


 Sign Out
Sign Out
Pharmacology: Pharmacodynamics: Clopidogrel is a prodrug, one of whose metabolites is an inhibitor of platelet aggregation. Clopidogrel must be metabolised by CYP450 enzymes to produce the active metabolite that inhibits platelet aggregation. The active metabolite of clopidogrel selectively inhibits the binding of adenosine diphosphate (ADP) to its platelet P2Y12 receptor, and the subsequent ADP-mediated activation of the glycoprotein GPIIb/IIIa complex, thereby inhibiting platelet aggregation. Due to the irreversible binding, platelets exposed are affected for the remainder of their lifespan (approximately 7-10 days) and recovery of normal platelet function occurs at a rate consistent with platelet turnover. Platelet aggregation induced by agonists other than ADP is also inhibited by blocking the amplification of platelet activation by released ADP.
Because the active metabolite is formed by CYP450 enzymes, some of which are polymorphic or subject to inhibition by other drugs, not all patients will have adequate platelet inhibition.
Repeated doses of 75 mg per day produced substantial inhibition of ADP-induced platelet aggregation from the first day; this increased progressively and reached steady state between Day 3 and Day 7. At steady state, the average inhibition level observed with a dose of 75 mg per day was between 40% and 60%. Platelet aggregation and bleeding time gradually returned to baseline values, generally within 5 days after treatment was discontinued.
The safety and efficacy of clopidogrel have been evaluated in 4 double-blind studies involving over 80,000 patients: the CAPRIE study, a comparison of clopidogrel to ASA, and the CURE, CLARITY and COMMIT studies comparing clopidogrel to placebo, both medicinal products given in combination with ASA and other standard therapy.
Recent myocardial infarction (MI), recent stroke or established peripheral arterial disease: The CAPRIE study included 19,185 patients with atherothrombosis as manifested by recent myocardial infarction (<35 days), recent ischaemic stroke (between 7 days and 6 months) or established peripheral arterial disease (PAD). Patients were randomised to clopidogrel 75 mg/day or ASA 325 mg/day, and were followed for 1 to 3 years. In the myocardial infarction subgroup, most of the patients received ASA for the first few days following the acute myocardial infarction.
Clopidogrel significantly reduced the incidence of new ischaemic events (combined end point of myocardial infarction, ischaemic stroke and vascular death) when compared to ASA. In the intention to treat analysis, 939 events were observed in the clopidogrel group and 1,020 events with ASA (relative risk reduction (RRR) 8.7%, [95% CI: 0.2 to 16.4]; p = 0.045), which corresponds, for every 1,000 patients treated for 2 years, to 10 [CI: 0 to 20] additional patients being prevented from experiencing a new ischaemic event. Analysis of total mortality as a secondary endpoint did not show any significant difference between clopidogrel (5.8%) and ASA (6.0%).
In a subgroup analysis by qualifying condition (myocardial infarction, ischaemic stroke, and PAD) the benefit appeared to be strongest (achieving statistical significance at p = 0.003) in patients enrolled due to PAD (especially those who also had a history of myocardial infarction) (RRR = 23.7%; CI: 8.9 to 36.2) and weaker (not significantly different from ASA) in stroke patients (RRR = 7.3%; CI: -5.7 to 18.7 [p=0.258]). In patients who were enrolled in the trial on the sole basis of a recent myocardial infarction, clopidogrel was numerically inferior, but not statistically different from ASA (RRR = -4.0%; CI: -22.5 to 11.7 [p=0.639]). In addition, a subgroup analysis by age suggested that the benefit of clopidogrel in patients over 75 years was less than that observed in patients ≤ 75 years.
Since the CAPRIE trial was not powered to evaluate efficacy of individual subgroups, it is not clear whether the differences in relative risk reduction across qualifying conditions are real, or a result of chance.
Acute coronary syndrome: The CURE study included 12,562 patients with non-ST segment elevation acute coronary syndrome (unstable angina or non-Q-wave myocardial infarction), and presenting within 24 hours of onset of the most recent episode of chest pain or symptoms consistent with ischaemia. Patients were required to have either ECG changes compatible with new ischaemia or elevated cardiac enzymes or troponin I or T to at least twice the upper limit of normal. Patients were randomised to clopidogrel (300 mg loading dose followed by 75 mg/day, N=6,259) or placebo (N=6,303), both given in combination with ASA (75-325 mg once daily) and other standard therapies. Patients were treated for up to one year. In CURE, 823 (6.6%) patients received concomitant GPIIb/IIIa receptor antagonist therapy. Heparins were administered in more than 90% of the patients and the relative rate of bleeding between clopidogrel and placebo was not significantly affected by the concomitant heparin therapy.
The number of patients experiencing the primary endpoint [cardiovascular (CV) death, myocardial infarction (MI), or stroke] was 582 (9.3%) in the clopidogrel-treated group and 719 (11.4%) in the placebo-treated group, a 20% relative risk reduction (95% CI of 10%-28%; p=0.00009) for the clopidogrel-treated group (17% relative risk reduction when patients were treated conservatively, 29% when they underwent percutaneous transluminal coronary angioplasty (PTCA) with or without stent and 10% when they underwent coronary artery bypass graft (CABG)). New cardiovascular events (primary endpoint) were prevented, with relative risk reductions of 22% (CI: 8.6, 33.4), 32% (CI: 12.8, 46.4), 4% (CI: -26.9, 26.7), 6% (CI: -33.5, 34.3) and 14% (CI: -31.6, 44.2), during the 0-1, 1-3, 3-6, 6-9 and 9-12 month study intervals, respectively. Thus, beyond 3 months of treatment, the benefit observed in the clopidogrel + ASA group was not further increased, whereas the risk of haemorrhage persisted (see Precautions).
The use of clopidogrel in CURE was associated with a decrease in the need of thrombolytic therapy (RRR = 43.3%; CI: 24.3%, 57.5%) and GPIIb/IIIa inhibitors (RRR = 18.2%; CI: 6.5%, 28.3%).
The number of patients experiencing the co-primary endpoint (CV death, MI, stroke or refractory ischaemia) was 1,035 (16.5%) in the clopidogrel-treated group and 1,187 (18.8%) in the placebo-treated group, a 14% relative risk reduction (95% CI of 6%-21%, p=0.0005) for the clopidogrel-treated group. This benefit was mostly driven by the statistically significant reduction in the incidence of MI [287 (4.6%) in the clopidogrel treated group and 363 (5.8%) in the placebo treated group]. There was no observed effect on the rate of rehospitalisation for unstable angina.
The results obtained in populations with different characteristics (e.g. unstable angina or non-Q-wave MI, low to high risk levels, diabetes, need for revascularisation, age, gender, etc) were consistent with the results of the primary analysis. In particular, in a post-hoc analysis in 2,172 patients (17% of the total CURE population) who underwent stent placement (Stent-CURE), the data showed that clopidogrel compared to placebo, demonstrated a significant RRR of 26.2% favouring clopidogrel for the co-primary endpoint (CV death, MI, stroke) and also a significant RRR of 23.9% for the second co-primary endpoint (CV death, MI, stroke or refractory ischaemia). Moreover, the safety profile of clopidogrel in this subgroup of patients did not raise any particular concern. Thus, the results from this subset are in line with the overall trial results.
The benefits observed with clopidogrel were independent of other acute and long-term cardiovascular therapies (such as heparin/LMWH, GPIIb/IIIa antagonists, lipid lowering medicinal products, beta blockers, and ACE-inhibitors). The efficacy of clopidogrel was observed independently of the dose of ASA (75-325 mg once daily).
In patients with acute ST-segment elevation MI, safety and efficacy of clopidogrel have been evaluated in 2 randomised, placebo-controlled, double-blind studies, CLARITY and COMMIT.
The CLARITY trial included 3,491 patients presenting within 12 hours of the onset of a ST elevation MI and planned for thrombolytic therapy. Patients received clopidogrel (300 mg loading dose, followed by 75 mg/day, n=1,752) or placebo (n=1,739), both in combination with ASA (150 to 325 mg as a loading dose, followed by 75 to 162 mg/day), a fibrinolytic agent and, when appropriate, heparin. The patients were followed for 30 days. The primary endpoint was the occurrence of the composite of an occluded infarct-related artery on the predischarge angiogram, or death or recurrent MI before coronary angiography. For patients who did not undergo angiography, the primary endpoint was death or recurrent myocardial infarction by Day 8 or by hospital discharge. The patient population included 19.7% women and 29.2% patients ≥ 65 years. A total of 99.7% of patients received fibrinolytics (fibrin specific: 68.7%, non-fibrin specific: 31.1%), 89.5% heparin, 78.7% beta blockers, 54.7% ACE inhibitors and 63% statins.
Fifteen percent (15.0%) of patients in the clopidogrel group and 21.7% in the placebo group reached the primary endpoint, representing an absolute reduction of 6.7% and a 36% odds reduction in favour of clopidogrel (95% CI: 24, 47%; p < 0.001), mainly related to a reduction in occluded infarct-related arteries. This benefit was consistent across all prespecified subgroups including patients' age and gender, infarct location, and type of fibrinolytic or heparin used.
The 2x2 factorial design COMMIT trial included 45,852 patients presenting within 24 hours of the onset of the symptoms of suspected MI with supporting ECG abnormalities (i.e. ST elevation, ST depression or left bundle-branch block). Patients received clopidogrel (75 mg/day, n=22,961) or placebo (n=22,891), in combination with ASA (162 mg/day), for 28 days or until hospital discharge. The co-primary endpoints were death from any cause and the first occurrence of re-infarction, stroke or death. The population included 27.8% women, 58.4% patients ≥ 60 years (26% ≥70 years) and 54.5% patients who received fibrinolytics.
Clopidogrel significantly reduced the relative risk of death from any cause by 7% (p=0.029), and the relative risk of the combination of re-infarction, stroke or death by 9% (p=0.002), representing an absolute reduction of 0.5% and 0.9%, respectively. This benefit was consistent across age, gender and with or without fibrinolytics, and was observed as early as 24 hours.
Pharmacokinetics: Absorption: After single and repeated oral doses of 75 mg per day, clopidogrel is rapidly absorbed. Mean peak plasma levels of unchanged clopidogrel (approximately 2.2-2.5 ng/ml after a single 75 mg oral dose) occurred approximately 45 minutes after dosing. Absorption is at least 50%, based on urinary excretion of clopidogrel metabolites.
Distribution: Clopidogrel and the main circulating (inactive) metabolite bind reversibly in vitro to human plasma proteins (98% and 94% respectively). The binding is non-saturable in vitro over a wide concentration range.
Metabolism: Clopidogrel is extensively metabolised by the liver. In vitro and in vivo, clopidogrel is metabolised according to two main metabolic pathways: one mediated by esterases and leading to hydrolysis into its inactive carboxylic acid derivative (85% of circulating metabolites), and one mediated by multiple cytochromes P450. Clopidogrel is first metabolised to a 2-oxo-clopidogrel intermediate metabolite. Subsequent metabolism of the 2-oxo-clopidogrel intermediate metabolite results in formation of the active metabolite, a thiol derivative of clopidogrel. In vitro, this metabolic pathway is mediated by CYP3A4, CYP2C19, CYP1A2 and CYP2B6. The active thiol metabolite which has been isolated in vitro, binds rapidly and irreversibly to platelet receptors, thus inhibiting platelet aggregation.
Elimination: Following an oral dose of 14C-labelled clopidogrel in man, approximately 50% was excreted in the urine and approximately 46% in the faeces in the 120-hour interval after dosing. After a single oral dose of 75 mg, clopidogrel has a half-life of approximately 6 hours. The elimination half-life of the main circulating (inactive) metabolite was 8 hours after single and repeated administration.
Pharmacogenetics: Several polymorphic CYP450 enzymes activate clopidogrel. CYP2C19 is involved in the formation of both the active metabolite and the 2-oxo-clopidogrel intermediate metabolite. Clopidogrel active metabolite pharmacokinetics and antiplatelet effects, as measured by ex vivo platelet aggregation assays, differ according to CYP2C19 genotype. The CYP2C19*1 allele corresponds to fully functional metabolism while the CYP2C19*2 and CYP2C19*3 alleles correspond to reduced metabolism. The CYP2C19*2 and CYP2C19*3 alleles account for 85% of reduced function alleles in whites and 99% in Asians. Other alleles associated with reduced metabolism include CYP2C19*4, *5, *6, *7 and *8, but these are less frequent in the general population. Published frequencies for the common CYP2C19 phenotypes and genotypes are listed in the table as follows. (See Table 1.)
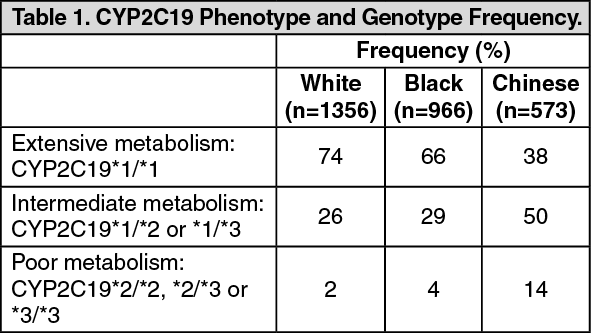 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTo date, the impact of CYP2C19 genotype on the pharmacokinetics of the active metabolite of clopidogrel has been evaluated in 227 subjects from 7 reported studies. Reduced CYP2C19 metabolism in intermediate and poor metabolisers decreased the Cmax and AUC of the active metabolite by 30-50% following 300- or 600-mg loading doses and 75-mg maintenance doses. Lower active metabolite exposure results in less platelet inhibition or higher residual platelet reactivity. To date, diminished antiplatelet responses to clopidogrel have been described for intermediate and poor metabolisers in 21 reported studies involving 4,520 subjects. The relative difference in antiplatelet response between genotype groups varies across studies depending on the method used to evaluate response, but is typically greater than 30%.
The association between CYP2C19 genotype and clopidogrel treatment outcome was evaluated in 2 post hoc clinical trial analyses (substudies of CLARITY [n=465] and TRITON-TIMI 38 [n=1,477]) and 5 cohort studies (total n=6,489). In CLARITY and one of the cohort studies (n=765; Trenk), cardiovascular event rates did not differ significantly by genotype. In TRITON-TIMI 38 and 3 of the cohort studies (n=3,516; Collet, Sibbing, Giusti), patients with an impaired metaboliser status (intermediate and poor combined) had a higher rate of cardiovascular events (death, myocardial infarction, and stroke) or stent thrombosis compared to extensive metabolisers. In the fifth cohort study (n=2,208; Simon), the increased event rate was observed only in poor metabolisers.
Pharmacogenetic testing can identify genotypes associated with variability in CYP2C19 activity.
There may be genetic variants of other CYP450 enzymes with effects on the ability to form the active metabolite of clopidogrel.
Special populations: The pharmacokinetics of the active metabolite of clopidogrel is not known in these special populations.
Renal impairment: After repeated doses of 75 mg clopidogrel per day, in subjects with severe renal disease (creatinine clearance from 5 to 15 ml/min) inhibition of ADP-induced platelet aggregation was lower (25%) than that observed in healthy subjects, however, the prolongation of bleeding time was similar to that seen in healthy subjects receiving 75 mg of clopidogrel per day. In addition, clinical tolerance was good in all patients.
Hepatic impairment: After repeated doses of 75 mg clopidogrel per day for 10 days in patients with severe hepatic impairment, inhibition of ADP-induced platelet aggregation was similar to that observed in healthy subjects. The mean bleeding time prolongation was also similar in the two groups.
Race: The prevalence of CYP2C19 alleles that result in intermediate and poor CYP2C19 metabolism differs according to race/ethnicity (see Pharmacogenetics previously mentioned). From literature, limited data in Asian populations are available to assess the clinical implication of genotyping of this CYP on clinical outcome events.
Toxicology: Preclinical safety data: During non clinical studies in rat and baboon, the most frequently observed effects were liver changes. These occurred at doses representing at least 25 times the exposure seen in humans receiving the clinical dose of 75 mg/day and were a consequence of an effect on hepatic metabolising enzymes. No effect on hepatic metabolising enzymes was observed in humans receiving clopidogrel at the therapeutic dose.
At very high doses, a poor gastric tolerability (gastritis, gastric erosions and/or vomiting) of clopidogrel was also reported in rat and baboon.
There was no evidence of carcinogenic effect when clopidogrel was administered for 78 weeks to mice and 104 weeks to rats when given at doses up to 77 mg/kg per day (representing at least 25 times the exposure seen in humans receiving the clinical dose of 75 mg/day).
Clopidogrel has been tested in a range of in vitro and in vivo genotoxicity studies, and showed no genotoxic activity.
Clopidogrel was found to have no effect on the fertility of male and female rats and was not teratogenic in either rats or rabbits. When given no lactating rats, clopidogrel caused a slight delay in the development of the offspring. Specific pharmacokinetic studies performed with radiolabelled clopidogrel have shown that the parent compound or its metabolites are excreted in the milk. Consequently, a direct effect (slight toxicity), or an indirect effect (low palatability) cannot be excluded.