


 Sign Out
Sign Out


All patients in these studies had moderate to severe rheumatoid arthritis. The study XELJANZ population had a mean age of 52.1 years and 83.2% were female.
The long-term safety population includes all patients who participated in a double-blind, controlled study (including earlier development phase studies) and then participated in one of two long-term safety studies.
A total of 6194 patients (Phase 1, 2, 3, and long-term extension studies) were treated with any dose of XELJANZ with a mean duration of 3.13 years, with 19405.8 patient-years of accumulated total drug exposure based on more than 8 years of continuous exposure to XELJANZ.
Safety information from ad hoc interim analyses is also included for one large (N=4362), ongoing randomized PASS study in RA patients who were 50 years or older with at least one cardiovascular risk factor (CV risk factors defined as: current cigarette smoker, diagnosis of hypertension, diabetes mellitus, family history of premature coronary heart disease, history of coronary artery disease including a history of revascularization procedure, coronary artery bypass grafting, myocardial infarction, cardiac arrest, unstable angina, acute coronary syndrome, and presence of extra-articular disease associated with RA, e.g., nodules, Sjögren's syndrome, anemia of chronic disease, pulmonary manifestations), and were on a stable background dose of methotrexate.
Patients were randomized to open-label tofacitinib 10 mg twice daily, tofacitinib 5 mg twice daily, or a TNF inhibitor (TNF inhibitor was either etanercept 50 mg once weekly or adalimumab 40 mg every other week) in a 1:1:1 ratio. The co-primary endpoints are adjudicated malignancy (excluding NMSC) and adjudicated major adverse cardiovascular events (MACE); cumulative incidence and statistical assessment of endpoints are blinded. The study is an event-powered study that also requires at least 1500 patients to be followed for 3 years. The study treatment of tofacitinib 10 mg twice daily has been stopped and the patients were switched to 5 mg twice daily because of a dose dependent signal of PE.
Clinical Trials Experience: The most common serious adverse reactions were serious infections (see Precautions).
The most commonly reported adverse reactions during the first 3 months in controlled clinical trials (occurring in ≥2% of patients treated with XELJANZ monotherapy or in combination with DMARDs) were headache, upper respiratory tract infections, nasopharyngitis, hypertension, nausea, and diarrhea.
The proportion of patients who discontinued treatment due to any adverse reactions during first 3 months of the double-blind, placebo or methotrexate controlled studies was 3.8% for patients taking XELJANZ and 3.2% for placebo-treated patients. The most common infections resulting in discontinuation of therapy were herpes zoster and pneumonia.
The Adverse Drug Reactions (ADRs) listed in the table as follows are presented by System Organ Class (SOC) and frequency categories, defined using the following convention: very common (≥1/10); common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100) or rare (≥1/10,000 to <1/1,000). Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness.
ADRs BY SOC AND CIOMS FREQUENCY CATEGORY LISTED IN ORDER OF DECREASING MEDICAL SERIOUSNESS OR CLINICAL IMPORTANCE WITHIN EACH FREQUENCY CATEGORY AND SOC. (See Table 9.)
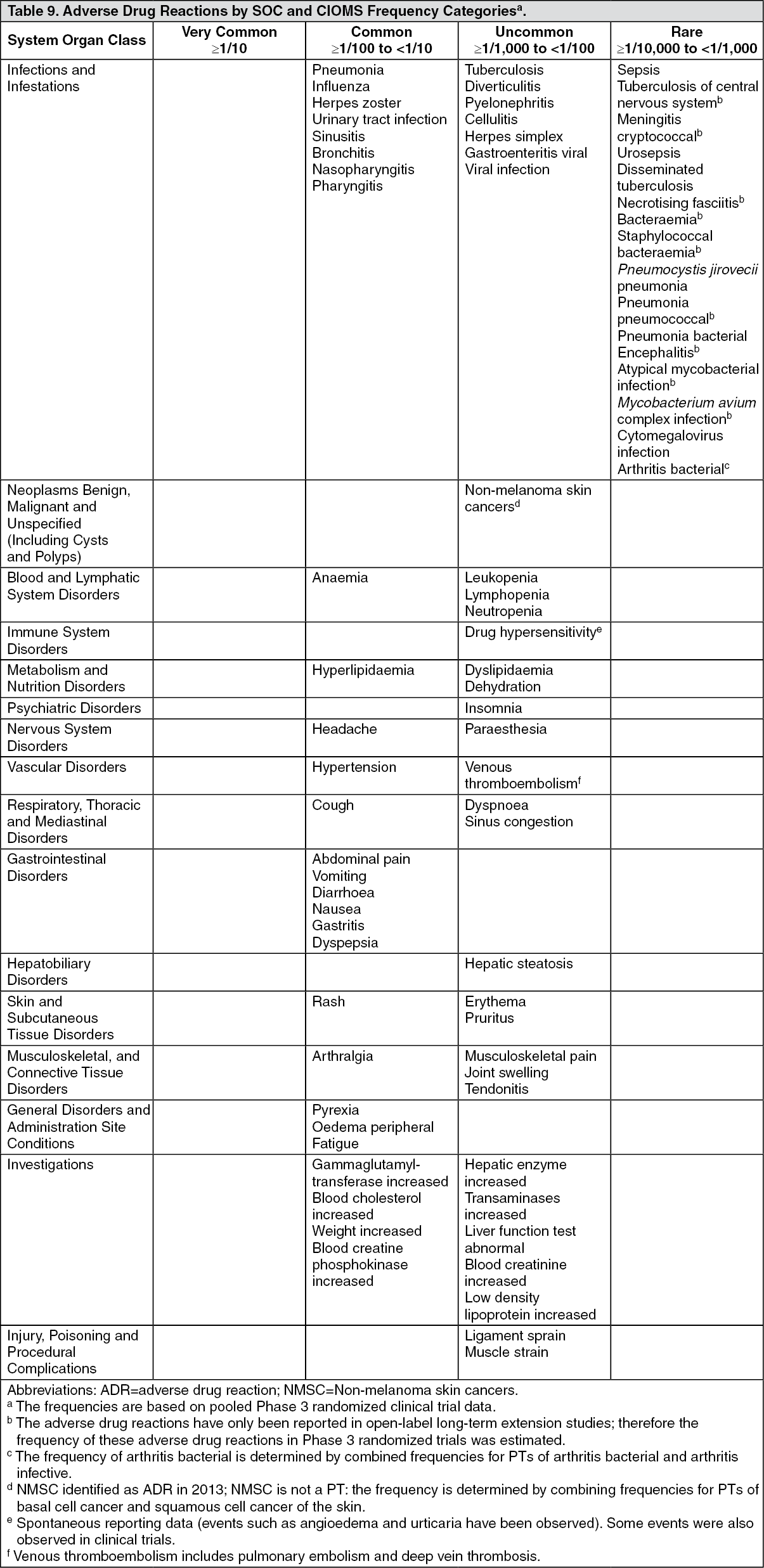 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageOverall Infections: In the 6-month and 24-month, controlled Phase 3 clinical studies the rates of infections in the 5 mg twice daily (total 616 patients) and 10 mg twice daily (total 642 patients) XELJANZ monotherapy group were 16.2% (100 patients), and 17.9% (115 patients), respectively, compared to 18.9% (23 patients) in the placebo group (total 122 patients). In studies of 6-month, 12-month, or 24-month duration with background DMARDs, the rates of infections in the 5 mg twice daily (total 973 patients) and 10 mg twice daily (total 969 patients) XELJANZ plus DMARD group were 21.3% (207 patients) and 21.8% (211 patients), respectively, compared to 18.4% (103 patients) in the placebo plus DMARD group (total 559 patients).
The most commonly reported infections were upper respiratory tract infections and nasopharyngitis (3.7% and 3.2%, respectively).
The overall rate of infections with XELJANZ in the long-term safety all exposure population (total 4867 patients) was 46.1 patients with events per 100 patient-years (43.8 and 47.2 patients with events for 5 mg and 10 mg twice daily, respectively). For patients (total 1750) on monotherapy, the rates were 48.9 and 41.9 patients with events per 100 patient-years for 5 mg and 10 mg twice daily, respectively. For patients (total 3117) on background DMARDs, the rates were 41.0 and 50.3 patients with events per 100 patient-years for 5 mg and 10 mg twice daily, respectively.
Serious Infections: In the 6-month and 24-month, controlled clinical studies, the rate of serious infections in the 5 mg twice daily XELJANZ monotherapy group was 1.7 patients with events per 100 patient-years. In the 10 mg twice daily XELJANZ monotherapy group, the rate was 1.6 patients with events per 100 patient-years, the rate was 0 events per 100 patient-years for the placebo group and the rate was 1.9 patients with events per 100 patient-years for the methotrexate group.
In studies of 6-, 12- or 24-month duration, the rates of serious infections in the 5 mg twice daily and 10 mg twice daily XELJANZ plus DMARD groups were 3.6 and 3.4 patients with events per 100 patient-years, respectively, compared to 1.7 patients with events per 100 patient-years in the placebo plus DMARD group.
In the long-term safety all exposure population, the overall rates of serious infections were 2.4 and 3.0 patients with events per 100 patient-years for 5 mg and 10 mg twice daily XELJANZ groups, respectively. The most common serious infections reported with XELJANZ included pneumonia, herpes zoster, urinary tract infection, cellulitis, gastroenteritis, and diverticulitis. Cases of opportunistic infections have been reported (see Precautions).
Of the 4271 patients who enrolled in Studies I to VI, a total of 608 rheumatoid arthritis patients were 65 years of age and older, including 85 patients 75 years and older. The frequency of serious infection among XELJANZ-treated patients 65 years of age and older was higher than those under the age of 65. As there is a higher incidence of infections in the elderly population in general, caution should be used when treating the elderly.
Viral Reactivation: In XELJANZ clinical trials, Japanese and Korean patients appear to have a higher rate of herpes zoster than that observed in other populations.
Venous Thromboembolism: Ongoing Randomized Post Authorization Safety Surveillance (PASS) Study in Rheumatoid Arthritis Patients: In this ongoing study of patients who were 50 years or older with at least one cardiovascular risk factor, based on interim data (data cut-off date 22 Feb 2019), the incidence rates (IRs) for (95% CI) for PE for tofacitinib 5 mg twice daily, tofacitinib 10 mg twice daily, and TNF inhibitors were 0.27 (0.12, 0.52), 0.54 (0.32, 0.87), and 0.09 (0.02, 0.26) patients with events per 100 patient-years (PYs), respectively. Compared with TNF inhibitors, the hazard ratio (HR) (95%CI) for PE with tofacitinib 5 mg twice daily was 2.99 (0.81, 11.06), and for tofacitinib 10 mg twice daily the HR (95% CI) was 5.96 (1.75, 20.33).
The IRs (95% CI) for DVT for tofacitinib 5 mg twice daily, tofacitinib 10 mg twice daily, and TNF inhibitors were 0.30 (0.14, 0.55), 0.38 (0.20, 0.67), and 0.18 (0.07, 0.39) patients with events per 100 PYs, respectively. Compared with TNF inhibitors, the HR (95% CI) for DVT with tofacitinib5 mg twice daily was 1.66 (0.60, 4.57), and for tofacitinib 10 mg twice daily the HR (95% CI) was 2.13 (0.80, 5.69).
Completed Rheumatoid Arthritis Studies: In the 4 to 12 week placebo period of randomized controlled studies of 4 weeks to 24 months duration, the IRs (95% CI) for tofacitinib 5 mg twice daily, tofacitinib 10 mg twice daily, and placebo for PE were 0.00 (0.00, 0.57), 0.00 (0.00, 0.77), and 0.40 (0.01, 2.22) patients with events per 100 PYs respectively; the IRs (95% CI) for DVT were 0.00 (0.00, 0.57), 0.21 (0.01,1.16), and 0.40 (0.01, 2.22) patients with events per 100 PYs respectively.
In the full randomized period of controlled studies of 4 weeks to 24 months duration, the IRs (95%CI) for tofacitinib 5 mg twice daily and tofacitinib 10 mg twice daily for PE were 0.12 (0.02, 0.34) and 0.15 (0.03, 0.44) patients with events per 100 PYs respectively; the IRs (95% CI) for DVT were 0.15 (0.04, 0.40) and 0.10 (0.01, 0.36) patients with events per 100 PYs respectively.
In the long term safety population that includes exposure during completed randomized controlled studies and open label long-term extension studies, the IRs (95% CI) for tofacitinib 5 mg twice daily and tofacitinib 10 mg twice daily for PE were 0.12 (0.06, 0.22) and 0.13 (0.08, 0.21) patients with events per 100 PYs respectively; the IRs (95% CI) for DVT were 0.17 (0.09, 0.27) and 0.15 (0.09, 0.22) patients with events per 100 PYs respectively.
Clinical Experience in Methotrexate-Naïve Rheumatoid Arthritis Patients: Study VI was an active-controlled clinical trial in methotrexate-naïve RA patients (see Pharmacology: Pharmacodynamics under Actions). The safety experience in these patients was consistent with Studies I-V.
Laboratory Tests: Lymphocytes: In the controlled clinical studies, confirmed decreases in lymphocyte counts below 500 cells/mm3 occurred in 0.23% of patients for the 5 mg twice daily and 10 mg twice daily doses combined.
In the long-term safety population, confirmed decreases in lymphocyte counts below 500 cells/mm3 occurred in 1.3% of patients for the 5 mg twice daily and 10 mg twice daily doses combined.
Confirmed lymphocyte counts <500 cells/mm3 were associated with an increased incidence of treated and serious infections (see Precautions).
Neutrophils: In the controlled clinical studies confirmed decreases in ANC below 1000 cells/mm3 occurred in 0.08% of patients for the 5 mg twice daily and 10 mg twice daily doses combined. There were no confirmed decreases in ANC below 500 cells/mm3 observed in any treatment group. There was no clear relationship between neutropenia and the occurrence of serious infections.
In the long-term safety population, the pattern and incidence of confirmed decreases in ANC remained consistent with what was seen in the controlled clinical studies (see Precautions).
Liver Enzyme Tests: Confirmed increases in liver enzymes >3 times the upper limit of normal (3x ULN) were uncommonly observed. In patients experiencing liver enzyme elevation, modification of treatment regimen, such as reduction in the dose of concomitant DMARD, interruption of XELJANZ, or reduction in XELJANZ dose, resulted in decrease or normalization of liver enzymes.
In the controlled portion of the Phase 3 monotherapy study (0-3 months), (Study I, see Pharmacology: Pharmacokinetics under Actions), ALT elevations >3x ULN were observed in 1.65%, 0.41%, and 0% of patients receiving placebo, XELJANZ 5 mg and 10 mg twice daily, respectively. In this study, AST elevations >3x ULN were observed in 1.65%, 0.41% and 0% of patients receiving placebo, XELJANZ 5 mg, and 10 mg twice daily, respectively.
In the Phase 3 monotherapy study (0-24 months) (Study VI, see Pharmacology: Pharmacodynamics under Actions), ALT elevations >3x ULN were observed in 7.1%, 3.0%, and 3.0% of patients receiving methotrexate, XELJANZ 5 mg, and 10 mg twice daily, respectively. In this study, AST elevations >3x ULN were observed in 3.3%, 1.6% and 1.5% of patients receiving methotrexate, XELJANZ 5 mg, and 10 mg twice daily, respectively.
In the controlled portion of the Phase 3 studies on background DMARDs (0-3 months), (Studies II-V, see Pharmacology: Pharmacodynamics under Actions), ALT elevations >3x ULN were observed in 0.9%, 1.24% and 1.14% of patients receiving placebo, XELJANZ 5 mg, and 10 mg twice daily, respectively. In these studies, AST elevations >3x ULN were observed in 0.72%, 0.5% and 0.31% of patients receiving placebo, XELJANZ 5 mg, and 10 mg twice daily, respectively.
Lipids: Elevations in lipid parameters (total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides) were first assessed at one month following initiation of XELJANZ in the controlled double-blind clinical trials. Increases were observed at this time point and remained stable thereafter. Changes in lipid parameters from baseline through the end of the study (6-24 months) in the controlled clinical studies are summarized as follows: Mean LDL cholesterol increased by 15% in the XELJANZ 5 mg twice daily arm and 20% in the XELJANZ 10 mg twice daily arm at Month 12, and increased by 16% in the XELJANZ 5 mg twice daily arm and 19% in the XELJANZ 10 mg twice daily arm at Month 24.
Mean HDL cholesterol increased by 17% in the XELJANZ 5 mg twice daily arm and 18% in the XELJANZ 10 mg twice daily arm at Month 12, and increased by 19% in the XELJANZ5 mg twice daily arm and 20% in the XELJANZ 10 mg twice daily arm at Month 24.
Mean LDL cholesterol/HDL cholesterol ratios were essentially unchanged in XELJANZ-treated patients.
Apolipoprotein B (ApoB)/ApoA1 ratios were essentially unchanged in XELJANZ-treated patients.
In a controlled clinical trial, elevations in LDL cholesterol and ApoB decreased to pretreatment levels in response to statin therapy.
In the long-term safety populations, elevations in the lipid parameters remained consistent with what was seen in the controlled clinical studies.
View ADR Monitoring Form