Piracetam may be taken with or without food. The film-coated tablets should be swallowed with liquid.
Route of Administration: For oral use.
Adults: Symptomatic treatment of psycho-organic syndromes: The recommended daily dose ranges from 2.4 g up to 4.8 g, in two or three sub-doses.
Treatment of myoclonus of cortical origin: The daily dosage should begin at 7.2 g, increasing by 4.8 g every three or four days up to a maximum of 20 g, in two or three divided doses. Treatment with other anti-myoclonic medicinal products should be maintained at the same dosage. Depending on the clinical benefit obtained, the dosage of other such medicinal products should be reduced, if possible. The dosage must be set individually for each patient by a therapeutic trial.
Once started, treatment with piracetam should be continued for as long as the original cerebral disease persists. In patients with an acute episode, spontaneous evolution may occur over time and an attempt should be made every 6 months to decrease or discontinue the medicinal treatment. This should be done by reducing the dose of piracetam by 1.2 g every two days (every three or four days in the case of a Lance-Adams syndrome, in order to prevent the possibility of sudden relapse or withdrawal seizures).
Treatment of vertigo: The recommended daily dose ranges from 2.4 g to 4.8 g, in two or three divided doses.
Prophylaxis and remission of sickle cell vaso-occlusive crises: The recommended daily dose for prophylaxis is 160 mg/kg, orally, in four divided doses.
The recommended daily dose for remission is 300 mg/kg intravenously, in four divided doses.
For sickle cell anaemia the prophylactic dosage must be permanent.
A dose lower than 160 mg/kg/day or irregular intake may result in relapse of crises.
Children: Dyslexia: The recommended dosage for school age children (from 8 years old) and adolescents is 3.2 g per day, that means 2 tablets of 800 mg in the morning and in the evening, usually during the whole period of the school year.
Prophylaxis and remission of sickle cell vaso-occlusive crises: For children from 3 years old onwards the prophylactic dosage is 160 mg/kg/per day divided into 4 divided doses. In case of remission a dose of 300 mg/kg/day is administered intravenously, divided into 4 divided doses. The prophylactic administration in sickle cell anaemia must be permanent.
A dose lower than 160 mg/kg/per day or an irregular intake may cause a relapse of the illness. Piracetam is administered to children with sickle cell anaemia indication in recommended daily doses (mg/kg - see previous text). Piracetam has been administered only to a limited number of children in the age range of 1-3 years.
Elderly: Adjustment of the dose is recommended in elderly patients with compromised renal function (see Renal impairment under Precautions).
For long term treatment in the elderly, regular evaluation of the creatinine clearance is required to allow dosage adaptation if needed.
Renal impairment: Piracetam is contraindicated in severe renal impairment (renal creatinine clearance of less than 20 ml per minute) (see Contraindications and Precautions).
The daily dose must be individualised according to renal function. Refer to the following table and adjust the dose as indicated. To use this dosing table, an estimate of the patient's creatinine clearance (Clcr) in ml/min is needed. The Clcr in ml/min may be estimated from serum creatinine (mg/dl) determination using the following formula: See equation and table.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Hepatic impairment:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Hepatic impairment: No dose adjustment is needed in patients with solely hepatic impairment. In patients with hepatic impairment and renal impairment, adjustment of dose is recommended (see dose adjustment in Renal impairment as previously mentioned).


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image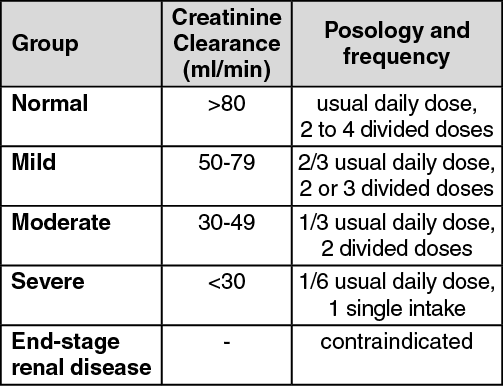 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Đăng xuất
Đăng xuất
