


 Sign Out
Sign Out



General: The dosage of antihyperglycemic therapy with JANUMET should be individualized on the basis of the patient's current regimen, effectiveness, and tolerability while not exceeding the maximum recommended daily dose of 100 mg sitagliptin and 2000 mg metformin.
JANUMET should generally be given twice daily with meals, with gradual dose escalation, to reduce the gastrointestinal (GI) side effects associated with metformin.
Dosing Recommendations: The starting dose of JANUMET should be based on the patient's current regimen. JANUMET should be given twice daily with meals. The following doses are available: 50 mg sitagliptin/500 mg metformin hydrochloride; 50 mg sitagliptin/1000 mg metformin hydrochloride.
As initial therapy: For patients with type 2 diabetes mellitus, whose hyperglycemia is inadequately controlled with diet and exercise alone, the recommended starting dose of JANUMET is 50 mg sitagliptin/500 mg metformin hydrochloride twice daily. Patients may be titrated up to 50 mg sitagliptin/1000 mg metformin hydrochloride twice daily.
For patients inadequately controlled on metformin monotherapy: For patients inadequately controlled on metformin alone, the usual starting dose of JANUMET should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose), plus the dose of metformin already being taken. For patients taking metformin 850 mg twice daily, the recommended starting dose of JANUMET is 50 mg sitagliptin/1000 mg metformin hydrochloride twice daily.
For patients inadequately controlled on sitagliptin monotherapy: For patients inadequately controlled on sitagliptin alone, the usual starting dose of JANUMET is 50 mg sitagliptin/500 mg metformin hydrochloride twice daily. Patients may be titrated up to 50 mg sitagliptin/1000 mg metformin hydrochloride twice daily. Patients taking sitagliptin monotherapy dose-adjusted for renal impairment should not be switched to JANUMET (see Contraindications).
For patients switching from co-administration of sitagliptin and metformin: For patients switching from co-administration of sitagliptin and metformin, JANUMET may be initiated at the dose of sitagliptin and metformin already being taken.
For patients inadequately controlled on dual combination therapy with any two of the following three antihyperglycemic agents: sitagliptin, metformin or a sulfonylurea: The usual starting dose of JANUMET should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose). In determining the starting dose of the metformin component, the patient's level of glycemic control and current dose (if any) of metformin should be considered. Gradual dose escalation to reduce the gastrointestinal (GI) side effects associated with metformin should be considered. Patients currently on or initiating a sulfonylurea may require lower sulfonylurea doses to reduce the risk of sulfonylurea-induced hypoglycemia (see Precautions).
For patients inadequately controlled on dual combination therapy with any two of the following three antihyperglycemic agents: sitagliptin, metformin or a PPAR agonist (i.e. thiazolidinediones): The usual starting dose of JANUMET should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose). In determining the starting dose of the metformin component, the patient's level of glycemic control and current dose (if any) of metformin should be considered. Gradual dose escalation to reduce the gastrointestinal (GI) side effects associated with metformin should be considered.
For patients inadequately controlled on dual combination therapy with any two of the following three antihyperglycemic agents: sitagliptin, metformin or insulin: The usual starting dose of JANUMET should provide sitagliptin dosed as 50 mg twice daily (100 mg total daily dose). In determining the starting dose of the metformin component, the patient's level of glycemic control and current dose (if any) of metformin should be considered. Gradual dose escalation to reduce the gastrointestinal (GI) side effects associated with metformin should be considered. Patients currently on or initiating insulin therapy may require lower doses of insulin to reduce the risk of hypoglycemia (see Precautions).
No studies have been performed specifically examining the safety and efficacy of JANUMET in patients previously treated with other oral antihyperglycemic agents and switched to JANUMET. Any change in therapy of type 2 diabetes should be undertaken with care and appropriate monitoring as changes in glycemic control can occur.
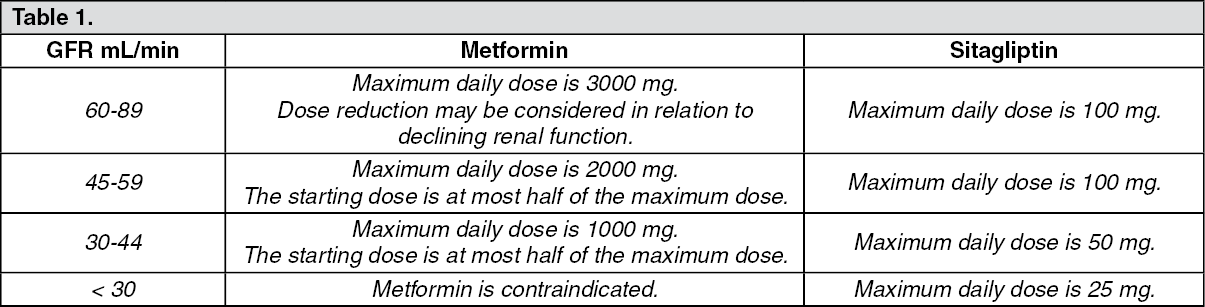
Recommendations for use in renal impairment: No dose adjustment is needed for patients with mild renal impairment (glomerular filtration rate [GFR] ≥ 60 mL/min). A GFR should be assessed before initiation of treatment with metformin-containing products and at least annually thereafter. In patients at increased risk of further progression of renal impairment and in the elderly, renal function should be assessed more frequently, e.g. every 3-6 months.
The maximum daily dose of metformin should preferably be divided into 2-3 daily doses. Factors that may increase the risk of lactic acidosis (see Precautions) should be reviewed before considering initiation of metformin in patients with GFR < 60 mL/min.
JANUMET is contraindicated in patients with GFR < 30 mL/min.
JANUMET is not recommended in patients with a GFR ≥ 30 mL/min and < 45 mL/min because these patients require a lower dosage of sitagliptin than what is available in the fixed combination JANUMET product.
If no adequate strength of Janumet is available, individual monocomponents should be used instead of the fixed-dose combination. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDiscontinuation for iodinated contrast imaging procedures: Intravascular administration of iodinated contrast agents may lead to contrast-induced nephropathy, resulting in metformin accumulation and an increased risk of lactic acidosis. Metformin should be discontinued prior to or at the time of the imaging procedure and not restarted until at least 48 hours after, provided that renal function has been re-evaluated and found to be stable (see Precautions).