


 Sign Out
Sign Out


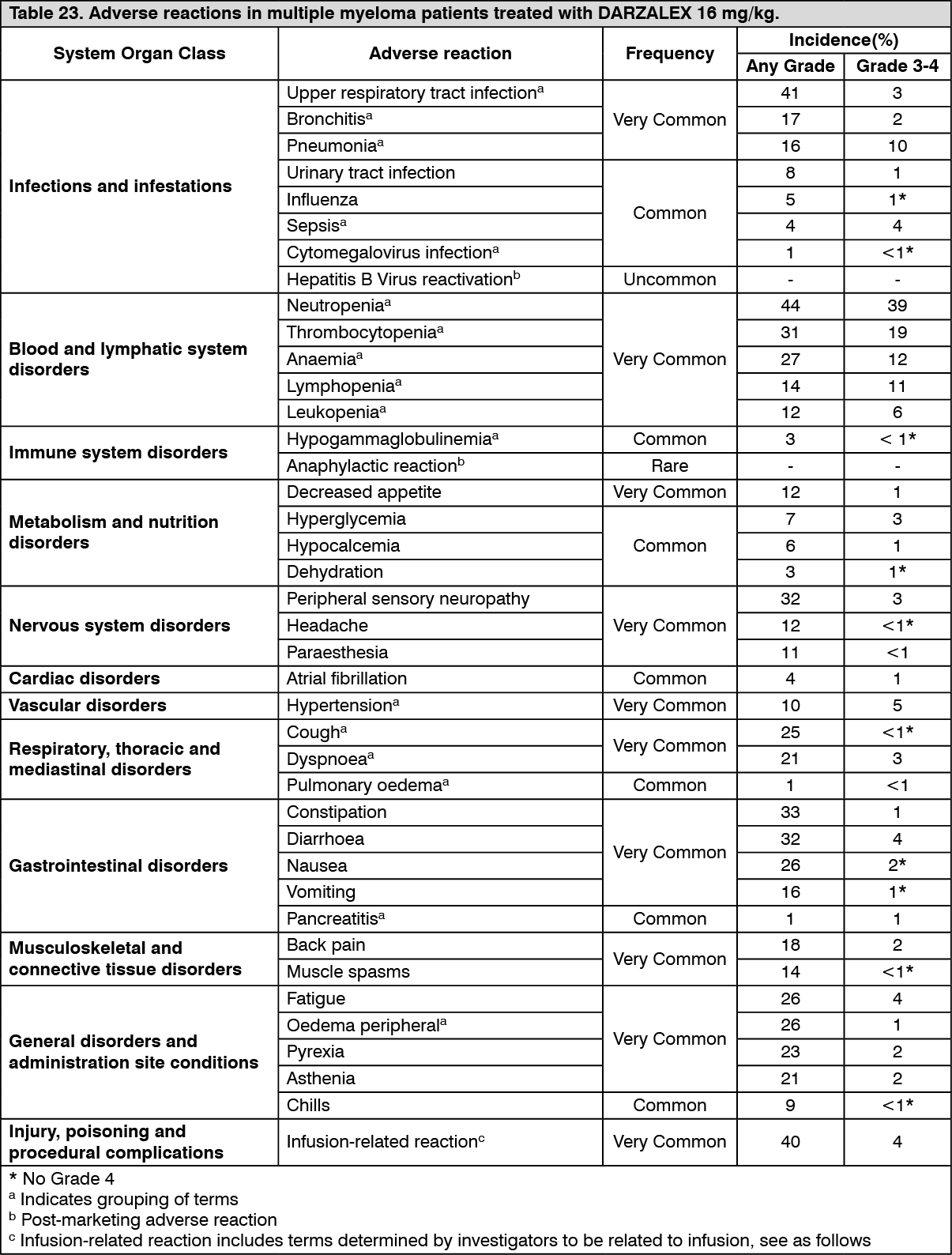
Tabulated list of adverse reactions: Table 23 summarises the adverse reactions that occurred in patients receiving DARZALEX. The data reflects exposure to DARZALEX (16 mg/kg) in 2066 patients with multiple myeloma including 1910 patients who received DARZALEX in combination with background regimens and 156 patients who received DARZALEX as monotherapy. Post-marketing adverse reactions are also included.
In Study MMY3006, the number of CD34+ cell yield was numerically lower in the D-VTd arm compared with the VTd arm (Median: D-VTd: 6.3 x 106/kg; VTd 8.9 x 106/kg) and among those who completed mobilisation, more patients in the D-VTd group received plerixafor compared to those in the VTd arm (D-VTd: 21.7%; VTd: 7.9%). The rates of engraftment and haematopoietic reconstitution was similar among the transplanted subjects in the D-VTd and VTd arms (D-VTd: 99.8%; VTd: 99.6%; as measured by the recovery of neutrophils > 0.5 x 109/L, leukocytes > 1.0 x 109/L, and platelets > 50 x 109/L without transfusion).
Frequencies are defined as very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000) and very rare (<1/10,000). Within each frequency grouping, where relevant, adverse reactions are presented in order of decreasing seriousness. (See Table 23.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Infusion-related reactions (IRRs): In clinical studies (monotherapy and combination treatments; N = 2066) the incidence of any grade IRRs was 37% with the first (16 mg/kg, Week 1) infusion of DARZALEX, 2% with the Week 2 infusion, and cumulatively 6% with subsequent infusions. Less than 1% of patients had a Grade 3/4 IRR with the Week 2 or subsequent infusions.
The median time to onset of a reaction was 1.5 hours (range: 0 to 72.8 hours). The incidence of infusion modifications due to reactions was 36%. Median durations of 16 mg/kg infusions for the 1st Week, 2nd Week and subsequent infusions were approximately 7, 4 and 3 hours respectively.
Severe IRRs included bronchospasm, dyspnoea, laryngeal oedema, pulmonary oedema, hypoxia, and hypertension. Other adverse IRRs included nasal congestion, cough, chills, throat irritation, vomiting and nausea (see Precautions).
When DARZALEX dosing was interrupted in the setting of ASCT (Study MMY3006) for a median of 3.75 (range: 2.4; 6.9) months, upon re-initiation of DARZALEX the incidence of IRRs was 11% at first infusion following ASCT. Infusion rate/dilution volume used upon re-initiation was that used for the last DARZALEX infusion prior to interruption due to ASCT. IRRs occurring at re-initiation of DARZALEX following ASCT were consistent in terms of symptoms and severity (Grade 3/4: <1%) with those reported in previous studies at Week 2 or subsequent infusions.
In Study MMY1001, patients receiving daratumumab combination treatment (n=97) were administered the first 16 mg/kg daratumumab dose at Week 1 split over two days i.e. 8 mg/kg on Day 1 and Day 2 respectively. The incidence of any grade IRRs was 42%, with 36% of patients experiencing IRRs on Day 1 of Week 1, 4% on Day 2 of Week 1, and 8% with subsequent infusions. The median time to onset of a reaction was 1.8 hours (range: 0.1 to 5.4 hours). The incidence of infusion interruptions due to reactions was 30%. Median durations of infusions were 4.2 h for Week 1-Day 1, 4.2 h for Week 1-Day 2, and 3.4 hours for the subsequent infusions.
Infections: In patients receiving DARZALEX combination therapy, Grade 3 or 4 infections were reported as follows: Relapsed/refractory patient studies: DVd: 21%, Vd: 19%; DRd: 27%, Rd: 23%; DPd: 28%.
Newly diagnosed patient studies: D‑VMP: 23%, VMP: 15%; DRd: 32%, Rd: 23%; D-VTd: 22%, VTd: 20%.
Pneumonia was the most commonly reported severe (Grade 3 or 4) infection across studies. In active controlled studies, discontinuations from treatment due to infections occurred in 1-4% of patients. Fatal infections were primarily due to pneumonia and sepsis.
In patients receiving DARZALEX combination therapy, fatal infections (Grade 5) were reported as follows: Relapsed/refractory patient studies: DVd: 1%, Vd: 2%; DRd: 2%, Rd: 1%; DPd: 2%.
Newly diagnosed patient studies: D-VMP: 1%, VMP: 1%; DRd: 2%, Rd: 2%; DVTd: 0%, VTd: 0%.
Key: D=daratumumab; Vd=bortezomib-dexamethasone; Rd=lenalidomide-dexamethasone; Pd=pomalidomide-dexamethasone; VMP=bortezomib-melphalan-prednisone; VTd=bortezomib-thalidomide-dexamethasone.
Haemolysis: There is a theoretical risk of haemolysis. Continuous monitoring for this safety signal will be performed in clinical studies and post-marketing safety data.
Other special populations: In the Phase III study MMY3007, which compared treatment with D-VMP to treatment with VMP in patients with newly diagnosed multiple myeloma who are ineligible for autologous stem cell transplant, safety analysis of the subgroup of patients with an ECOG performance score of 2 (D-VMP: n=89, VMP: n=84), was consistent with the overall population (see Pharmacology: Pharmacodynamics under Actions).
Elderly patients: Of the 2459 patients who received DARZALEX at the recommended dose, 38% were 65 to 75 years of age, and 15% were 75 years of age or older. No overall differences in effectiveness were observed based on age. The incidence of serious adverse reactions was higher in older than in younger patients. Among patients with relapsed and refractory multiple myeloma (n=1213), the most common serious adverse reactions that occurred more frequently in elderly (≥65 years of age) were pneumonia and sepsis. Among patients with newly diagnosed multiple myeloma who are ineligible for autologous stem cell transplant (n=710), the most common serious adverse reaction that occurred more frequently in elderly (≥75 years of age) was pneumonia.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
Solution for SC injection: Summary of the safety profile: The most frequent adverse reactions of any grade (≥ 20% patients) with daratumumab (either intravenous or subcutaneous formulations) when administered either as monotherapy or combination treatment were IRRs, fatigue, nausea, diarrhoea, constipation, pyrexia, cough, neutropenia, thrombocytopenia, anaemia, oedema peripheral, peripheral sensory neuropathy and upper respiratory tract infection. Serious adverse reactions were pneumonia, bronchitis, upper respiratory tract infection, sepsis, pulmonary oedema, influenza, pyrexia, dehydration, diarrhoea, atrial fibrillation and syncope.
The safety profile of the DARZALEX subcutaneous formulation was similar to that of intravenous formulation with the exception of a lower rate of IRRs. In the phase III study MMY3012, neutropenia was the only adverse reaction reported at ≥ 5% higher frequency for DARZALEX subcutaneous formulation compared to intravenous daratumumab (grade 3 or 4: 13% vs 8%, respectively).
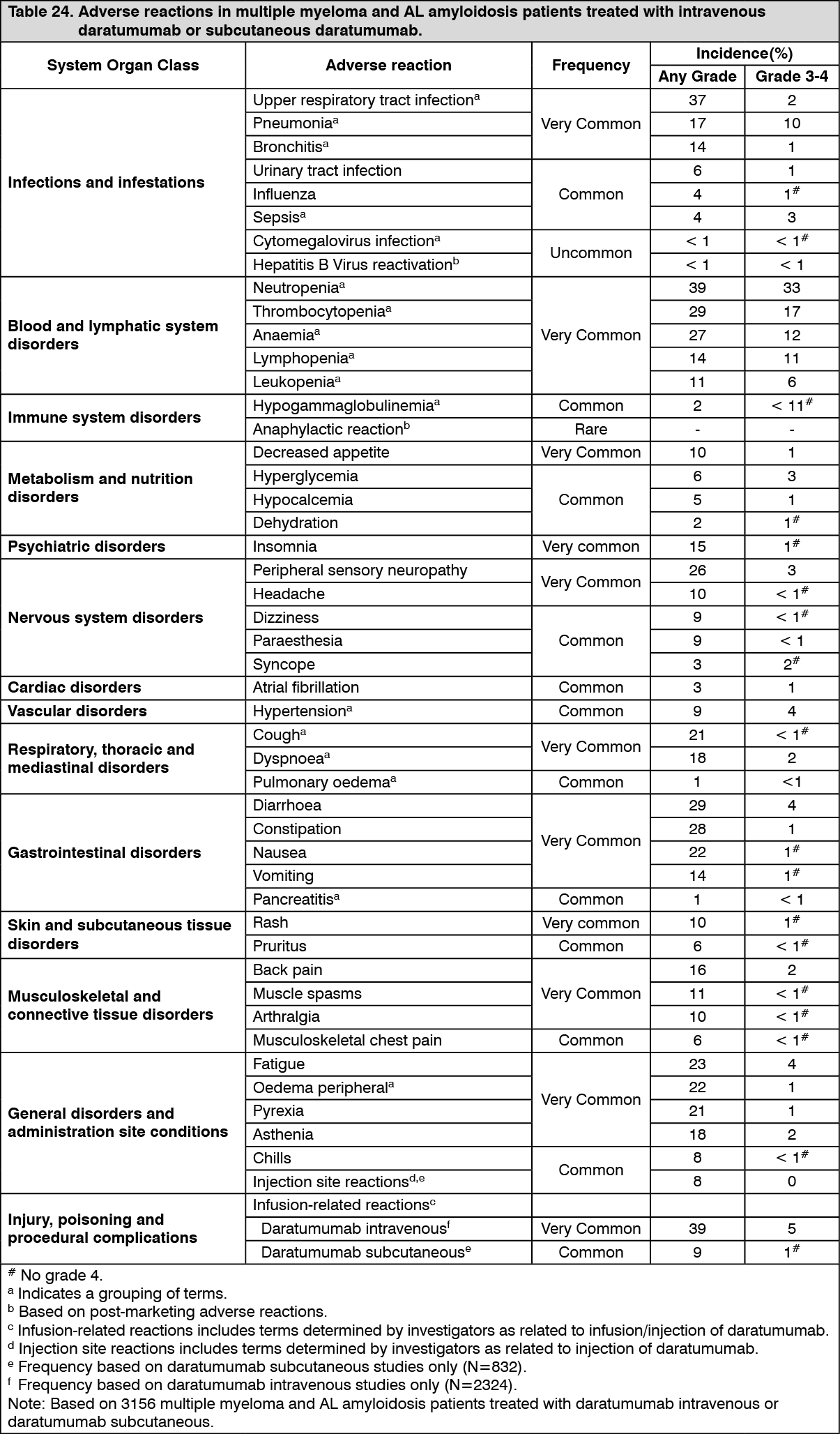
Tabulated list of adverse reactions: Table 24 summarises the adverse reactions that occurred in patients receiving DARZALEX subcutaneous formulation or intravenous formulation of daratumumab.
The data reflects exposure to DARZALEX subcutaneous formulation (1800 mg) in 639 patients with multiple myeloma (MM). The data includes 260 patients from a phase III active-controlled study (MMY3012) who received DARZALEX solution for subcutaneous injection as monotherapy and 149 patients from a phase III active-controlled study (MMY3013) who received DARZALEX subcutaneous formulation in combination with pomalidomide and dexamethasone (D-Pd). The data also reflects three open-label, clinical studies in which patients received DARZALEX solution for subcutaneous injection either as monotherapy (N=31, MMY1004 and MMY1008) and MMY2040 in which patients received DARZALEX solution for subcutaneous injection in combination with either bortezomib, melphalan and prednisone (D-VMP, n=67), lenalidomide and dexamethasone (D-Rd, n=65) or bortezomib, lenalidomide and dexamethasone (D-VRd, n=67). Additionally, data reflect exposure to 193 patients with newly diagnosed AL amyloidosis from a phase III active-controlled study (AMY3001) in which patients received DARZALEX subcutaneous formulation in combination with bortezomib, cyclophosphamide and dexamethasone (D-VCd).
The safety data also reflects exposure to intravenous daratumumab (16 mg/kg) in 2324 patients with multiple myeloma including 1910 patients who received intravenous daratumumab in combination with background regimens and 414 patients who received intravenous daratumumab as monotherapy. Post-marketing adverse reactions are also included.
Frequencies are defined as very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1000 to < 1/100), rare (≥ 1/10000 to < 1/1000) and very rare (< 1/10000). Within each frequency grouping, adverse reactions are presented in the order of decreasing seriousness. (See Table 24.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Infusion-related reactions (IRRs): In clinical studies (monotherapy and combination treatments; N=832) with DARZALEX subcutaneous formulation, the incidence of any grade IRRs was 8.2% with the first injection of DARZALEX (1800 mg, week 1), 0.4% with the week 2 injection, and 1.1% with subsequent injections. Grade 3 IRRs were seen in 0.8% of patients. No patients had grade 4 IRRs.
Signs and symptoms of IRR may include respiratory symptoms, such as nasal congestion, cough, throat irritation, allergic rhinitis, wheezing as well as pyrexia, chest pain, pruritis, chills, vomiting, nausea, and hypotension. Severe reactions have occurred, including bronchospasm, hypoxia, dyspnoea, hypertension and tachycardia (see Precautions).
Injection site reactions (ISRs): In clinical studies (N=832) with DARZALEX subcutaneous formulation, the incidence of any grade injection site reaction was 7.7%. There were no grade 3 or 4 ISRs. The most common (> 1%) ISR at the site of injection was erythema.
Infections: In patients with multiple myeloma receiving daratumumab as monotherapy, the overall incidence of infections was similar between DARZALEX subcutaneous formulation (52.9%) versus intravenous daratumumab groups (50.0%). Grade 3 or 4 infections also occurred at similar frequencies between DARZALEX subcutaneous formulation (11.7%) and intravenous daratumumab (14.3%). Most infections were manageable and rarely led to treatment discontinuation. Pneumonia was the most commonly reported grade 3 or 4 infection across studies. In active-controlled studies, discontinuations from treatment due to infections occurred in 1-4% of patients. Fatal infections were primarily due to pneumonia and sepsis.
In patients with multiple myeloma receiving intravenous daratumumab combination therapy, the following were reported: Grade 3 or 4 infections: Relapsed/refractory patient studies: DVd: 21%, Vd: 19%; DRd: 28%, Rd: 23%; DPd: 28%.
Newly diagnosed patient studies: D-VMP: 23%, VMP: 15%; DRd: 32%, Rd: 23%; D-VTd: 22%, VTd: 20%.
Grade 5 (fatal) infections: Relapsed/refractory patient studies: DVd: 1%, Vd: 2%; DRd: 2%, Rd: 1%; DPd: 2%.
Newly diagnosed patient studies: D-VMP: 1%, VMP: 1%; DRd: 2%, Rd: 2%; DVTd: 0%, VTd: 0%.
In patients with multiple myeloma receiving DARZALEX subcutaneous formulation combination therapy, the following were reported: Grade 3 or 4 infections: DPd: 28%, Pd: 23%.
Grade 5 (fatal) infections: DPd: 5%, Pd: 3%.
Key: D=daratumumab; Vd=bortezomib-dexamethasone; Rd=lenalidomide-dexamethasone; Pd=pomalidomide-dexamethasone; VMP=bortezomib-melphalan-prednisone; VTd=bortezomib-thalidomide-dexamethasone.
In patients with AL amyloidosis receiving DARZALEX subcutaneous formulation combination therapy, the following were reported: Grade 3 or 4 infections: D-VCd: 17%, VCd:10%.
Grade 5 infections: D-VCd: 1%, VCd: 1%.
Key: D=daratumumab; VCd=bortezomib-cyclophosphamide-dexamethasone.
Haemolysis: There is a theoretical risk of haemolysis. Continuous monitoring for this safety signal will be performed in clinical studies and post-marketing safety data.
Cardiac disorders and AL amyloidosis-related cardiomyopathy: The majority of patients in AMY3001 had AL amyloidosis-related cardiomyopathy at baseline (D-VCd 72% vs. VCd 71%). Grade 3 or 4 cardiac disorders occurred in 11% of D-VCd patients compared to 10% of VCd patients, while serious cardiac disorders occurred in 16% vs. 13% of D-VCd and VCd patients, respectively. Serious cardiac disorders occurring in ≥ 2% of patients included cardiac failure (D-VCd 6.2% vs. VCd 4.3%), cardiac arrest (D-VCd 3.6% vs. VCd 1.6%) and atrial fibrillation (D-VCd 2.1% vs. VCd 1.1%). All D-VCd patients who experienced serious or fatal cardiac disorders had AL amyloidosis-related cardiomyopathy at baseline. The longer median duration of treatment in the D-VCd arm compared to the VCd arm (9.6 months vs. 5.3 months, respectively) should be taken into consideration when comparing the frequency of cardiac disorders between the two treatment groups. Exposure-adjusted incidence rates (number of patients with the event per 100 patient-months at risk) of overall grade 3 or 4 cardiac disorders (1.2 vs. 2.3), cardiac failure (0.5 vs. 0.6), cardiac arrest (0.1 vs. 0.0) and atrial fibrillation (0.2 vs. 0.1) were comparable in the D-VCd arm vs. the VCd arm, respectively.
With a median follow-up of 11.4 months, overall deaths (D-VCd 14% vs. VCd 15%) in study AMY3001 were primarily due to AL amyloidosis-related cardiomyopathy in both treatment arms.
Other special populations: In the phase III study MMY3007, which compared treatment with D-VMP to treatment with VMP in patients with newly diagnosed multiple myeloma who are ineligible for autologous stem cell transplant, safety analysis of the subgroup of patients with an ECOG performance score of 2 (D-VMP: n=89, VMP: n=84), was consistent with the overall population (see Pharmacology: Pharmacodynamics under Actions).
Elderly patients: Of the 3549 patients who received daratumumab (n=832 subcutaneous; n=2717 intravenous) at the recommended dose, 38% were 65 to less than 75 years of age, and 16% were 75 years of age or older. No overall differences in effectiveness were observed based on age. The incidence of serious adverse reactions was higher in older than in younger patients. Among patients with relapsed and refractory multiple myeloma (n=1976), the most common serious adverse reactions that occurred more frequently in elderly (≥ 65 years of age) were pneumonia and sepsis. Among patients with newly diagnosed multiple myeloma who are ineligible for autologous stem cell transplant (n=777), the most common serious adverse reaction that occurred more frequently in elderly (≥ 75 years of age) was pneumonia. Among patients with newly diagnosed AL amyloidosis (n=193), the most common serious adverse reaction that occurred more frequently in elderly (≥ 65 years of age) was pneumonia.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
View ADR Monitoring Form