Each tablet contains 50 mg sumatriptan base (as the succinate salt).
Excipients/Inactive Ingredients: Lactose monohydrate, lactose anhydrous, microcrystalline cellulose, croscarmellose sodium, magnesium stearate, Opadry Pink YS-1-1441-G.
Pharmacotherapeutic group: Analgesics: Selective 5-HT1 receptor agonists. ATC code: N02CC01.
Pharmacology: Pharmacodynamics: Sumatriptan has been demonstrated to be a specific and selective 5-hydroxytryptamine1 (5-HT1D) receptor agonist with no effect on other 5-HT receptor (5-HT2-7) subtypes. The vascular 5-HT1D receptor is found predominantly in cranial blood vessels and mediates vasoconstriction. In animals, sumatriptan selectively constricts the carotid arterial circulation but does not alter cerebral blood flow. The carotid arterial circulation supplies blood to the extracranial and intracranial tissues such as the meninges and dilatation of and/or oedema formation in these vessels is thought to be the underlying mechanism of migraine in man.
In addition, evidence from animal studies suggests that sumatriptan inhibits trigeminal nerve activity. Both these actions (cranial vasoconstriction and inhibition of trigeminal nerve activity) may contribute to the anti-migraine action of sumatriptan in humans.
Sumatriptan remains effective in treating menstrual migraine i.e. migraine without aura that occurs between 3 days prior and up to 5 days post onset of menstruation. Sumatriptan should be taken as soon as possible in an attack.
Clinical response begins around 30 minutes following a 100 mg oral dose.
Although the recommended dose of oral IMIGRAN is 50 mg, migraine attacks vary in severity both within and between patients. Doses of 25-100 mg have shown greater efficacy than placebo in clinical trials, but 25 mg is statistically significantly less effective than 50 and 100 mg.
A number of placebo-controlled clinical studies assessed the safety and efficacy of oral sumatriptan standard tablets in over 650 child and adolescent migraineurs aged 10-17 years. These studies failed to demonstrate a statistically significant difference in headache relief at 2 hours between placebo and any sumatriptan dose. The undesirable effects profile of oral sumatriptan in children and adolescents aged 10-17 years was similar to that reported from studies in the adult population.
Pharmacokinetics: Following oral administration, sumatriptan is rapidly absorbed, 70% of maximum concentration occurring at 45 min. After a 100 mg dose, the maximum plasma concentration is 54 ng/ml. Mean absolute oral bioavailability is 14% partly due to pre-systemic metabolism and partly due to incomplete absorption. The elimination phase half-life is approximately 2 hours, although there is an indication of a longer terminal phase. Plasma protein binding is low (14 to 21%), mean volume of distribution is 170 litres. Mean total plasma clearance is approximately 1,160 ml/min and the mean renal plasma clearance is approximately 260 ml/min. Non-renal clearance accounts for about 80% of the total clearance. Sumatriptan is eliminated primarily by oxidative metabolism mediated by monoamine oxidase A.
Special patient populations: Hepatic Impairment: Sumatriptan pharmacokinetics after an oral dose (50 mg) and a subcutaneous dose (6 mg) were studied in 8 patients with mild to moderate hepatic impairment matched for sex, age, and weight with 8 healthy subjects. Following an oral dose, sumatriptan plasma exposure (AUC and Cmax) almost doubled (increased approximately 80%) in patients with mild to moderate hepatic impairment compared to the control subjects with normal hepatic function. There was no difference between the patients with hepatic impairment and control subjects after the s.c. dose. This indicates that mild to moderate hepatic impairment reduces presystemic clearance and increases the bioavailability and exposure to sumatriptan compared to healthy subjects.
Following oral administration, pre-systemic clearance is reduced in patients with mild to moderate hepatic impairment and systemic exposure is almost doubled.
The pharmacokinetics in patients with severe hepatic impairment have not been studied (see Contraindications and Precautions).
The major metabolite, the indole acetic acid analogue of sumatriptan is mainly excreted in the urine, where it is present as a free acid and the glucuronide conjugate. It has no known 5HT1 or 5HT2 activity. Minor metabolites have not been identified. The pharmacokinetics of oral sumatriptan do not appear to be significantly affected by migraine attacks.
In a pilot study, no significant differences were found in the pharmacokinetic parameters between the elderly and young healthy volunteers.
Toxicology: Preclinical Safety Data: Sumatriptan was devoid of genotoxic and carcinogenic activity in in-vitro systems and animal studies.
In a rat fertility study oral doses of sumatriptan resulting in plasma levels approximately 200 times those seen in man after a 100 mg oral dose were associated with a reduction in the success of insemination.
This effect did not occur during a subcutaneous study where maximum plasma levels achieved approximately 150 times those in man by the oral route.
In rabbits embryolethality, without marked teratogenic defects, was seen. The relevance for humans of these findings is unknown.
IMIGRAN tablets are indicated for the acute relief of migraine attacks, with or without aura. IMIGRAN should only be used where there is a clear diagnosis of migraine.
Adults: IMIGRAN is indicated for the acute intermittent treatment of migraine. It should not be used prophylactically. The recommended dose of IMIGRAN should not be exceeded.
It is advisable that IMIGRAN be given as early as possible after the onset of migraine attack but it is equally effective at whatever stage of the attack it is administered.
The recommended dose of oral IMIGRAN is a 50 mg tablet. Some patients may require 100 mg.
If the patient has responded to the first dose but the symptoms recur a second dose may be provided that there is a minimum interval of two hours between the two doses. No more than 300 mg should be taken in any 24 hour period.
Patients who do not respond to the prescribed dose of IMIGRAN should not take a second dose for the same attack. In these cases the attack can be treated with paracetamol, acetylsalicylic acid, or non-steroidal anti-inflammatory drugs. IMIGRAN may be taken for subsequent attacks.
IMIGRAN is recommended as monotherapy for the acute treatment of migraine and should not be given concomitantly with ergotamine or derivatives of ergotamine (including methysergide) (see Contraindications).
The tablets should be swallowed whole with water.
Paediatric population: The efficacy and safety of IMIGRAN in children aged less than 10 years have not been established. No clinical data are available in this age group.
The efficacy and safety of IMIGRAN in children 10 to 17 years of age have not been demonstrated in the clinical trials performed in this age group. Therefore the use of IMIGRAN in children 10 to 17 years of age is not recommended (see Pharmacology: Pharmacodynamics under Actions).
Elderly (Over 65 Years of age): Experience of the use of IMIGRAN in patients aged over 65 years is limited. The pharmacokinetics do not differ significantly from a younger population but until further clinical data are available, the use of IMIGRAN in patients aged over 65 years is not recommended.
Doses in excess of 400 mg orally were not associated with side effects other than those mentioned.
If overdosage occurs, the patient should be monitored for at least ten hours and standard supportive treatment applied as required.
It is unknown what effect haemodialysis or peritoneal dialysis has on the plasma concentrations of IMIGRAN.
Hypersensitivity to sumatriptan or to any of the excipients listed in Description.
Sumatriptan should not be given to patients who have had myocardial infarction or have ischaemic heart disease (IHD), Prinzmetal's angina/coronary vasospasm, peripheral vascular disease or patients who have symptoms or signs consistent with IHD.
Sumatriptan should not be administered to patients with a history of cerebrovascular accident (CVA) or transient ischaemic attack (TIA).
Sumatriptan should not be administered to patients with severe hepatic impairment.
The use of sumatriptan in patients with moderate and severe hypertension and mild uncontrolled hypertension is contraindicated.
The concomitant administration of ergotamine or derivatives of ergotamine (including methysergide) or any triptan/5-hydroxytryptamine1 (5-HT1) receptor agonist with sumatriptan is contraindicated (see Interactions).
Concurrent administration of monoamine oxidase inhibitors (MAOIs) and sumatriptan is contraindicated.
Sumatriptan must not be used within two weeks of discontinuation of therapy with monoamine oxidase inhibitors.
IMIGRAN should only be used where there is a clear diagnosis of migraine.
Sumatriptan is not indicated for use in the management of hemiplegic, basilar or ophthalmoplegic migraine.
Before treating with sumatriptan, care should be taken to exclude potentially serious neurological conditions (e.g. CVA, TIA) if the patient presents with atypical symptoms or if they have not received an appropriate diagnosis for sumatriptan use.
Following administration, sumatriptan can be associated with transient symptoms including chest pain and tightness which may be intense and involve the throat (see Adverse Reactions). Where such symptoms are thought to indicate ischaemic heart disease, no further doses of sumatriptan should be given and appropriate evaluation should be carried out.
Sumatriptan should not be given to patients with risk factors for ischaemic heart disease, including those patients who are heavy smokers or users of nicotine substitution therapies, without prior cardiovascular evaluation (see Contraindications). Special consideration should be given to postmenopausal women and males over 40 with these risk factors. The evaluations however, may not identify every patient who has cardiac disease and, in very rare cases, serious cardiac events have occurred in patients without underlying cardiovascular disease.
Sumatriptan should be administered with caution to patients with mild controlled hypertension, since transient increases in blood pressure and peripheral vascular resistance have been observed in a small proportion of patients (see Contraindications).
There have been rare post-marketing reports describing patients with serotonin syndrome (including altered mental status, autonomic instability and neuromuscular abnormalities) following the use of a selective serotonin reuptake inhibitor (SSRI) and sumatriptan. Serotonin syndrome has been reported following concomitant treatment with triptans and serotonin noradrenaline reuptake inhibitors (SNRIs).
If concomitant treatment with sumatriptan and an SSRI/SNRI is clinically warranted, appropriate observation of the patient is advised (see Interactions).
Sumatriptan should be administered with caution to patients with conditions which may affect significantly the absorption, metabolism or excretion of the drug, e.g. impaired hepatic (Child Pugh grade A or B; see Pharmacology: Pharmacokinetics under Actions) or renal function (see Pharmacology: Pharmacokinetics under Actions). A 50 mg dose should be considered in patients with hepatic impairment.
Sumatriptan should be used with caution in patients with a history of seizures or other risk factors which lower the seizure threshold, as seizures have been reported in association with sumatriptan (see Adverse Reactions).
Patients with known hypersensitivity to sulphonamides may exhibit an allergic reaction following administration of sumatriptan. Reactions may range from cutaneous hypersensitivity to anaphylaxis. Evidence of cross sensitivity is limited, however, caution should be exercised before using sumatriptan in these patients.
Undesirable effects may be more common during concomitant use of triptans and herbal preparations containing St John's Wort (Hypericum perforatum).
Prolonged use of any type of painkiller for headaches can make them worse. If this situation is experienced or suspected, medical advice should be obtained and treatment should be discontinued. The diagnosis of medication overuse headache (MOH) should be suspected in patients who have frequent or daily headaches despite (or because of) the regular use of headache medications.
Patients with rare hereditary problems of galactose intolerance, the Lapp lactase deficiency or glucose-galactose malabsorption should not take this medicine as it contains lactose.
Effects on Ability to Drive and Use Machines: No studies on the effects on the ability to drive and use machines have been performed. Drowsiness may occur as a result of migraine or its treatment with sumatriptan. This may influence the ability to drive and to operate machinery.
Pregnancy: Post-marketing data from the use of sumatriptan during the first trimester in over 1,000 women are available. Although these data contain insufficient information to draw definitive conclusions, they do not point to an increased risk of congenital defects. Experience with the use of sumatriptan in the second and third trimester is limited.
Evaluation of experimental animal studies does not indicate direct teratogenic effects or harmful effects on peri- and postnatal development. However, embryofoetal viability might be affected in the rabbit (see Pharmacology: Toxicology: Preclinical Safety Data under Actions). Administration of sumatriptan should only be considered if the expected benefit to the mother is greater than any possible risk to the foetus.
Lactation: It has been demonstrated that following subcutaneous administration sumatriptan is excreted into breast milk. Infant exposure can be minimised by avoiding breast feeding for 12 hours after treatment, during which time any breast milk expressed should be discarded.
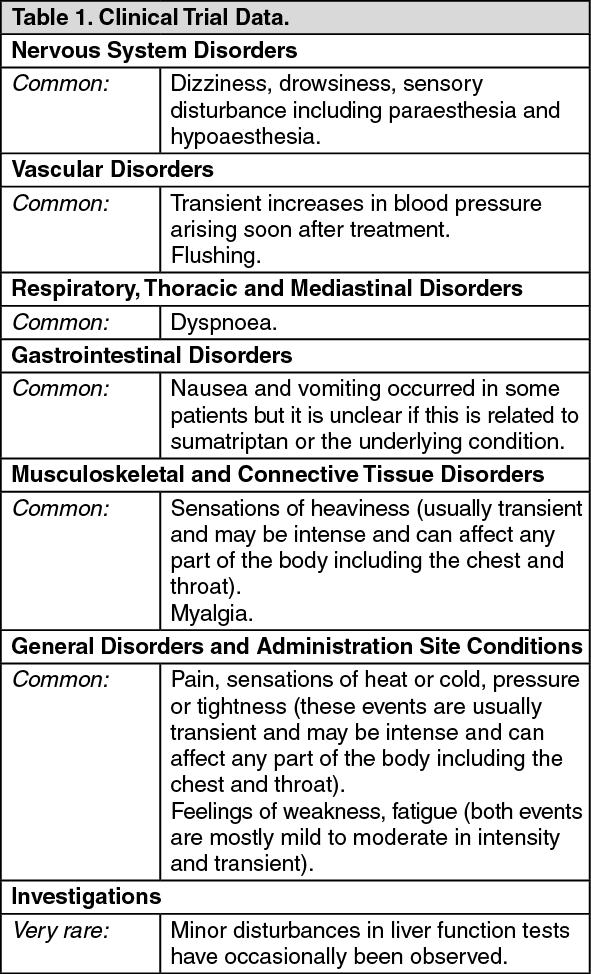
Adverse events are listed below by system organ class and frequency. Frequencies are defined as: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1000 to <1/100), rare (≥1/10,000 to <1/1000), very rare (<1/10,000) and not known (cannot be estimated from the available data). Some of the symptoms reported as undesirable effects may be associated symptoms of migraine. (See Tables 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Studies in healthy subjects show that sumatriptan does not interact with propranolol, flunarizine, pizotifen or alcohol.
There are limited data on an interaction with preparations containing ergotamine or another triptan/5-HT1 receptor agonist. The increased risk of coronary vasospasm is a theoretical possibility and concomitant administration is contraindicated (see Contraindications).
The period of time that should elapse between the use of sumatriptan and ergotamine-containing preparations or another triptan/5-HT1 receptor agonist is not known. This will also depend on the doses and types of products used. The effects may be additive. It is advised to wait at least 24 hours following the use of ergotamine-containing preparations or another triptan/5-HT1 receptor agonist before administering sumatriptan. Conversely, it is advised to wait at least 6 hours following use of sumatriptan before administering an ergotamine-containing product and at least 24 hours before administering another triptan/5-HT1 receptor agonist.
An interaction may occur between sumatriptan and MAOIs and concomitant administration is contra-indicated (see Contraindications).
There have been rare post-marketing reports describing patients with serotonin syndrome (including altered mental status, autonomic instability and neuromuscular abnormalities) following the use of SSRIs and sumatriptan. Serotonin syndrome has also been reported following concomitant treatment with triptans and SNRIs (see Precautions).
N02CC01 - sumatriptan ; Belongs to the class of selective serotonin (5HT1) agonists preparations. Used to relieve migraine.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image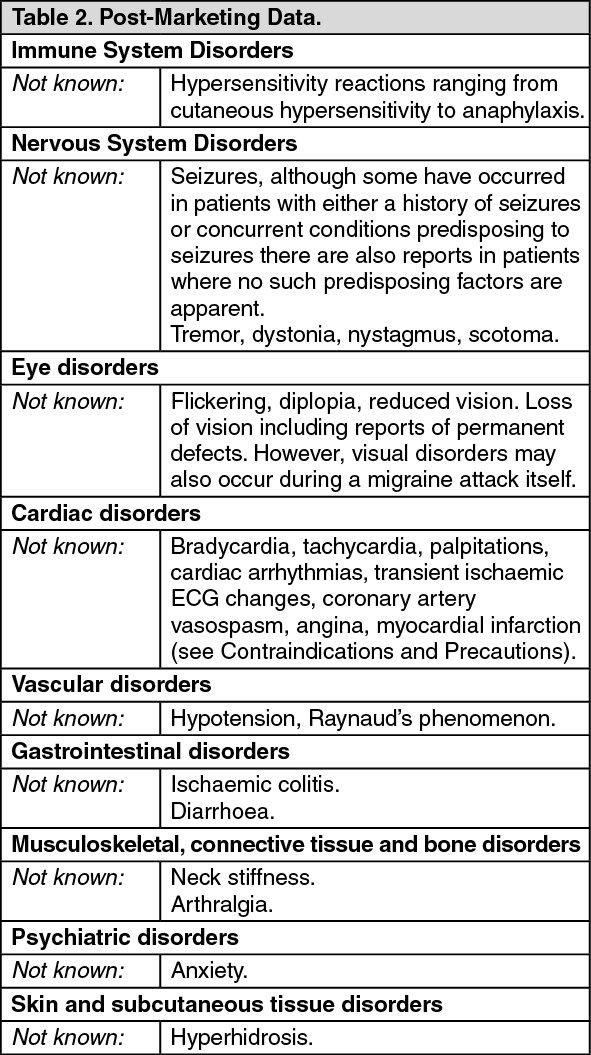 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
