


 Sign Out
Sign Out
Bleeding is the most common reaction reported both in clinical studies as well as in post-marketing experience where it was mostly reported during the first month of treatment.
In CAPRIE, in patients treated with either clopidogrel or ASA, the overall incidence of any bleeding was 9.3%. The incidence of severe cases was 1.4% for clopidogrel and 1.6% for ASA.
In CURE, the major bleeding event rate for clopidogrel + ASA was dose-dependent on ASA (<100mg: 2.6%; 100-200mg: 3.5%; >200mg: 4.9%) as was the major bleeding event rate for placebo + ASA (<100mg: 2.0%; 100-200mg: 2.3%; >200mg: 4.0%). The risk of bleeding (life-threatening, major, minor, other) decreased during the course of the trial: 0-1 months (clopidogrel: 9.6%; placebo: 6.6%), 1-3 months (clopidogrel: 4.5%; placebo: 2.3%), 3-6 months (clopidogrel: 3.8%; placebo: 1.6%), 6-9 months (clopidogrel: 3.2%; placebo: 1.5%), 9-12 months (clopidogrel: 1.9%; placebo: 1.0%). There was no excess in major bleeds with clopidogrel + ASA within 7 days after coronary bypass graft surgery in patients who stopped therapy more than five days prior to surgery (4.4% clopidogrel + ASA vs. 5.3% placebo + ASA). In patients who remained on therapy within five days of bypass graft surgery, the event rate was 9.6% for clopidogrel + ASA, and 6.3% for placebo + ASA.
In CLARITY, there was an overall increase in bleeding in the clopidogrel + ASA group (17.4%) vs. the placebo + ASA group (12.9%). The incidence of major bleeding was similar between groups (1.3% versus 1.1% for the clopidogrel + ASA and the placebo + ASA groups, respectively). This was consistent across subgroups of patients defined by baseline characteristics, and type of fibrinolytic or heparin therapy.
In COMMIT, the overall rate of noncerebral major bleeding or cerebral bleeding was low and similar in both groups (0.6% versus 0.5% in the clopidogrel + ASA and the placebo + ASA groups, respectively).
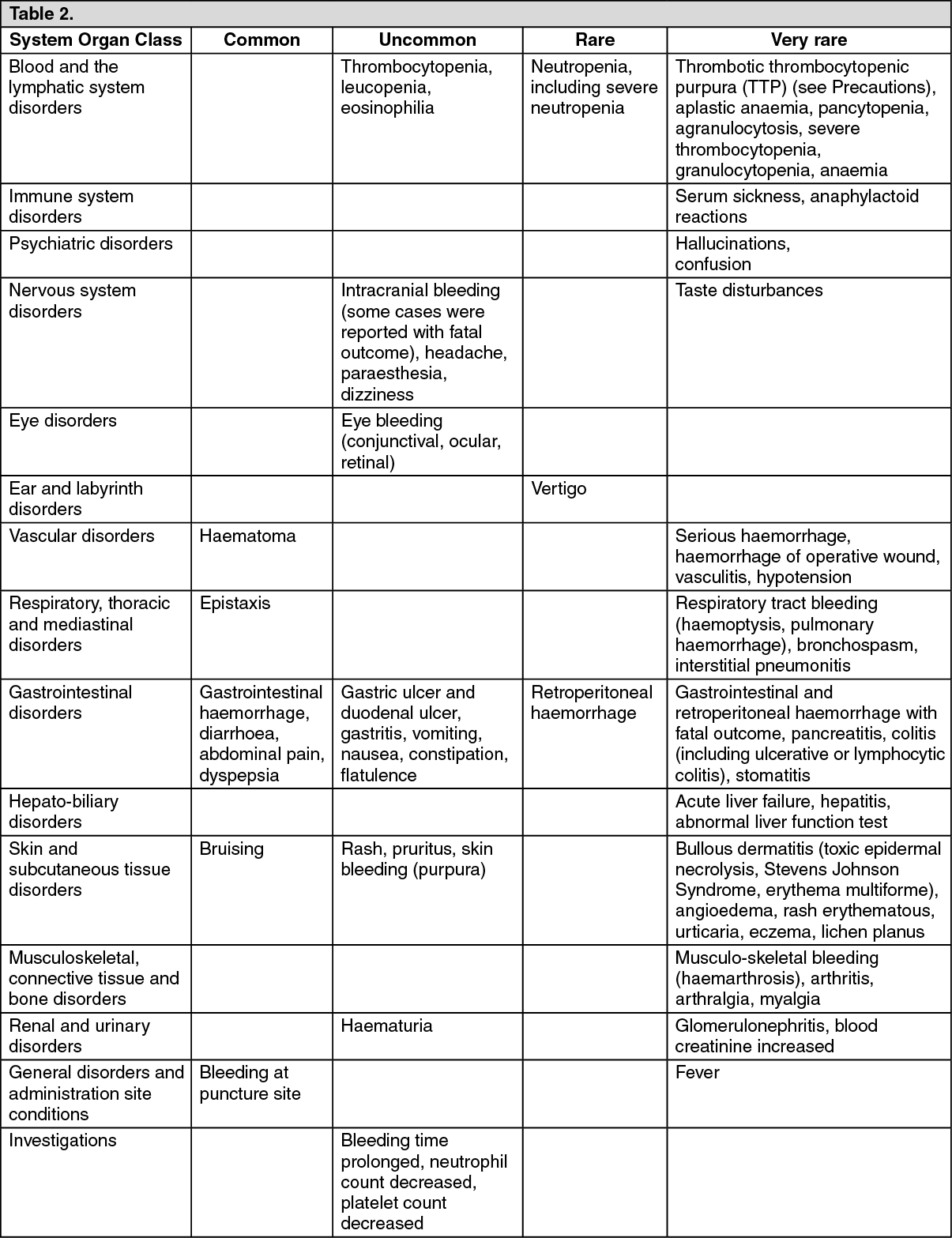
Adverse reactions that occurred either during clinical studies or that were spontaneously reported are presented in the table below. Their frequency is defined using the following conventions: common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000). Within each system organ class, adverse drug reactions are presented in order of decreasing seriousness. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form