


 Sign Out
Sign Out

The most severe adverse reaction reported with dolutegravir was a hypersensitivity reaction that included rash and severe liver effects (see Precautions).
Tabulated list of adverse reactions: The adverse reactions from clinical study and post-marketing experience are listed in Table 3 by body system, organ class and absolute frequency. Frequencies are defined as very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), not known (cannot be estimated from the available data). (See Table 3.)
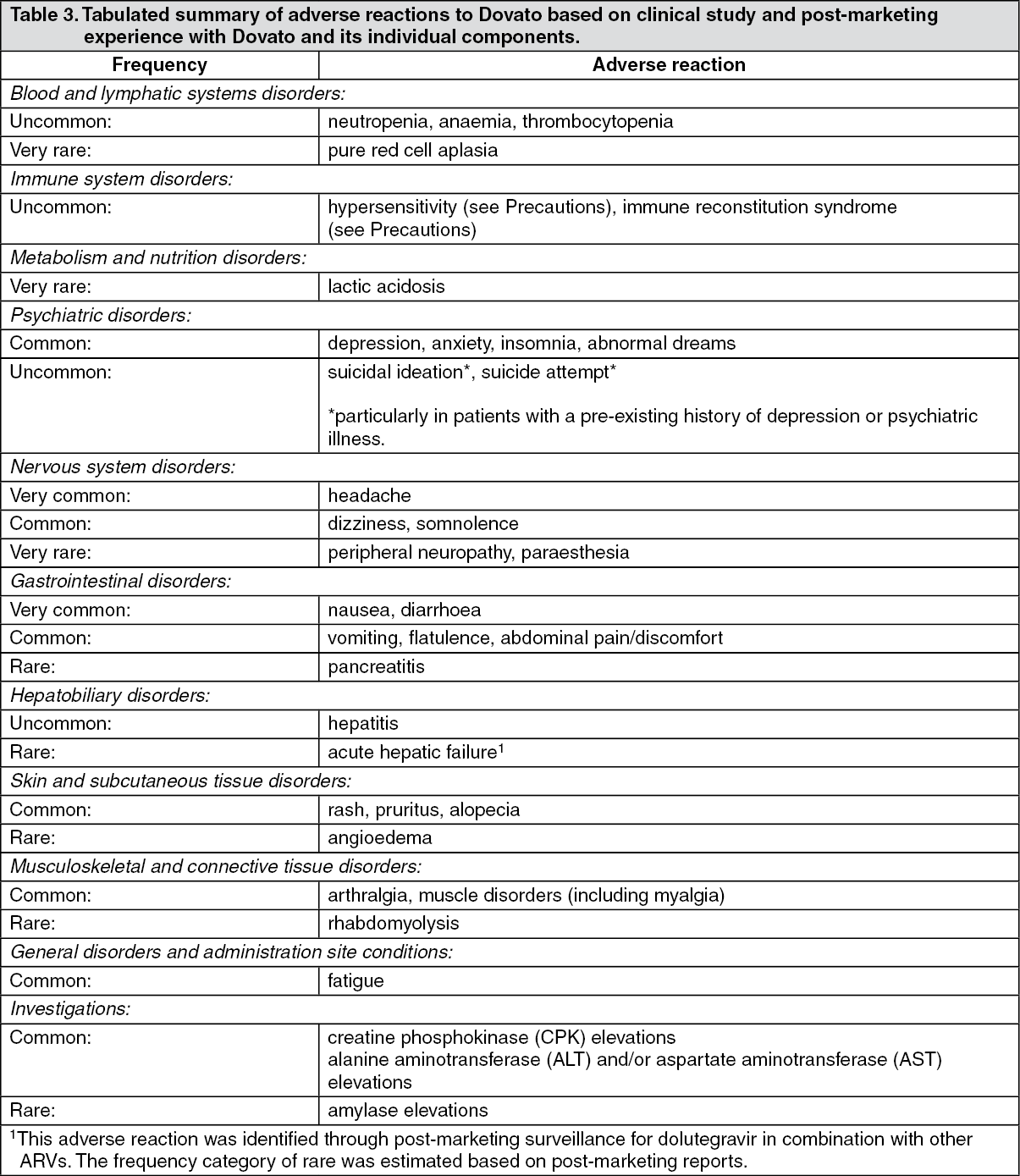 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Changes in laboratory biochemistries: Dolutegravir has been associated with an increase in serum creatinine occurring in the first week of treatment when administered with other antiretroviral medicinal products. Increases in serum creatinine occurred within the first four weeks of treatment with dolutegravir plus lamivudine and remained stable through 48 weeks. In the pooled GEMINI studies a mean change from baseline of 10.3 μmol/L (range: -36.3 μmol/L to 55.7 μmol/L) was observed after 48 weeks of treatment. These changes are linked to the inhibiting effect of dolutegravir on renal tubular transporters of creatinine. The changes are not considered to be clinically relevant and do not reflect a change in glomerular filtration rate.
Co-infection with Hepatitis B or C: In the Phase III studies for the dolutegravir single agent, patients with hepatitis B and/or C co-infection were permitted to enrol provided that baseline liver chemistry tests did not exceed 5 times the upper limit of normal (ULN). Overall, the safety profile in patients co-infected with hepatitis B and/or C was similar to that observed in patients without hepatitis B or C co-infection, although the rates of AST and ALT abnormalities were higher in the subgroup with hepatitis B and/or C co-infection for all treatment groups. Liver chemistry elevations consistent with immune reconstitution syndrome were observed in some subjects with hepatitis B and/or C co-infection at the start of dolutegravir therapy, particularly in those whose anti-hepatitis B therapy was withdrawn (see Precautions).
Metabolic parameters: Weight and levels of blood lipids and glucose may increase during antiretroviral therapy (see Precautions).
Osteonecrosis: Cases of osteonecrosis have been reported, particularly in patients with generally acknowledged risk factors, advanced HIV disease or long-term exposure to CART. The frequency of this is unknown (see Precautions).
Immune response syndrome: In HIV-infected patients with severe immune deficiency at the time of initiation of combination antiretroviral therapy (CART), an inflammatory reaction to asymptomatic or residual opportunistic infections may arise. Autoimmune disorders (such as Graves' disease and autoimmune hepatitis) have also been reported; however, the reported time to onset is more variable and these events can occur many months after initiation of treatment (see Precautions).
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product.
View ADR Monitoring Form