The units of Botulinum Toxin Type A are specific to the preparation and are not interchangeable with other preparations of botulinum toxin.
Botulin um Toxin Type A should only be administered by appropriately trained physicians.
Ipsen can facilitate training in administration of Botulinum Toxin Type A injections.
The exposed central portion of the rubber stopper should be cleaned with alcohol immediately prior to piercing the septum. A sterile 23 or 25 gauge needle should be used.
Arm spasticity: Posology: The recommended dose is 1000 units in total, distributed amongst the following five muscles: (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
The sites of injection should be guided by standard locations used for electromyography, although actual location of the injection site will be determined by palpation. All muscles except the biceps brachii (BB) should be injected at one site, whilst the biceps should be injected at two sites. The maximum dose administered must not exceed 1000 units.
The starting dose should be lowered if there is evidence to suggest that this dose may result in excessive weakness of the target muscles, such as for patients whose target muscles are small, where the BB muscle is not to be injected or for patients who require concomitant injections into other muscle groups. Clinical improvement may be expected within two weeks after injection. Injections may be repeated approximately every 16 weeks, or as required to maintain a response, but not more frequently than every 12 weeks.
Children: The safety and effectiveness of Botulinum Toxin Type A in the treatment of arm spasticity in children have not been demonstrated.
Method of administration: When treating arm spasticity, Botulinum Toxin Type A is reconstituted with 1.0 mL of sodium chloride injection B.P. (0.9%) to yield a solution containing 500 units per mL of botulinum toxin type A.
Botulinum Toxin Type A is administered by intramuscular injection into the five muscles detailed previously when treating arm spasticity.
Paediatric cerebral palsy spasticity: Posology: The initial recommended dose is 20 units/kg body weight given as a divided dose between both calf muscles. If only one calf is affected, a dose of 10 units/kg bodyweight should be used. Consideration should be given to lowering this starting dose if there is evidence to suggest that this dose may result in excessive weakness of the target muscles, such as for patients whose target muscles are small or patients who require concomitant injections to other muscle groups. Following evaluation of response to the starting dose, subsequent treatment may be titrated within the range 10 units/kg and 30 units/kg divided between both legs. The maximum dose administered must not exceed 30 units/kg or 1000 units/patient whichever is the lower. Administration should primarily be targeted to the gastrocnemius, although injections of the soleus and injection of the tibialis posterior should also be considered.
The use of electromyography (EMG) is not routine clinical practice but may assist in identifying the most active muscles.
Clinical improvement may be expected within two weeks after injection. Injections may be repeated approximately every 16 weeks or as required to maintain response, but not more frequently than every 12 weeks.
Method of administration: When treating paediatric cerebral palsy spasticity, Botulinum Toxin Type A is reconstituted with 1.0 mL of sodium chloride injection B.P. (0.9%) to yield a solution containing 500 units per mL of Botulinum Toxin Type A. Botulinum Toxin Type A is administered by intramuscular injection into the calf muscles when treating spasticity.
Spasmodic torticollis: Posology: The doses recommended for torticollis are applicable to adults of all ages providing the adults are of normal weight with no evidence of low neck muscle mass. A reduced dose may be appropriate if the patient is markedly underweight or in the elderly, where reduced muscle mass may exist.
The initial recommended dose for the treatment of spasmodic torticollis is 500 units per patient given as a divided dose and administered to the two or three most active neck muscles.
For rotational torticollis distribute the 500 units by administering 350 units into the splenius capitis muscle, ipsilateral to the direction of the chin/head rotation and 150 units into the sternomastoid muscle, contralateral to the rotation.
For laterocollis, distribute the 500 units by administering 350 units into the ipsilateral splenius capitis muscle and 150 units into the ipsilateral sternomastoid muscle. In cases associated with shoulder elevation the ipsilateral trapezoid or levator scapulae muscles may also require treatment, according to visible hypertrophy of the muscle or electromyographic (EMG) findings. Where injections of three muscles are required, distribute the 500 units as follows, 300 units splenius capitis, 100 units sternomastoid and 100 units to the third muscle.
For retrocollis distribute the 500 units by administering 250 units into each of the splenius capitis muscles. Bilateral splenii injections may increase the risk of neck muscle weakness.
All other forms of torticollis are highly dependent on specialist knowledge and EMG to identify and treat the most active muscles. EMG should be used diagnostically for all complex forms of torticollis, for reassessment after unsuccessful injections in non complex cases, and for guiding injections into deep muscles or in overweight patients with poorly palpable neck muscles.
On subsequent administration, the doses may be adjusted according to the clinical response and side effects observed. Doses within the range of 250-1000 units are recommended, although the higher doses may be accompanied by an increase in side effects, particularly dysphagia. The maximum dose administered must not exceed 1000 units.
The relief of symptoms of torticollis may be expected within a week after the injection. Injections may be repeated approximately every 16 weeks or as required to maintain a response, but not more frequently than every 12 weeks.
Children: The safety and effectiveness of Botulinum Toxin Type A in the treatment of spasmodic torticollis in children have not been demonstrated.
Method of administration: When treating spasmodic torticollis Botulinum Toxin Type A is reconstituted with 1.0 mL of sodium chloride injection B.P. (0.9%) to yield a solution containing 500 units per mL of Botulinum Toxin Type A. Botulinum Toxin Type A is administered by intramuscular injection as previously mentioned when treating spasmodic torticollis.
Blepharospasm and hemifacial spasm: Posology:
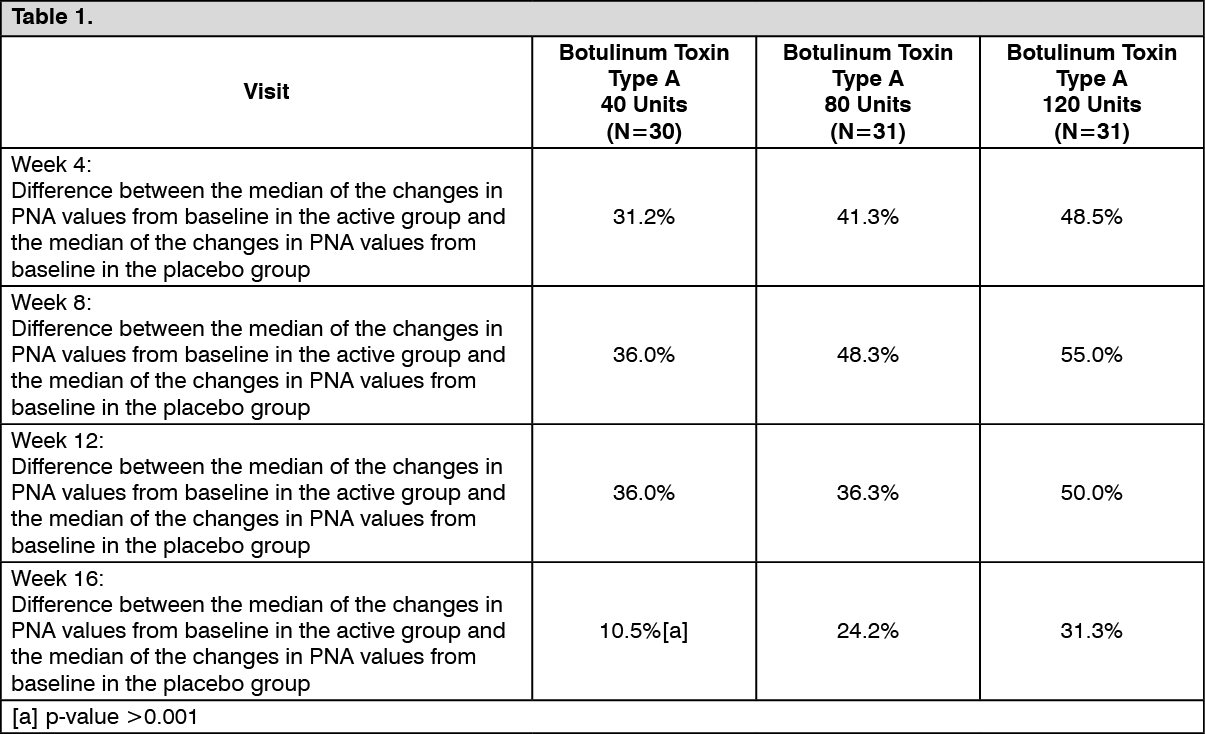
Adults and elderly: In a dose ranging clinical trial on the use of Botulinum Toxin Type A for the treatment of benign essential blepharospasm, a dose of 40 units per eye was significantly effective. Doses of 80 units and 120 units per eye resulted in a longer duration of effect. However, the incidence of related adverse events, specifically ptosis, was dose related. In the treatment of blepharospasm and hemifacial spasm, the maximum dose used must not exceed a total dose of 120 units per eye.
An injection of 10 units (0.05 mL) should be made medially and of 10 units (0.05 mL) should be made laterally into the junction between the preseptal and orbital parts of both the upper and lower orbicularis oculi muscles of each eye. In order to reduce the risk of ptosis, injections near the levator palpebrae superioris should be avoided.
For injections into the upper lid the needle should be directed away from its centre to avoid the levator muscle. A diagram to aid placement of these injections is provided. The relief of symptoms may be expected to begin within two to four days with maximal effect within two weeks.
Injections should be repeated approximately every twelve weeks or as required to prevent recurrence of symptoms but not more frequently than every twelve weeks. On such subsequent administrations, if the response from the initial treatment is considered insufficient, the dose per eye may need to be increased to 60 units: 10 units (0.05 mL) medially and 20 units (0.1 mL) laterally, 80 units: 20 units (0.1 mL) medially and 20 units (0.1 mL) laterally or up to 120 units: 20 units (0.1 mL) medially and 40 units (0.2 mL) laterally above and below each eye in the manner previously described. Additional sites in the frontalis muscle above the brow may also be injected if spasms here interfere with vision.
In cases of unilateral blepharospasm, the injections should be confined to the affected eye. Patients with hemifacial spasm should be treated as for unilateral blepharospasm. The doses recommended are applicable to adults of all ages including the elderly.
Children: The safety and effectiveness of Botulinum Toxin Type A in the treatment of blepharospasm and hemifacial spasm in children have not been demonstrated.
Method of administration: When treating blepharospasm and hemifacial spasm Botulinum Toxin Type A is reconstituted with 2.5 mL of sodium chloride injection BP (0.9%) to yield a solution containing 200 units per mL of Botulinum Toxin Type A. Botulinum Toxin Type A is administered by subcutaneous injection medially and laterally into the junction between the preseptal and orbital parts of both the upper and lower orbicularis oculi muscles of the eyes.
Glabellar Lines: Posology and method of administration: Once reconstituted, Botulinum Toxin Type A should only be used to treat a single patient, during a single session.
Prior to injection, the product is reconstituted with sodium chloride injection BP (0.9% w/v) to yield a solution containing 200 units per mL.
Remove any make-up and disinfect the skin with a local antiseptic.
Intramuscular injections should be performed at right angles to the skin using a sterile 29-30 gauge needle.
The recommended dose is 50 units (0.25 mL of reconstituted solution) of Botulinum Toxin Type A to be divided into 5 injection sites, 10 units (0.05 mL of reconstituted solution) are to be administered intramuscularly into each of the 5 sites: 2 injections into each corrugator muscle and one into the procerus muscle near the nasofrontal angle.
The anatomical landmarks can be more readily identified if observed and palpated at maximal frown. Before injection, place the thumb or index finger firmly below the orbital rim in order to prevent extravasation below the orbital rim. The needle should be pointed upward and medially during the injection. In order to reduce the risk of ptosis, avoid injections near the levator palpebrae superioris muscle, particularly in patients with larger brow-depressor complexes (depressor supercilii). Injections in the corrugator muscle must be made into the central part of that muscle, at least 1 cm above the orbital rim.
The treatment interval depends on the individual patient's response after assessment. In clinical studies, an optimal effect was demonstrated for up to 4 months after injection. Some patients were still responders at 5 months. Treatment interval should not be more frequent than every three months.
In the event of treatment failure or diminished effect following repeat injections, alternative treatment methods should be employed. In case of treatment failure after the first treatment session, the following approaches may be considered: Analysis of the causes of failure e.g. incorrect muscles injected, injection technique and formation of toxin-neutralising antibodies; Re-evaluation of the relevance of treatment with botulinum toxin A.
Use in children: The safety and effectiveness of Botulinum Toxin Type A in treating glabellar lines in individuals under 18 years of age have not been demonstrated.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image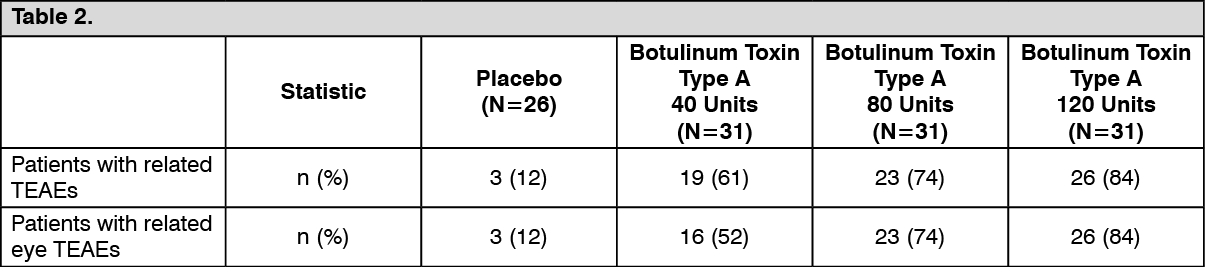 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out