal PE. The secondary efficacy outcome was defined as the composite of recurrent DVT, non-fatal PE and all-cause mortality.
In EINSTEIN CHOICE, 3,396 patients with confirmed symptomatic DVT and/or PE who completed 6-12 months of anticoagulant treatment were studied for the prevention of fatal PE or non-fatal symptomatic recurrent DVT or PE. Patients with an indication for continued therapeutic-dosed anticoagulation were excluded from the study. The treatment duration was up to 12 months depending on the individual randomization date (median: 351 days). Xarelto 20 mg once daily and Xarelto 10 mg once daily were compared with 100 mg acetylsalicylic acid once daily.
The primary efficacy outcome was symptomatic recurrent VTE defined as the composite of recurrent DVT or fatal or non-fatal PE. The secondary efficacy outcome was the composite of the primary efficacy outcome, MI, ischemic stroke, or non-CNS systemic embolism.
In the EINSTEIN DVT study (see Table 1) Xarelto was demonstrated to be non-inferior to enoxaparin/VKA for the primary outcome. The prespecified NCB (primary efficacy outcome plus major bleeding events) was reported with a HR of 0.67 ((95% CI = 0.47-0.95), nominal p value p=0.027) in favour of rivaroxaban. The incidence rates for the principal safety outcome (major or clinically relevant non-major bleeding events) as well as the secondary safety outcome (major bleeding events), were similar for both treatment groups.
In the EINSTEIN PE study (see Table 2) Xarelto was demonstrated to be non-inferior to enoxaparin/VKA for the primary outcome (p=0.0026 (test for non-inferiority); hazard ratio: 1.12 (0.75 - 1.68)). The prespecified NCB (primary efficacy outcome plus major bleeding events) was reported with a HR of 0.85 ((95% CI= 0.63 - 1.14), nominal p value p=0.275).
A prespecified pooled analysis of the outcome of the EINSTEIN DVT and PE studies was conducted (see Table 3).
In the EINSTEIN Extension study (see Table 4 ) Xarelto was superior to placebo for the primary and secondary efficacy outcomes. For the principal safety outcome (major bleeding events) there was a non-significant numerically higher incidence rate for patients treated with Xarelto 20 mg once daily compared to placebo. The secondary safety outcome (major or clinically relevant non-major bleeding events) showed higher rates for patients treated with Xarelto 20 mg once daily compared to placebo.
In the EINSTEIN CHOICE study Xarelto 20 mg and 10 mg were both superior to 100 mg acetylsalicylic acid for the primary efficacy outcome. The secondary efficacy outcome was significantly reduced when comparing Xarelto 20 mg or 10 mg vs. 100 mg acetylsalicylic acid. The principal safety outcome (major bleeding events) was similar for patients treated with Xarelto 20 mg and 10 mg once daily compared to 100 mg acetylsalicylic acid. The secondary safety outcome (non-major bleeding associated with treatment cessation of more than 14 days) was similar when comparing Xarelto 20 mg or 10 mg vs. 100 mg acetylsalicylic acid. Outcomes were consistent across the patients with provoked and unprovoked VTE (see Table 5).
In a prespecified net clinical benefit analysis (NCB) (primary efficacy outcome plus major bleeding events) of EINSTEIN CHOICE, a HR of 0.44 (95% CI 0.27 - 0.71, p=0.0009) for Xarelto 20 mg once daily vs 100 mg acetylsalicylic acid once daily and a HR of 0.32 (95% CI 0.18 - 0.55, p<0.0001) for Xarelto 10 mg once daily vs 100 mg acetylsalicylic acid once daily were reported. (See Tables 1, 2, 3, 4 and 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In addition to the phase III EINSTEIN program, a prospective, non-interventional, open-label cohort study (XALIA) with central outcome adjudication including recurrent VTE, major bleeding and death has been conducted. 5,142 patients with acute DVT were enrolled to investigate the long-term safety of rivaroxaban compared with standard-of-care anticoagulation therapy under real-world conditions. Rates of major bleeding, recurrent VTE and all-cause mortality for rivaroxaban were 0.7%, 1.4% and 0.5%, respectively. Hazard ratios comparing rivaroxaban and standard-of-care were adjusted to account for differences in patient baseline characteristics. Adjusted hazard ratios for major bleeding, recurrent VTE and all-cause mortality were 0.77 (95% CI 0.40-1.50), 0.91 (95% CI 0.54-1.54) and 0.51 (95% CI 0.24-1.07), respectively.
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In addition to the phase III EINSTEIN program, a prospective, non-interventional, open-label cohort study (XALIA) with central outcome adjudication including recurrent VTE, major bleeding and death has been conducted. 5,142 patients with acute DVT were enrolled to investigate the long-term safety of rivaroxaban compared with standard-of-care anticoagulation therapy under real-world conditions. Rates of major bleeding, recurrent VTE and all-cause mortality for rivaroxaban were 0.7%, 1.4% and 0.5%, respectively. Hazard ratios comparing rivaroxaban and standard-of-care were adjusted to account for differences in patient baseline characteristics. Adjusted hazard ratios for major bleeding, recurrent VTE and all-cause mortality were 0.77 (95% CI 0.40-1.50), 0.91 (95% CI 0.54-1.54) and 0.51 (95% CI 0.24-1.07), respectively.
Rivaroxaban showed similar safety and efficacy compared to standard anticoagulation.
These results in patients who were observed in routine clinical practice are consistent with those observed in the EINSTEIN DVT study.
Patients with prosthetic heart valves having recently undergone TAVR: In the randomised, open label, active-controlled, event-driven multicenter phase III GALILEO study 1644 patients were randomized to either a rivaroxaban-based strategy or an antiplatelet-based strategy 1-7 days after a successful transcatheter aortic valve replacement. Patients with previous atrial fibrillation or with an ongoing indication for oral anticoagulation were excluded.
The main objective was to assess the efficacy and safety of a rivaroxaban-based treatment strategy (10 mg rivaroxaban od plus 75-100 mg acetylsalicylic acid (ASA) od for 90 days followed by rivaroxaban 10 mg od) compared to standard of care (clopidogrel 75 mg od plus 75-100 mg ASA od for 90 days followed by ASA od). The study was terminated early due to an imbalance in death and thromboembolic events.
In the intention-to-treat (ITT) analysis the primary efficacy endpoint, i.e. death and thromboembolic events, occurred in 105 patients (9.8 per 100 patient years) in the rivaroxaban arm and in 78 patients (7.21 per 100 patient years) in the antiplatelet arm; the HR was 1.35 (95% CI: 1.01; 1.81). In the on-treatment analysis the primary efficacy outcome occurred in 68 patients (8.11 per 100 patient years) in the rivaroxaban arm compared to 63 (6.6 per 100 patient years) in the antiplatelet arm; the HR was 1.21 (95% CI: 0.86; 1.70).
In the ITT analysis the primary safety endpoint, i.e. composite of life-threatening, disabling or major bleeding, occurred in 46 patients (4.29 per 100 patient years) in the rivaroxaban arm compared to 31 (2.83 per 100 patient years) in the antiplatelet arm; the HR was 1.50 (95% CI 0.95; 2.37).
Patients with high risk triple positive antiphospholipid syndrome: In an investigator sponsored randomized open-label multicenter study with blinded endpoint adjudication, rivaroxaban was compared to warfarin in patients with a history of thrombosis, diagnosed with antiphospholipid syndrome and at high risk for thromboembolic events (positive for all 3 antiphospholipid tests: lupus anticoagulant, anticardiolipin antibodies, and anti-beta 2-glycoprotein I antibodies). The trial was terminated prematurely after the enrollment of 120 patients due to an excess of events among patients in the rivaroxaban arm. Mean follow-up was 569 days. Fifty-nine patients were randomized to rivaroxaban 20 mg (15 mg for patients with creatinine clearance <50 mL/min) and 61 to warfarin (INR 2.0-3.0).
Thromboembolic events occurred in 12% of patients randomized to rivaroxaban (4 ischaemic stroke and 3 myocardial infarction). No events were reported in patients randomized to warfarin. Major bleeding occurred in 4 patients (7%) of the rivaroxaban group and 2 patients (3%) of the warfarin group.
Pharmacokinetics: Absorption and Bioavailability: Rivaroxaban is rapidly absorbed with maximum concentrations (C
max) appearing 2-4 hours after tablet intake.
Oral absorption of rivaroxaban is almost complete and oral bioavailability is high (80 - 100%) for the 10 mg tablet dose, irrespective of fasting/fed conditions. Intake with food does not affect rivaroxaban AUC or C
max at the 10 mg dose. Xarelto 10 mg tablets can be taken with or without food (see 'Dosage & Administration').
Due to reduced extent of absorption an oral bioavailability of 66% was determined for the 20 mg tablet under fasting conditions. When Xarelto 20 mg tablets are taken together with food increases in mean AUC by 39% were observed when compared to tablet intake under fasting conditions, indicating almost complete absorption and high oral bioavailability. Xarelto 15 mg and 20 mg should be taken with food (see 'Dosage & Administration').
Under fed condition Xarelto 10 mg, 15 mg and 20 mg tablets demonstrated dose-proportionality.
Variability in rivaroxaban pharmacokinetics is moderate with inter-individual variability (CV%) ranging from 30% to 40%.
Distribution: Plasma protein binding in humans is high at approximately 92% to 95%, with serum albumin being the main binding component. The volume of distribution is moderate with V
ss being approximately 50 L.
Metabolism and Elimination: Of the administered rivaroxaban dose, approximately
2/
3 undergoes metabolic degradation, with half then eliminated renally and the other half eliminated by the fecal route. The other
1/
3 of the administered dose undergoes direct renal excretion as unchanged active substance in the urine, mainly via active renal secretion.
Rivaroxaban is metabolized via CYP 3A4, CYP 2J2 and CYP-independent mechanisms. Oxidative degradation of the morpholinone moiety and hydrolysis of the amide bonds are the major sites of biotransformation. Based on
in vitro investigations rivaroxaban is a substrate of the transporter proteins P-gp (P-glycoprotein) and Bcrp (breast cancer resistance protein).
Unchanged rivaroxaban is the most important compound in human plasma with no major or active circulating metabolites being present. With a systemic clearance of about 10 L/h rivaroxaban can be classified as low-clearance drug. Elimination of rivaroxaban from plasma occurred with terminal half-lives of 5 to 9 hours in young individuals, and with terminal half-lives of 11 to 13 hours in the elderly.
Toxicology: Preclinical safety data: The non-clinical safety evaluation in the data from conventional and appropriate studies of safety pharmacology, single and repeat-dose toxicity, genotoxicity, phototoxicity, and carcinogenicity and toxicity to reproduction reveal no special hazard for humans.
No organ-specific toxicity of rivaroxaban was observed up to the highest doses tested.
Prevention of venous thromboembolism (VTE) in patients undergoing major orthopedic surgery of the lower limbs.
Xarelto is indicated for prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation.
Xarelto is indicated for the treatment of Deep Vein Thrombosis (DVT) and for the prevention of recurrent DVT and Pulmonary Embolism (PE) following an acute DVT in adults.
Xarelto is indicated for the treatment of Pulmonary Embolism (PE) and for the prevention of recurrent PE and DVT.
VTE Treatment: Recommended Dose: Initial Treatment of Acute DVT: 15 mg twice daily for the 1st 3 weeks followed by 20 mg once daily for the continued treatment and the prevention of recurrent DVT and PE.
VTE Prevention in Major Orthopedic Surgery: Recommended Dose: 10 mg taken once daily. Duration of Treatment: After major hip surgery: 5 weeks; major knee surgery: 2 weeks.
Rivaroxaban may be taken with or without food. The initial dose should be taken 6-10 hrs after surgery provided that hemostasis has been established. If a dose is missed, the patient should take rivaroxaban immediately and continue on the following day with the once-daily intake as before.
Special Populations:
Elderly >65 years, Gender and Body Weight: No dose adjustment is required for these patient populations (see Pharmacokinetics under Actions).
Children (From Birth to 16 or 18 years Depending on Local Law): No clinical data available in children.
Patients with Impaired Liver Function: Rivaroxaban is contraindicated in patients with hepatic disease which is associated with coagulopathy leading to a clinically relevant bleeding risk.
No dose adjustment is necessary in patients with other hepatic diseases (see Pharmacology: Pharmacokinetics under Actions).
Limited clinical data in patients with moderate hepatic impairment indicate a significant increase in the pharmacological activity. No clinical data are available for patients with severe hepatic impairment (see Contraindications and Pharmacology: Pharmacokinetics under Actions).
Patients with Impaired Renal Function: No dose adjustment is required if rivaroxaban is administered in patients with mild or moderate renal impairment (see Pharmacology: Pharmacokinetics under Actions).
Limited clinical data for patients with severe renal impairment indicate that rivaroxaban plasma levels are significantly increased in this patient population.
Therefore, rivaroxaban must be used with caution in these patients. Use of rivaroxaban is not recommended in patients with CrCl <15 mL/min (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Ethnic Differences: No dose adjustment is required based on ethnic differences (see Pharmacokinetics under Actions).
SPAF - Dosage and method of administration: SPAF: Method of administration: Oral use.
SPAF: Recommended usual dose: The recommended dose is 20 mg once daily.
For patients with
moderate renal impairment (creatinine clearance (CrC): <50-30 mL/min) the recommended dose is 15 mg once daily.
SPAF: Method and frequency of administration: One 20 mg tablet of Xarelto should be taken once daily.
For patients with moderate renal impairment (CrC: <50-30 mL/min) one 15 mg tablet of Xarelto should be taken once daily.
Xarelto 15 mg tablets and Xarelto 20 mg tablets should be taken with food.
For patients who are unable to swallow whole tablets, Xarelto tablet may be crushed and mixed with water or soft foods such as applesauce immediately prior to use and administered orally. After the administration of crushed Xarelto 15 mg or Xarelto 20 mg tablets, the dose should be immediately followed by food.
The crushed Xarelto tablet may be given through gastric tubes. Gastric placement of the tube should be confirmed before administering Xarelto. The crushed tablet should be administered in a small amount of water via a gastric tube after which it should be flushed with water. After the administration of crushed Xarelto 15 mg or 20 mg tablets, the dose should then be immediately followed by enteral feeding (see 'Pharmacology: Pharmacokinetics under Actions').
SPAF: Missed Dose: If a dose is missed the patient should take Xarelto immediately and continue with the once daily intake as recommended on the following day.
The dose should not be doubled to make up for a missed dose within the same day.
SPAF: Maximum daily dose: The recommended maximum daily dose is 20 mg.
SPAF: Additional information on special populations: SPAF: Patients with hepatic impairment: Xarelto is contraindicated in patients with hepatic disease which is associated with coagulopathy leading to a clinically relevant bleeding risk (see 'Contraindications').
No dose adjustment is necessary in patients with other hepatic diseases.
Limited clinical data in patients with moderate hepatic impairment indicate a significant increase in the pharmacological activity. No clinical data are available for patients with severe hepatic impairment (see 'Contraindications').
SPAF: Patients with renal impairment: No dose adjustment is required if Xarelto is administered in patients with mild renal impairment.
For patients with moderate renal impairment the recommended dose is 15 mg once daily.
Limited clinical data for patients with severe renal impairment indicate that rivaroxaban plasma levels are significantly increased in this patient population. Therefore, Xarelto 15 mg must be used with caution in these patients (see 'Precautions').
Use of Xarelto is not recommended in patients with CrC <15 mL/min (see 'Precautions').
SPAF: Converting from Vitamin K Antagonists (VKA) to Xarelto: VKA treatment should be stopped and Xarelto therapy should be initiated when the INR is ≤ 3.0. When converting patients from VKAs to Xarelto, INR values will be falsely elevated after the intake of Xarelto. The INR is not valid to measure the anticoagulant activity of Xarelto, and therefore should not be used (see 'Interactions').
SPAF: Converting from Xarelto to Vitamin K antagonists (VKA): There is a potential for inadequate anticoagulation during the transition from Xarelto to VKA. Continuous adequate anticoagulation should be ensured during any transition to an alternate anticoagulant. It should be noted that Xarelto can contribute to an elevated INR.
In patients converting from Xarelto to VKA, VKA should be given concurrently until the INR is ≥2.0. For the first two days of the conversion period, standard VKA dosing should be used followed by VKA dosing guided by INR testing. While patients are on both Xarelto and VKA, the INR should not be tested earlier than 24 hours (after the previous dose but prior to the next dose of Xarelto. Once Xarelto is discontinued INR testing may be done reliably 24 hours after the last dose (see 'Interactions').
SPAF: Converting from parenteral anti-coagulants to Xarelto: For patients currently receiving a parenteral anticoagulant, start Xarelto 0 to 2 hours before the time of the next scheduled administration of the parenteral drug (e.g. LMWH) or at the time of discontinuation of a continuously administered parenteral drug (e.g. intravenous unfractionated heparin).
SPAF: Converting from Xarelto to parenteral anti-coagulants: Discontinue Xarelto and give the first dose of parenteral anticoagulant at the time that the next Xarelto dose would be taken.
SPAF: Cardioversion: Xarelto can be initiated or continued in patients who may require cardioversion.
For transesophageal echocardiogram (TEE) guided cardioversion in patients not previously treated with anticoagulants, Xarelto treatment should be started at least 4 hours before cardioversion to ensure adequate anticoagulation.
SPAF: Patients who undergo PCI (percutaneous coronary intervention) with stent placement: Patients with non-valvular atrial fibrillation who undergo PCI with stent placement should receive reduced dose of 15 mg Xarelto once daily (or 10 mg Xarelto once daily for patients with moderate renal impairment [CrCl: <50-30 mL/min]) in addition to a P2Y12 inhibitor. This treatment regimen is recommended for a maximum of 12 months after PCI with stent placement (see 'Precautions' and 'Pharmacology: Pharmacodynamics under Actions'). After completion of the antiplatelet therapy, rivaroxaban dosage should be increased to the standard dose for patients with non-valvular atrial fibrillation.
SPAF: Children and adolescents (from birth to 16 or 18 years depending on local law): Safety and efficacy have not been established in children and adolescents below 18 years.
SPAF: Geriatric patients: No dose adjustment is required based on age.
SPAF: Gender: No dose adjustment is required based on gender.
SPAF: Body weight: No dose adjustment is required based on body weight.
SPAF: Ethnic differences: No dose adjustment is required based on ethnic differences.
Treatment and prevention of recurrent DVT and PE - Dosage and method of administration: Treatment and prevention of recurrent DVT and PE: Method of administration: Oral use.
Treatment and prevention of recurrent DVT and PE: Recommended usual dose: The recommended dose for the initial treatment of acute DVT and PE is Xarelto 15 mg twice daily for the first three weeks followed by Xarelto 20 mg once daily for the continued treatment and the prevention of recurrent DVT and PE.
Following completion of at least 6 months treatment for DVT or PE, Xarelto 10 mg once daily or Xarelto 20 mg once daily is recommended based on an individual assessment of the risk of recurrent DVT or PE against the risk for bleeding. (See Table 6.)
Click on icon to see table/diagram/image
Treatment and prevention of recurrent DVT and PE: Method and frequency of administration: During the initial 3 weeks of acute treatment 15 mg of Xarelto should be taken twice daily. After the initial 3 weeks treatment Xarelto should be continued at 20 mg once daily.
After at least 6 months treatment Xarelto should be taken at 10 mg once daily or 20 mg once daily.
Xarelto 15 mg tablets and Xarelto 20 mg tablets should be taken with food.
For patients who are unable to swallow whole tablets, Xarelto tablet may be crushed and mixed with water or soft foods such as applesauce immediately prior to use and administered orally. After the administration of crushed Xarelto 15 mg or Xarelto 20 mg tablets, the dose should be immediately followed by food.
The crushed Xarelto tablet may be given through gastric tubes. Gastric placement of the tube should be confirmed before administering Xarelto. The crushed tablet should be administered in a small amount of water via a gastric tube after which it should be flushed with water. After the administration of crushed Xarelto 15 mg or 20 mg tablets, the dose should then be immediately followed by enteral feeding (see 'Pharmacology: Pharmacokinetics under Actions').
Treatment and prevention of recurrent DVT and PE: Missed Dose: It is essential to adhere to the dosage schedule provided.
If a dose is missed during the 15 mg twice daily treatment phase the patient should take Xarelto immediately to ensure intake of 30 mg Xarelto per day. In this case two 15 mg tablets may be taken at once. The patient should continue with the regular 15 mg twice daily intake as recommended on the following day.
If a dose is missed during the once daily treatment phase the patient should take Xarelto immediately to ensure intake of the recommended daily dose. The patient should continue with the regular once daily dose as recommended on the following day.
Treatment and prevention of recurrent DVT and PE: Maximum daily dose: The recommended maximum daily dose is 30 mg during the first 3 weeks of treatment. In the following treatment phase the recommended maximum daily dose is 20 mg.
Treatment and prevention of recurrent DVT and PE: Additional information on special populations: Treatment and prevention of recurrent DVT and PE: Patients with hepatic impairment: Xarelto is contraindicated in patients with hepatic disease which is associated with coagulopathy leading to a clinically relevant bleeding risk (see 'Contraindications').
No dose adjustment is necessary in patients with other hepatic diseases.
Limited clinical data in patients with moderate hepatic impairment indicate a significant increase in the pharmacological activity.
No clinical data are available for patients with severe hepatic impairment (see 'Contraindications').
Treatment and prevention of recurrent DVT and PE: Patients with renal impairment: No dose adjustment is required if Xarelto is administered in patients with mild or moderate renal impairment.
Limited clinical data for patients with severe renal impairment indicate that rivaroxaban plasma levels are significantly increased in this patient population. Therefore Xarelto must be used with caution in these patients (see 'Precautions').
Use of Xarelto is not recommended in patients with CrC: <15 mL/min (see 'Precautions').
Treatment and prevention of recurrent DVT and PE: Converting from Vitamin K Antagonists (VKA) to Xarelto: VKA treatment should be stopped and Xarelto therapy should be initiated once the INR is ≤ 2.5.
When converting patients from VKAs to Xarelto, INR values will be falsely elevated after the intake of Xarelto. The INR is not valid to measure the anticoagulant activity of Xarelto, and therefore should not be used (see 'Interactions').
Treatment and prevention of recurrent DVT and PE: Converting from Xarelto to Vitamin K antagonists (VKA): There is a potential for inadequate anticoagulation during the transition from Xarelto to VKA. Continuous adequate anticoagulation should be ensured during any transition to an alternate anticoagulant. It should be noted that Xarelto can contribute to an elevated INR.
In patients converting from Xarelto to VKA, VKA should be given concurrently until the INR is ≥2.0. For the first two days of the conversion period, standard VKA dosing should be used followed by VKA dosing guided by INR testing. While patients are on both Xarelto and VKA, the INR should not be tested earlier than 24 hours (after the previous dose but prior to the next dose of Xarelto. Once Xarelto is discontinued INR testing may be done reliably 24 hours after the last dose (see 'Interactions').
Treatment and prevention of recurrent DVT and PE: Converting from parenteral anti-coagulants to Xarelto: For patients currently receiving a parenteral anticoagulant, start Xarelto 0 to 2 hours before the time of the next scheduled administration of the parenteral drug (e.g. LMWH) or at the time of discontinuation of a continuously administered parenteral drug (e.g. intravenous unfractionated heparin).
Treatment and prevention of recurrent DVT and PE: Converting from Xarelto to parenteral anti-coagulants: Discontinue Xarelto and give the first dose of parenteral anticoagulant at the time that the next Xarelto dose would be taken.
Treatment and prevention of recurrent DVT and PE: Children and adolescents (from birth to 16 or 18 years depending on local law): Safety and efficacy have not been established in children and adolescents below 18 years.
Treatment and prevention of recurrent DVT and PE: Geriatric patients: No dose adjustment is required based on age.
Treatment and prevention of recurrent DVT and PE: Gender: No dose adjustment is required based on gender.
Treatment and prevention of recurrent DVT and PE: Body weight: No dose adjustment is required based on body weight.
Treatment and prevention of recurrent DVT and PE: Ethnic differences: No dose adjustment is required based on ethnic differences.
Rare cases of overdose up to 600 mg have been reported without bleeding complications or other adverse reactions. Due to limited absorption a ceiling effect with no further increase in average plasma exposure is expected at supratherapeutic doses of 50 mg or above.
A specific antidote antagonizing the pharmacodynamic effect of rivaroxaban is not available. The use of activated charcoal to reduce absorption in case of Xarelto overdose may be considered. Due to the high plasma protein binding rivaroxaban is not expected to be dialyzable.
Management of Bleeding: Should a bleeding complication arise in a patient receiving rivaroxaban, the next administration should be delayed or treatment should be discontinued as appropriate. Rivaroxaban has a half-life of approximately 5 to 13 hours. Management should be individualized according to the severity and location of the hemorrhage. Appropriate symptomatic treatment could be used as needed, such as mechanical compression (e.g., for severe epistaxis), surgical hemostasis with bleeding control procedures, fluid replacement and hemodynamic support, blood products (packed red cells or fresh frozen plasma, depending on associated anemia or coagulopathy) or platelets.
If bleeding cannot be controlled by the previously mentioned measures, administration of a specific procoagulant reversal agent should be considered, such as prothrombin complex concentrate (PCC), activated prothrombin complex concentrate (APCC), or recombinant factor VIIa (r-FVIIa). However, there is currently very limited clinical experience with the use of these products in individuals receiving Xarelto.
Protamine sulfate and vitamin K are not expected to affect the anticoagulant activity of rivaroxaban.
There is limited experience with tranexamic acid and no experience with aminocaproic acid and aprotinin in individuals receiving Xarelto. There is neither scientific rationale for benefit nor experience with the systemic hemostatic desmopressin in individuals receiving Xarelto.
Xarelto is contraindicated in patients with hypersensitivity to rivaroxaban or any excipient of the tablet (see 'Description').
Xarelto is contraindicated in patients with clinically significant active bleeding (e.g., intracranial bleeding, gastrointestinal bleeding).
Xarelto is contraindicated in patients with hepatic disease which is associated with coagulopathy leading to a clinically relevant bleeding risk.
Safety and efficacy of Xarelto have not been established in pregnant women. Animal data show that rivaroxaban crosses the placental barrier. Therefore use of Xarelto is contraindicated throughout pregnancy (see 'Use in Pregnancy & Lactation').
Safety and efficacy of Xarelto have not been established in nursing mothers. Animal data indicate that rivaroxaban is secreted into breast milk. Therefore Xarelto may only be administered after breastfeeding is discontinued (see 'Use in Pregnancy & Lactation').
Patients with prosthetic heart valves: Xarelto is not recommended for thromboprophylaxis in patients having recently undergone transcatheter aortic valve replacement (TAVR) based on data from a randomized controlled clinical study comparing a Xarelto-regimen to an antiplatelet regimen.
The safety and efficacy of Xarelto have not been studied in patients with other prosthetic heart valves or other valve procedures; therefore, there are no data to support that Xarelto provides adequate anticoagulation in those patient populations.
Patients with high risk triple positive antiphospholipid syndrome: Xarelto is not recommended for patients with a history of thrombosis who are diagnosed with antiphospholipid syndrome and are persistently triple positive (for lupus anticoagulant, anticardiolipin antibodies, and anti-beta 2-glycoprotein I antibodies) as treatment with rivaroxaban is associated with an increased rate of recurrent thrombotic events compared with vitamin K antagonists (VKA).
Concomitant medication: Xarelto is not recommended in patients receiving concomitant systemic treatment with azole-antimycotics (e.g. ketoconazole) or HIV protease inhibitors (e.g. ritonavir). These drugs are strong inhibitors of both CYP 3A4 and P-gp. Therefore, these drugs may increase rivaroxaban plasma concentrations to a clinically relevant degree (2.6-fold on average) which may lead to an increased bleeding risk (see 'Interactions').
The azole anti-mycotic fluconazole, a moderate CYP 3A4 inhibitor, has however less effect on rivaroxaban exposure and can be co-administered (see 'Interactions').
Treatment and prevention of recurrent DVT and PE: Renal impairment: Xarelto is to be used with caution in patients with moderate renal impairment receiving co-medications leading to increased rivaroxaban plasma concentrations (see 'Interactions').
SPAF, treatment and prevention of recurrent DVT and PE: Renal impairment: In patients with severe renal impairment rivaroxaban plasma levels may be significantly elevated (1.6-fold on average) which may lead to an increased bleeding risk.
Due to limited clinical data Xarelto should be used with caution in patients with CrC <30 - 15 mL/min.
No clinical data are available for patients with severe renal impairment. Therefore use of Xarelto is not recommended in these patients (see 'Dosage & Administration').
Patients with severe renal impairment or increased bleeding risk and patients receiving concomitant systemic treatment with azole-antimycotics or HIV protease inhibitors are to be carefully monitored for signs of bleeding complications after initiation of treatment (see 'Interactions').
Bleeding risk: Xarelto like other antithrombotics should be used with caution in patients with an increased bleeding risk such as: congenital or acquired bleeding disorders; uncontrolled severe arterial hypertension; active ulcerative gastrointestinal disease; recent gastrointestinal ulcerations; vascular retinopathy; recent intracranial or intracerebral hemorrhage; intraspinal or intracerebral vascular abnormalities; recent brain, spinal or ophthalmological surgery; bronchiectasis or history of pulmonary bleeding.
Bleeding during antithrombotic treatment may unmask underlying yet unknown malignancy, in particular in the gastrointestinal or genitourinary tract. Patients with malignant disease may simultaneously be at higher risk of bleeding and thrombosis. The individual benefit of antithrombotic treatment should be weighed against risk for bleeding in patients with active cancer dependent on tumor location, antineoplastic therapy and stage of disease.
Care should be taken if patients are treated concomitantly with drugs affecting hemostasis such as non-steroidal anti-inflammatory drugs (NSAIDs), platelet aggregation inhibitors, other antithrombotics or selective serotonin reuptake inhibitors (SSRI), and serotonin norepinephrine reuptake inhibitors (SNRIs) (see 'Interactions').
For patients at risk of ulcerative gastrointestinal disease an appropriate prophylactic treatment may be considered (see 'Interactions').
Any unexplained fall in hemoglobin or blood pressure should lead to a search for a bleeding site.
Surgery and interventions: If an invasive procedure or surgical intervention is required, Xarelto should be stopped at least 24 hours before the intervention, if possible and based on clinical judgment of the physician.
If the procedure cannot be delayed, the increased risk of bleeding should be assessed against the urgency of the intervention.
Xarelto should be restarted as soon as possible after the invasive procedure or surgical intervention provided the clinical situation allows and adequate hemostasis has been established.
Neuraxial (epidural/spinal) anesthesia: When neuraxial (epidural/spinal) anesthesia or spinal puncture is performed, patients treated with antithrombotics for prevention of thromboembolic complications are at risk for development of an epidural or spinal hematoma which may result in long-term paralysis.
The risk of these events is even further increased by use of indwelling epidural catheters or the concomitant use of drugs affecting hemostasis. The risk may also be increased by traumatic or repeated epidural or spinal puncture.
Patients should be frequently monitored for signs and symptoms of neurological impairment (e.g., numbness or weakness of the legs, bowel or bladder dysfunction). If neurological deficits are noted, urgent diagnosis and treatment is necessary.
The physician should consider the potential benefit versus the risk before neuraxial intervention in patients anticoagulated or to be anticoagulated for thromboprophylaxis.
There is no clinical experience with the use of 15 mg and 20 mg rivaroxaban in these situations.
For the removal of an epidural catheter and based on the general PK characteristics at least 2x half-life should elapse, i.e. at least 18 hour in young patients and 26 hours in elderly patients, after the last administration of Xarelto.
Xarelto should be administered at earliest 6 hours after the removal of the catheter.
If traumatic puncture occurs, the administration of Xarelto should be delayed for 24 hours.
Treatment and prevention of recurrent DVT and PE: Haemodynamically unstable PE patients or patients who require thrombolysis or pulmonary embolectomy: Xarelto is not recommended as an alternative to unfractionated heparin in patients with pulmonary embolism who are haemodynamically unstable or may receive thrombolysis or pulmonary embolectomy since the safety and efficacy of Xarelto have not been established in these clinical situations.
SPAF: Patients who undergo PCI with stent placement: Clinical data are available from an interventional study with the primary objective to assess safety in patients with non-valvular atrial fibrillation who undergo PCI with stent placement. Data on efficacy in this population are limited (see 'Dosage & Administration').
Effects on ability to drive or use machines: Syncope and dizziness have been reported and may affect the ability to drive and use machines (see 'Adverse Reactions'). Patients experiencing these adverse reactions should not drive or use machines.
Use in Pregnancy: Women of childbearing potential: Xarelto should be used in women of childbearing potential only with effective contraception.
Women of childbearing potential/Contraception: Xarelto should be used in women of childbearing potential only with effective contraception.
Pregnancy: Safety and efficacy of Xarelto have not been established in pregnant women.
In rats and rabbits rivaroxaban showed pronounced maternal toxicity with placental changes related to its pharmacological mode of action (e.g., hemorrhagic complications) leading to reproductive toxicity. No primary teratogenic potential was identified. Due to the intrinsic risk of bleeding and the evidence that rivaroxaban passes the placenta, Xarelto is contraindicated in pregnancy (see 'Contraindications').
Lactation: Safety and efficacy of Xarelto have not been established in nursing mothers. In rats rivaroxaban is secreted into breast milk.
Therefore Xarelto may only be administered after breastfeeding is discontinued (see 'Contraindications').
Summary of the safety profile: The safety of rivaroxaban has been evaluated in
thirteen phase III studies including
53,103 patients exposed to rivaroxaban,
as listed in the following tables: See Tables 7 and 8.
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Due to the pharmacological mode of action, Xarelto may be associated with an increased risk of occult or overt bleeding from any tissue and organ which may result in post hemorrhagic anemia. The risk of bleedings may be increased in certain patient groups e.g. patients with uncontrolled severe arterial hypertension and/or on concomitant medication affecting hemostasis (see 'Precautions').
The signs, symptoms, and severity (including fatal outcome) will vary according to the location and degree or extent of the bleeding and/or
anemia (see 'Management of Bleeding under Overdosage').
Hemorrhagic complications may present as weakness, paleness, dizziness, headache or unexplained swelling,
dyspnea, and unexplained shock. In some cases as a consequence of anemia, symptoms of cardiac ischemia like chest pain or angina pectoris have been observed.
Known complications secondary to severe bleeding such as compartment syndrome and renal failure due to hypoperfusion have been reported for Xarelto. Therefore, the possibility of a hemorrhage should be considered in evaluating the condition in any anticoagulated patient.
Tabulated list of adverse reactions: The frequencies of ADRs reported with Xarelto are summarized in the table as follows. Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness. Frequencies are defined as: very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1,000 to < 1/100), rare (≥ 1/10,000 to < 1/1,000). (See Table 9.)
Click on icon to see table/diagram/image
Post marketing observations: The following adverse reactions have been reported post-marketing in temporal association with the use of Xarelto: Immune system disorders: Angioedema and allergic oedema.
Hepatobiliary disorders: Cholestasis, Hepatitis (incl. hepatocellular injury).
Blood and lymphatic system disorders: Thrombocytopenia.
Pharmacokinetic interactions: Rivaroxaban is cleared mainly via cytochrome P450-mediated (CYP3A4, CYP2J2) hepatic metabolism and renal excretion of the unchanged drug, involving the P-glycoprotein (P-gp)/breast cancer resistance protein (Bcrp) transporter systems.
CYP Inhibition: Rivaroxaban does not inhibit CYP3A4 or any other major CYP isoforms.
CYP Induction: Rivaroxaban does not induce CYP 3A4 or any other CYP isoforms.
Effects on rivaroxaban: The concomitant use of Xarelto with strong CYP 3A4 and P-gp inhibitors may lead to both reduced hepatic and renal clearance and thus significantly increased systemic exposure.
Co-administration of Xarelto with the azole-antimycotic ketoconazole (400 mg once daily) a strong CYP 3A4 and P-gp inhibitor, led to a 2.6-fold increase in mean rivaroxaban steady state AUC and a 1.7-fold increase in mean rivaroxaban Cmax, with significant increases in its pharmacodynamic effects.
Co-administration of Xarelto with the HIV protease inhibitor ritonavir (600 mg twice daily), a strong CYP 3A4 and P-gp inhibitor, led to a 2.5-fold increase in mean rivaroxaban AUC and a 1.6-fold increase in mean rivaroxaban Cmax, with significant increases in its pharmacodynamic effects. Therefore Xarelto is not recommended in patients receiving concomitant systemic treatment with azole-antimycotics or HIV-protease inhibitors (see Precautions).
Clarithromycin (500 mg twice daily), considered as strong CYP 3A4 inhibitor and moderate P-gp inhibitor, led to a 1.5-fold increase in mean rivaroxaban AUC and a 1.4-fold increase in Cmax. This increase, which is close to the magnitude of the normal variability of AUC and Cmax, is considered as clinically not relevant.
Erythromycin (500 mg three times daily), which inhibits CYP 3A4 and P-gp moderately, led to a 1.3-fold increase in mean rivaroxaban AUC and Cmax. This increase is within the magnitude of the normal variability of AUC and Cmax and is considered as clinically not relevant.
Fluconazole (400 mg once daily), considered as moderate CYP 3A4 inhibitor, led to a 1.4-fold increase in mean rivaroxaban AUC and a 1.3-fold increase in mean Cmax. This increase is within the magnitude of the normal variability of AUC and Cmax and is considered as clinically not relevant.
Co-administration of Xarelto with the strong CYP 3A4 and P-gp inducer rifampicin led to an approximate 50% decrease in mean rivaroxaban AUC, with parallel decreases in its pharmacodynamic effects.
The concomitant use of Xarelto with other strong CYP 3A4 inducers (e.g., phenytoin, carbamazepine, phenobarbitone or St. John's Wort) may also lead to a decreased rivaroxaban plasma concentration.
Strong CYP 3A4 inducers should be co-administered with caution.
Pharmacodynamic interactions: After combined administration of enoxaparin (40 mg single dose) with Xarelto (10 mg single dose), an additive effect on anti-factor Xa activity was observed without any additional effects on clotting tests (PT, aPTT). Enoxaparin did not affect the pharmacokinetics of rivaroxaban (see 'Precautions').
Clopidogrel (300 mg loading dose followed by 75 mg maintenance dose) did not show a pharmacokinetic interaction (with Xarelto 15 mg) but a relevant increase in bleeding times was observed in a subset of patients which was not correlated to platelet aggregation, P-selectin or GPIIb/IIIa receptor levels (see 'Precautions').
No clinically relevant prolongation of bleeding time was observed after concomitant administration of Xarelto (15 mg) and 500 mg naproxen. Nevertheless there may be individuals with more pronounced pharmacodynamic response (see 'Precautions').
Converting patients from warfarin (INR 2.0 to 3.0) to Xarelto (20 mg) or from Xarelto (20 mg) to warfarin (INR 2.0 to 3.0) increased prothrombin time/INR (Neoplastin) more than additively (individual INR values up to 12 may be observed), whereas effects on aPTT, inhibition of factor Xa activity and endogenous thrombin potential were additive.
If it is desired to test the pharmacodynamic effects of Xarelto during the conversion period, anti-factor Xa activity, PiCT, and HepTest can be used as these tests were not affected by warfarin. From day 4 after stopping warfarin onwards, all tests (including PT, aPTT, inhibition of factor Xa activity and ETP) reflected only the effect of Xarelto (see 'Dosage & Administration').
If it is desired to test the pharmacodynamic effects of warfarin during the conversion period, INR measurement can be used at the Ctrough of rivaroxaban (24 hours after the previous intake of rivaroxaban) as this test is minimally affected by rivaroxaban at this time point.
No pharmacokinetic interaction was observed between warfarin and Xarelto.
As with other anticoagulants the possibility may exist that patients are at increased risk of bleeding in case of concomitant use with SSRIs or SNRIs due to their reported effect on platelets. When concomitantly used in the rivaroxaban clinical program, numerically higher of major or non-major clinically relevant bleeding were observed in all treatment groups.
Food and dairy products: Rivaroxaban 10 mg can be taken with or without food (see Pharmacology: Pharmacokinetics under Actions).
Xarelto 15 mg tablets and Xarelto 20 mg tablets should be taken with food.
Interactions with laboratory parameters: Clotting parameter tests (PT, aPTT, HepTest) are affected as expected by the mode of action of Xarelto.
Incompatibilities: None Known.
Instructions for use/handling: None.
B01AF01 - rivaroxaban ; Belongs to the class of direct factor Xa inhibitors. Used in the treatment of thrombosis.
Xarelto FC tab 10 mg
1 × 10's
Xarelto FC tab 15 mg
3 × 10's
Xarelto FC tab 20 mg
3 × 10's




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image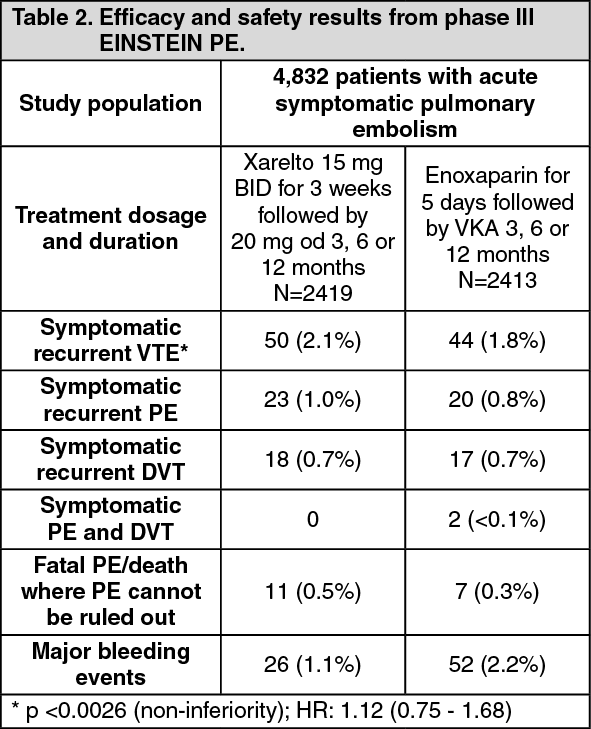 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image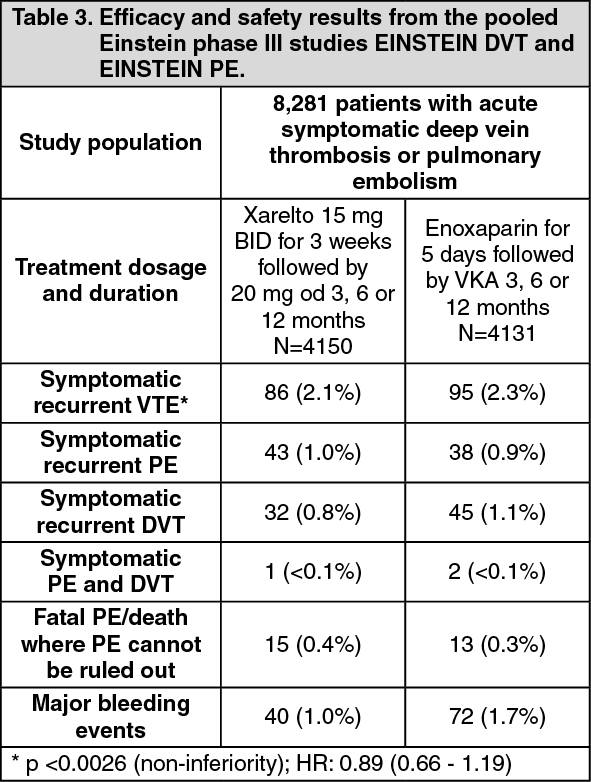 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image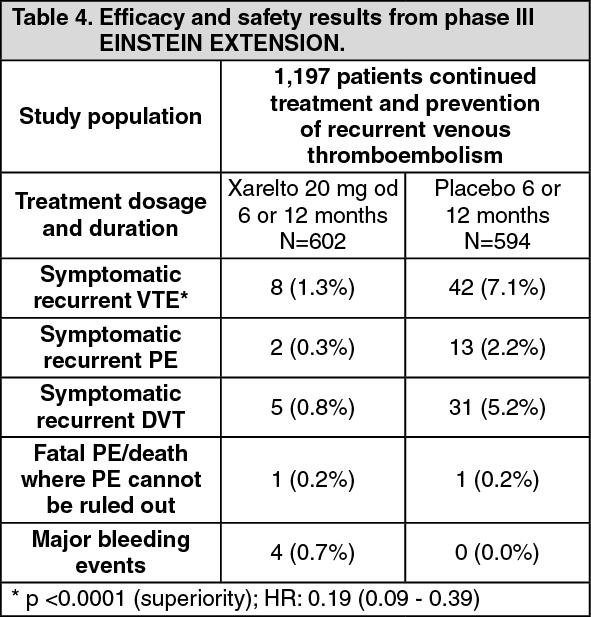 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image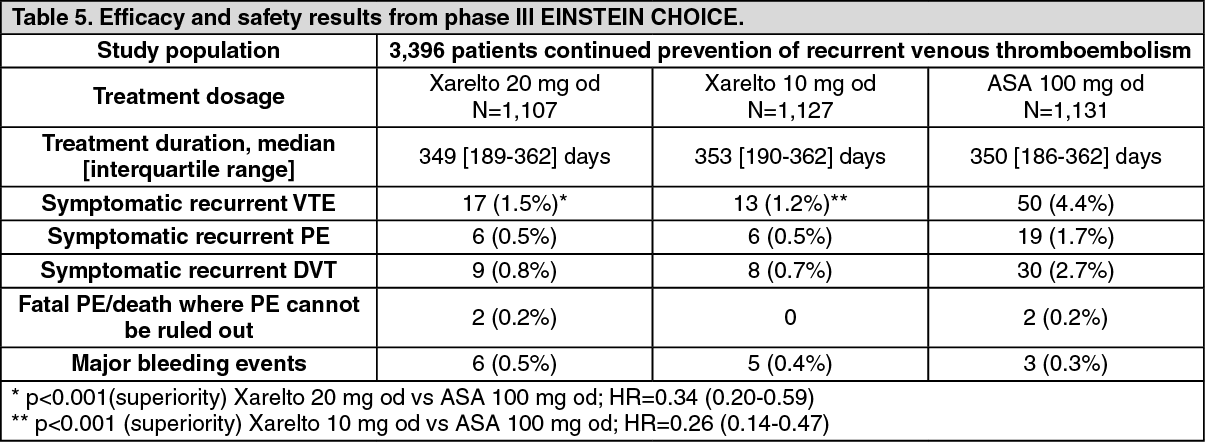 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image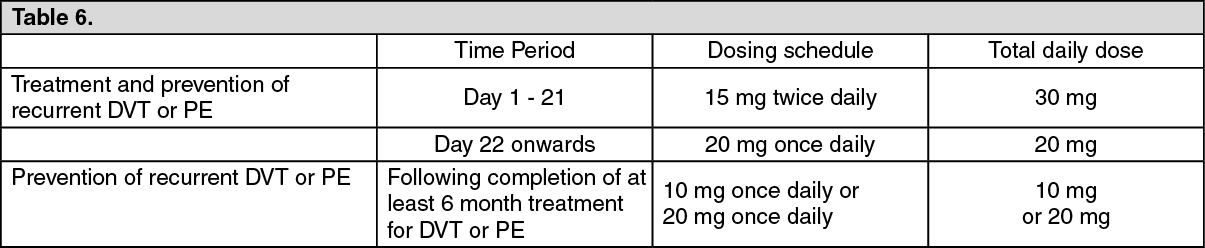 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image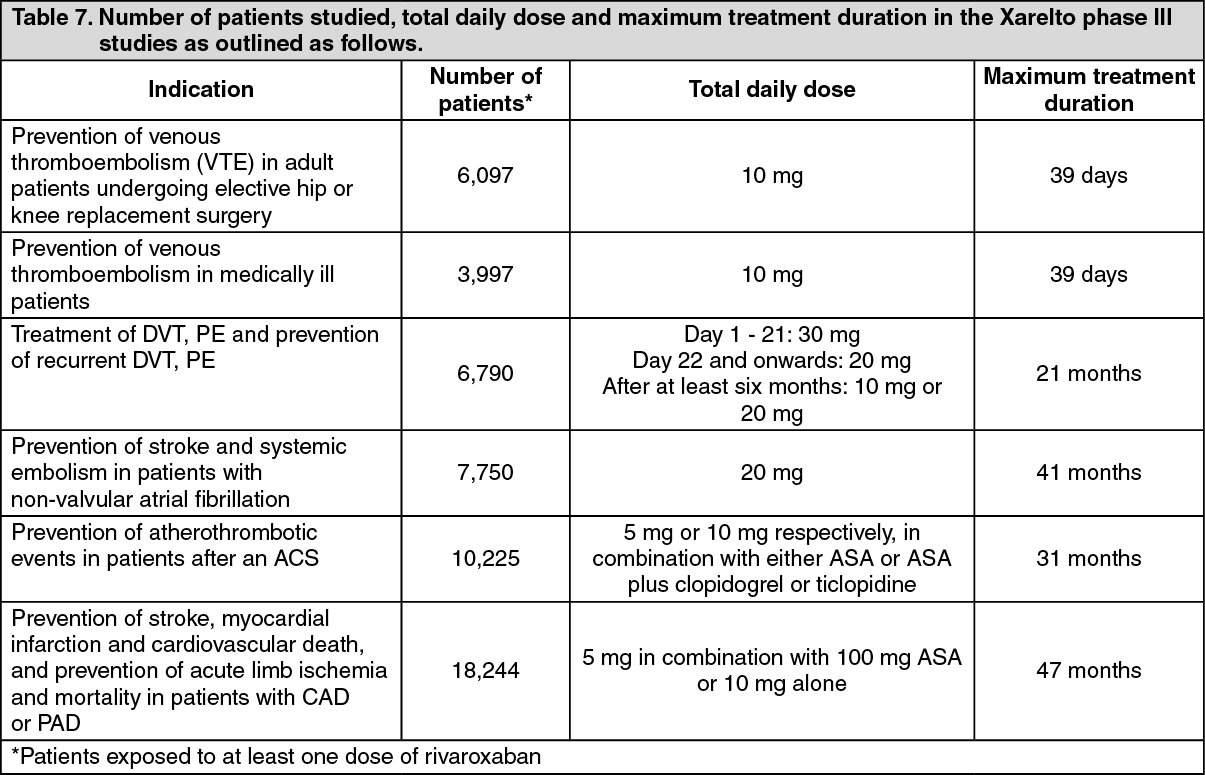 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image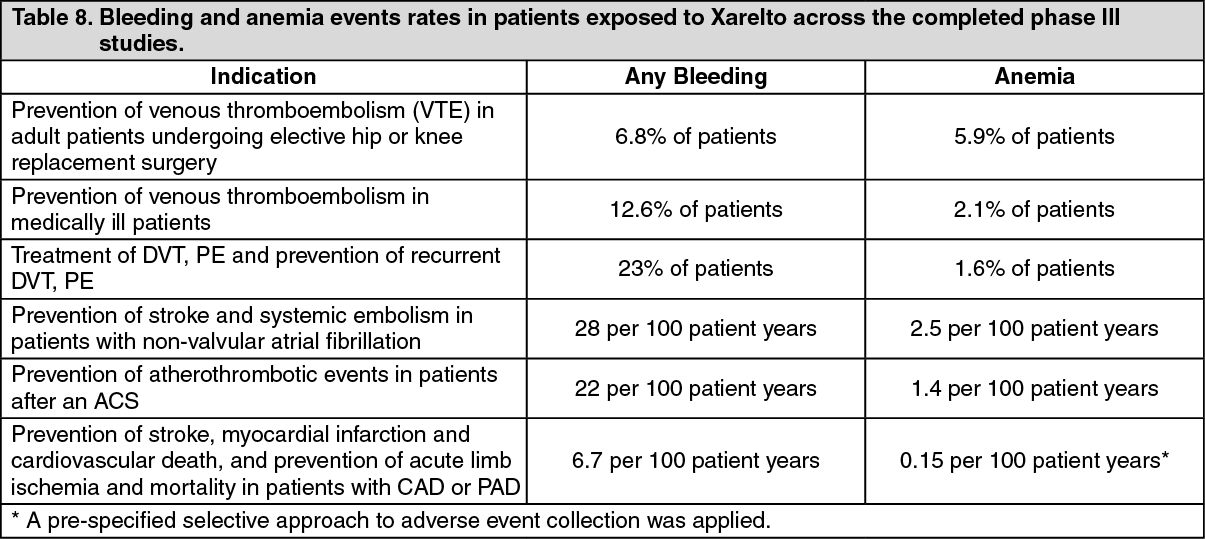 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image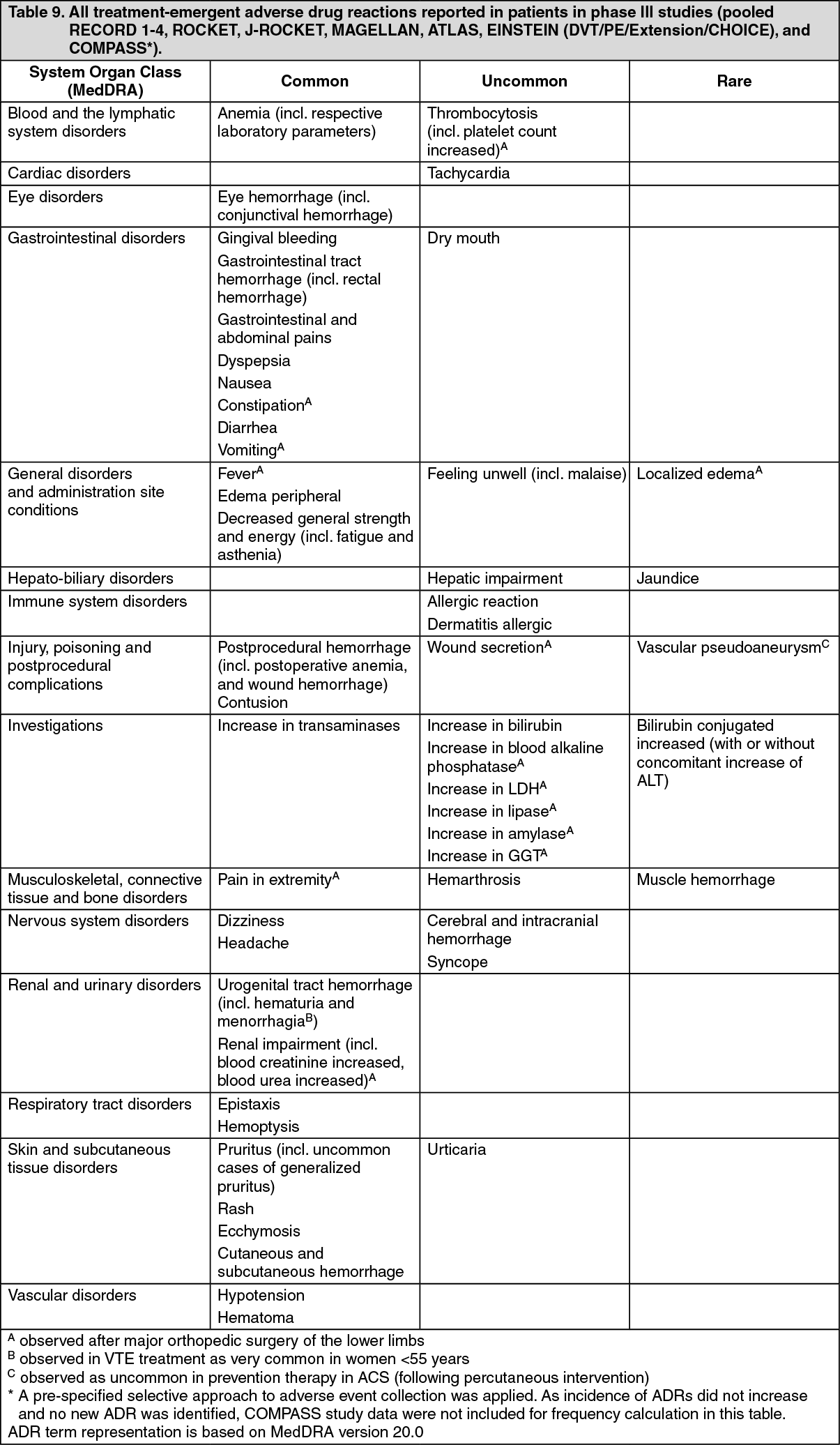 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out