


 Sign Out
Sign Out


PHARMACOLOGY: Pharmacodynamics: Mechanism of action: Ceftazidime inhibits bacterial peptidoglycan cell wall synthesis following binding to penicillin binding proteins (PBPs), which leads to bacterial cell lysis and death. Avibactam is a non-β-lactam, β-lactamase inhibitor that acts by forming a covalent adduct with the enzyme that is stable to hydrolysis. It inhibits both Ambler class A and class C β-lactamases and some class D enzymes, including extended-spectrum β-lactamases (ESBLs), KPC and OXA-48 carbapenemases, and AmpC enzymes. Avibactam does not inhibit class B enzymes (metallo-β-lactamases) and is not able to inhibit many class D enzymes.
Resistance: Bacterial resistance mechanisms that could potentially affect ceftazidime/avibactam include mutant or acquired PBPs, decreased outer membrane permeability to either compound, active efflux of either compound, and β-lactamase enzymes refractory to inhibition by avibactam and able to hydrolyse ceftazidime.
Antibacterial activity in combination with other antibacterial agents: No synergy or antagonism was demonstrated in vitro drug combination studies with ceftazidime/avibactam and metronidazole, tobramycin, levofloxacin, vancomycin, linezolid, colistin and tigecycline.
Susceptibility testing breakpoints: Minimum Inhibitory Concentration (MIC) breakpoints established by the European Committee on Antimicrobial Susceptibility Testing (EUCAST) for ceftazidime/avibactam are as follows: See Table 1.
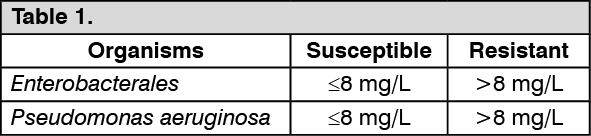 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetic/pharmacodynamic relationship: The antimicrobial activity of ceftazidime against specific pathogens has been shown to best correlate with the percent time of free-drug concentration above the ceftazidime/avibactam minimum inhibitory concentration over the dose interval (% fT >MIC of ceftazidime/avibactam). For avibactam the PK-PD index is the percent time of the free drug concentration above a threshold concentration over the dose interval (% fT >CT).
Clinical efficacy against specific pathogens: Efficacy has been demonstrated in clinical studies against the following pathogens that were susceptible to ceftazidime/avibactam in vitro.
Complicated intra-abdominal infections: Gram-negative micro-organisms: Citrobacter freundii, Enterobacter cloacae, Escherichia coli, Klebsiella oxytoca, Klebsiella pneumoniae, Pseudomonas aeruginosa.
Complicated urinary-tract infections: Gram-negative micro-organisms: Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, Enterobacter cloacae, Pseudomonas aeruginosa.
Hospital-acquired pneumonia including ventilator-associated pneumonia: Gram-negative micro-organisms: Enterobacter cloacae, Escherichia coli, Klebsiella pneumoniae, Proteus mirabilis, Serratia marcescens, Pseudomonas aeruginosa.
Clinical efficacy has not been established against the following pathogens that are relevant to the approved indications although in vitro studies suggest that they would be susceptible to ceftazidime/avibactam in the absence of acquired mechanisms of resistance.
Gram-negative micro-organisms: Citrobacter koseri, Enterobacter aerogenes, Morganella morganii, Proteus vulgaris, Providencia rettgeri.
In vitro data indicate that the following species are not susceptible to ceftazidime/avibactam: Staphylococcus aureus (methicillin-susceptible and methicillin-resistant), Anaerobes, Enterococcus spp., Stenotrophomonas maltophilia, Acinetobacter spp.
Paediatric population: Zavicefta has been evaluated in paediatric patients aged 3 months to < 18 years in two Phase 2 single-blind, randomised, comparative clinical studies, one in patients with cIAI and one in patients with cUTI. The primary objective in each study was to assess safety and tolerability of ceftazidime-avibactam (+/- metronidazole). Secondary objectives included assessment of pharmacokinetics and efficacy; efficacy was a descriptive endpoint in both studies. Clinical cure rate at TOC (ITT) was 91.8% (56/61) for Zavicefta compared to 95.5% (21/22) for meropenem in paediatric patients with cIAI. Microbiological eradication rate at TOC (micro-ITT) was 79.6% (43/54) for Zavicefta compared to 60.9% (14/23) for cefepime in paediatric patients with cUTI.
Pharmacokinetics: Distribution: The human protein binding of both ceftazidime and avibactam is approximately 10% and 8%, respectively. The steady-state volumes of distribution of ceftazidime and avibactam were about 17 L and 22 L, respectively in healthy adults following multiple doses of 2 g/0.5 g ceftazidime/avibactam infused over 2 hours every 8 hours. Both ceftazidime and avibactam penetrate into human bronchial epithelial lining fluid (ELF) to the same extent with concentrations around 30% those in plasma. The concentration time profiles are similar for ELF and plasma.
Penetration of ceftazidime into the intact blood-brain barrier is poor. Ceftazidime concentrations of 4 to 20 mg/L or more are achieved in the CSF when the meninges are inflamed. Avibactam penetration of the blood brain barrier has not been studied clinically; however, in rabbits with inflamed meninges, CSF exposures of ceftazidime and avibactam were 43% and 38% of plasma AUC, respectively. Ceftazidime crosses the placenta readily, and is excreted in the breast milk.
Biotransformation: Ceftazidime is not metabolised. No metabolism of avibactam was observed in human liver preparations (microsomes and hepatocytes). Unchanged avibactam was the major drug-related component in human plasma and urine following dosing with [14C]-avibactam.
Elimination: The terminal half-life (t½) of both ceftazidime and avibactam is about 2 h after intravenous administration. Ceftazidime is excreted unchanged into the urine by glomerular filtration; approximately 80-90% of the dose is recovered in the urine within 24 h. Avibactam is excreted unchanged into the urine with a renal clearance of approximately 158 mL/min, suggesting active tubular secretion in addition to glomerular filtration. Approximately 97% of the avibactam dose is recovered in the urine, 95% within 12 h. Less than 1% of ceftazidime is excreted via the bile and less than 0.25% of avibactam is excreted into faeces.
Linearity/non-linearity: The pharmacokinetics of both ceftazidime and avibactam are approximately linear across the dose range studied (0.05 g to 2 g) for a single intravenous administration. No appreciable accumulation of ceftazidime or avibactam was observed following multiple intravenous infusions of 2 g/0.5 g of ceftazidime/avibactam administered every 8 hours for up to 11 days in healthy adults with normal renal function.
Special populations: Renal impairment: Elimination of ceftazidime and avibactam is decreased in patients with moderate or severe renal impairment. The average increases in avibactam AUC are 3.8-fold and 7-fold in subjects with moderate and severe renal impairment, see Dosage & Administration.
Hepatic impairment: Mild to moderate hepatic impairment had no effect on the pharmacokinetics of ceftazidime in individuals administered 2 g intravenously every 8 hours for 5 days, provided renal function was not impaired. The pharmacokinetics of ceftazidime in patients with severe hepatic impairment has not been established. The pharmacokinetics of avibactam in patients with any degree of hepatic impairment has not been studied.
As ceftazidime and avibactam do not appear to undergo significant hepatic metabolism, the systemic clearance of either active substance is not expected to be significantly altered by hepatic impairment.
Elderly patients (≥65 years): Reduced clearance of ceftazidime was observed in elderly patients, which was primarily due to age-related decrease in renal clearance of ceftazidime. The mean elimination half-life of ceftazidime ranged from 3.5 to 4 hours following intravenous bolus dosing with 2 g every 12 hours in elderly patients 80 years or older.
Following a single dose intravenous administration of 500 mg avibactam as a 30-minute IV infusion, the elderly had a slower terminal half-life of avibactam, which may be attributed to age related decrease in renal clearance.
Paediatric population: The pharmacokinetics of ceftazidime and avibactam were evaluated in paediatric patients from 3 months to < 18 years of age with suspected or confirmed infections following a single dose of ceftazidime 50 mg/kg and avibactam 12.5 mg/kg for patients weighing < 40 kg or Zavicefta 2 g/0.5 g (ceftazidime 2 grams and avibactam 0.5 grams) for patients weighing ≥ 40 kg. Plasma concentrations of ceftazidime and avibactam were similar across all four age cohorts in the study (3 months to < 2 years, 2 to < 6 years, 6 to < 12 years, and 12 to < 18 years). Ceftazidime and avibactam AUC0-t and Cmax values in the two older cohorts (paediatric patients from 6 to < 18 years), which had more extensive pharmacokinetic sampling, were similar to those observed in healthy adult subjects with normal renal function that received Zavicefta 2 g/0.5 g. Data from this study and the two Phase 2 paediatric studies in patients with cIAI and cUTI were pooled with PK data from adults (Phase 1 to Phase 3) to update the population PK model, which was used to conduct simulations to assess PK/PD target attainment. Results from these simulations demonstrated that the recommended dose regimens for paediatric patients with cIAI, cUTI and HAP/VAP, including dose adjustments for patients with renal impairment, result in systemic exposure and PK/PD target attainment values that are similar to those in adults at the approved Zavicefta dose of 2 g/0.5 g administered over 2 hours, every 8 hours.
There is limited experience with the use of ceftazidime plus avibactam in the paediatric groups of 3 months to < 6 months. The recommended dosing regimens are based on simulations conducted using the final population PK models. Simulations demonstrated that the recommended dose regimens result in comparable exposures to other age groups with PK/PD target attainment > 90%. Based on data from the completed paediatric clinical trials, at the recommended dose regimens, there was no evidence of over or under exposure in the subjects aged 3 months to < 6 months.
In addition, there is very limited data in paediatric patients aged 3 months to < 2 years with impaired renal function (CrCL ≤ 50 mL/min/1.73 m2), with no data in severe renal impairment from the completed paediatric clinical trials. Population PK models for ceftazidime and avibactam were used to conduct simulations for patients with impaired renal function.
Gender and race: The pharmacokinetics of ceftazidime/avibactam is not significantly affected by gender or race.
Toxicology: Preclinical safety data: Ceftazidime: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, reproduction toxicity or genotoxicity. Carcinogenicity studies have not been conducted with ceftazidime.
Avibactam: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity or genotoxicity. Carcinogenicity studies have not been conducted with avibactam.
Reproduction toxicity: In pregnant rabbits administered avibactam at 300 and 1000 mg/kg/day, there was a dose-related lower mean foetal weight and delayed ossification, potentially related to maternal toxicity. Plasma exposure levels at maternal and foetal NOAEL (100 mg/kg/day) indicate moderate to low margins of safety.
In the rat, no adverse effects were observed on embryofetal development or fertility. Following administration of avibactam throughout pregnancy and lactation in the rat, there was no effect on pup survival, growth or development, however there was an increase in incidence of dilation of the renal pelvis and ureters in less than 10% of the rat pups at maternal exposures greater than or equal to approximately 1.5 times human therapeutic exposures.