The usual course of therapy is seven days (range 5 to 10 days).
Film-coated tablet: ZINNAT should be taken after food for optimum absorption.
Adults: (See Table 3).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Sequential Therapy: Pneumonia: 1.5 g
ZINACEF three times a day or twice a day (intravenous (i.v.) or intramuscular (i.m)) for 48 to 72 hours, followed by
ZINNAT (cefuroxime axetil) oral therapy 500 mg twice a day for 7 to 10 days.
Acute exacerbations of chronic bronchitis: 750 mg
ZINACEF three times a day or twice a day (i.v. or i.m.) for 48 to 72 hours, followed by
ZINNAT (cefuroxime axetil) oral therapy 500 mg twice a day for 5 to 10 days.
Duration of both parenteral and oral therapy is determined by the severity of the infection and the clinical status of the patient.
Children aged ≥ 3 months and up to 12 years: (See Table 4.)
Click on icon to see table/diagram/image
ZINNAT tablets should not be crushed and are therefore unsuitable for treatment of patients, such as younger children, who cannot swallow tablets. In children
ZINNAT oral suspension may be used.
There is no experience of using
ZINNAT in children under the age of 3 months.
Oral suspension: For optimal absorption,
ZINNAT should be taken with food.
Adults: (See Table 5.)
Click on icon to see table/diagram/image
Children 3 month-12 years: When prescription of a fixed dose is preferred, the recommended dose for most infections is 125 mg twice daily. In children aged two years or older with otitis media or where appropriate, with more severe infections, the dose is 250 mg twice daily, to a maximum of 500 mg daily.
There are no clinical trial data available on the use of ZINNAT in children under the age of 3 months.
In infants and children, it may be preferable to adjust dosage according to weight or age. The dose in infants and children 3 months to 12 years is 10 mg/kg twice daily for most infections, to a maximum of 250 mg daily. In otitis media or more severe infections the recommended dose is 15 mg/kg twice daily to a maximum of 500 mg daily.
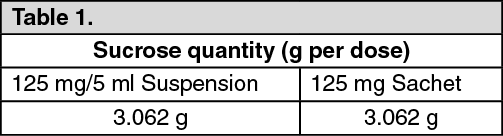
The following two tables, divided by age group and weight, serve as a guideline for simplified administration from measuring spoons (5 ml) for the 125 mg/5 ml multi-dose suspension, and 125 mg single dose sachets. (See Tables 6 and 7.)
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
To enhance compliance and improve the dosing accuracy in very young children, a dosing syringe can be supplied with a multidose bottle containing 50 ml of suspension. However, dosing in spoonfuls should be considered a more favourable option if the child is able to take the medication from the spoon.
If required, the dosing syringe may also be used in older children (refer to the dosing tables as follows).
The recommended doses for the paediatric dosing syringe are expressed in ml or mg and according to body weight in Tables 8 and 9.
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
ZINNAT is also available as the
sodium salt
(ZINACEF) for parenteral
administration. This permits parenteral therapy with
ZINNAT to be followed by oral therapy in situations where a change
from parenteral to oral treatment is clinically indicated.
Film-coated tablet & oral suspension: Renal impairment: Cefuroxime is primarily excreted by the kidneys. In patients with markedly impaired renal function it is recommended that the dosage of cefuroxime be reduced to compensate for its slower excretion. (See Table 10.)
Click on icon to see table/diagram/image



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image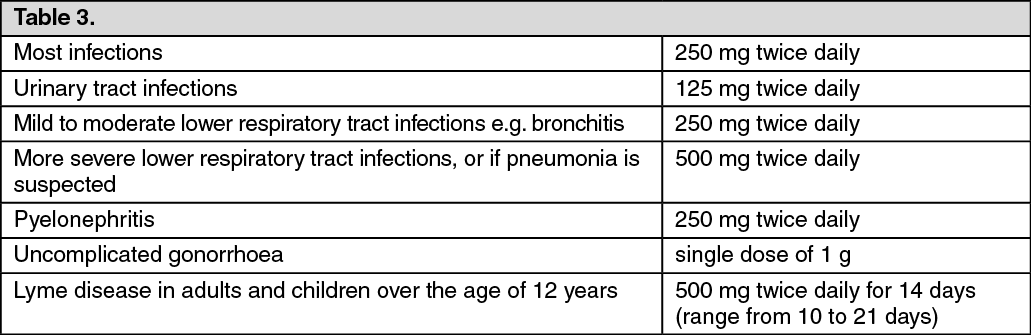 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image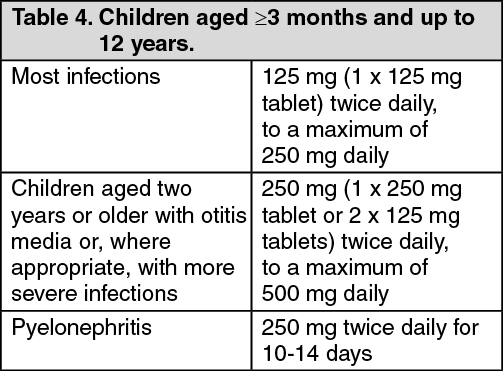 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Đăng xuất
Đăng xuất
