In placebo-controlled clinical trials, in patients with type 2 diabetes mellitus, the combination of sitagliptin and metformin was generally well tolerated. The overall incidence of side effects reported in patients receiving the combination of sitagliptin and metformin was similar to that reported in patients receiving the combination of placebo and metformin.
Combination Therapy with Sitagliptin and Metformin: Initial Therapy: In a 24-week placebo-controlled factorial study of initial therapy with sitagliptin 50 mg twice daily in combination with metformin at 500 or 1000 mg twice daily, the drug-related adverse reactions reported in ≥1% of patients receiving combination therapy (and greater than in patients receiving placebo) are shown in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Add-on Combination Therapy to Metformin:
Click on icon to see table/diagram/image
Add-on Combination Therapy to Metformin: In a 24-week placebo-controlled study of sitagliptin added to ongoing metformin therapy, 464 patients on metformin were treated with sitagliptin 100 mg once daily and 237 patients were given placebo with metformin. The only drug-related adverse reaction reported that occurred with an incidence of ≥1% and higher than placebo in patients receiving sitagliptin and metformin was nausea (100 mg sitagliptin and metformin, 1.1%; placebo and metformin, 0.4%).
Hypoglycemia and Gastrointestinal Adverse Experiences: In the placebo-controlled studies of combination therapy with sitagliptin and metformin, the incidence of hypoglycemia (regardless of investigator assessment of causality) reported in patients treated with the combination of sitagliptin and metformin was similar to that reported for patients treated with metformin and placebo. The incidences of pre-specified gastrointestinal adverse experiences in patients treated with the combination of sitagliptin and metformin were similar to those reported for patients treated with metformin alone. (See Table 3.)
Click on icon to see table/diagram/image
In all studies, adverse experiences of hypoglycemia were based on all reports of symptomatic hypoglycemia; a concurrent glucose measurement was not required.
Sitagliptin in Combination with Metformin and a Sulfonylurea: In a 24-week placebo-controlled study of sitagliptin 100 mg daily added to ongoing combination treatment with glimepiride ≥4 mg daily and metformin ≥1500 mg daily, the drug-related adverse reactions reported in ≥1% of patients treated with sitagliptin (N=116) and more commonly than in patients treated with placebo (N=113) were hypoglycemia (sitagliptin, 13.8%; placebo, 0.9%) and constipation (1.7%, 0.0%).
Sitagliptin in Combination with Metformin and a PPARγ Agonist: In a placebo-controlled study of sitagliptin 100 mg daily added to ongoing combination treatment with metformin and rosiglitazone, the drug-related adverse reactions reported through the primary time point at Week 18 in ≥1% of patients treated with sitagliptin (N=170) and more commonly than in patients treated with placebo (N=92) were: headache (sitagliptin, 2.4%; placebo, 0.0%), diarrhea (1.8%, 1.1%), nausea (1.2%, 1.1%), hypoglycemia (1.2%, 0.0%), and vomiting (1.2%, 0.0%). Through Week 54, the drug-related adverse reactions reported in ≥1% of patients treated with sitagliptin and more commonly than in patients treated with placebo were: headache (2.4%, 0.0%), hypoglycemia (2.4%, 0.0%), upper respiratory tract infection (1.8%, 0.0%), nausea (1.2%, 1.1%), cough (1.2%, 0.0%), fungal skin infection (1.2%, 0.0%), peripheral edema (1.2%, 0.0%), and vomiting (1.2%, 0.0%).
Sitagliptin in Combination with Metformin and Insulin: In a 24-week placebo-controlled study of sitagliptin 100 mg added to ongoing combination treatment with metformin ≥1500 mg daily and stable-dose insulin, the only drug-related adverse reaction reported in ≥1% of patients treated with sitagliptin (N=229) and more commonly than in patients treated with placebo (N=233) was hypoglycemia (sitagliptin, 10.9%; placebo, 5.2%). In another 24-week study of patients receiving sitagliptin as add-on therapy while undergoing insulin intensification (with or without metformin), the only drug-related adverse reaction reported in ≥1% in patients treated with sitagliptin and metformin and more commonly than in patients treated with placebo and metformin was vomiting (sitagliptin and metformin, 1.1%; placebo and metformin, 0.4%).
Pancreatitis: In a pooled analysis of 19 double-blind clinical trials that included data from 10,246 patients randomized to receive sitagliptin 100 mg/day (N=5429) or corresponding (active or placebo) control (N=4817), the incidence of non-adjudicated acute pancreatitis events was 0.1 per 100 patient-years in each group (4 patients with an event in 4708 patient-years for sitagliptin and 4 patients with an event in 3942 patient-years for control). See also TECOS Cardiovascular Safety Study as follows. (See JANUMET: Pancreatitis under Precautions.)
With the combination of sitagliptin and metformin, no clinically meaningful changes in vital signs or in ECG (including in QTc interval) were observed.
The most common adverse experience in sitagliptin monotherapy reported regardless of investigator assessment of causality in ≥5% of patients and more commonly than in patients given placebo was nasopharyngitis.
The most common (>5%) established adverse reactions due to initiation of metformin therapy are diarrhea, nausea/vomiting, flatulence, abdominal discomfort, indigestion, asthenia, and headache.
TECOS Cardiovascular Safety Study: The Trial Evaluating Cardiovascular Outcomes with Sitagliptin (TECOS) included 7,332 patients treated with sitagliptin, 100 mg daily (or 50 mg daily if the baseline estimated glomerular filtration rate (eGFR) was ≥30 and <50 mL/min/1.73 m
2), and 7,339 patients treated with placebo in the intention-to-treat population. Both treatments were added to usual care targeting regional standards for HbA1c and CV risk factors. The overall incidence of serious adverse events in patients receiving sitagliptin was similar to that in patients receiving placebo.
In the intention-to-treat population, among patients who were using insulin and/or a sulfonylurea at baseline, the incidence of severe hypoglycemia was 2.7% in sitagliptin-treated patients and 2.5% in placebo-treated patients; among patients who were not using insulin and/or a sulfonylurea at baseline, the incidence of severe hypoglycemia was 1.0% in sitagliptin-treated patients and 0.7% in placebo-treated patients. The incidence of adjudication-confirmed pancreatitis events was 0.3% in sitagliptin-treated patients and 0.2% in placebo-treated patients.
Postmarketing Experience: Additional adverse reactions have been identified during postmarketing use of JANUMET or sitagliptin, one of the components of JANUMET. These reactions have been reported when JANUMET or sitagliptin have been used alone and/or in combination with other antihyperglycemic agents. Because these reactions are reported voluntarily from a population of uncertain size, it is generally not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Hypersensitivity reactions including anaphylaxis, angioedema, rash, urticaria, cutaneous vasculitis, and exfoliative skin conditions including Stevens-Johnson syndrome (see Contraindications; Sitagliptin phosphate: Hypersensitivity Reactions under Precautions); acute pancreatitis; including fatal and non-fatal hemorrhagic and necrotizing pancreatitis (see JANUMET: Pancreatitis under Precautions); worsening renal function, including acute renal failure (sometimes requiring dialysis); bullous pemphigoid; upper respiratory tract infection; nasopharyngitis; constipation; vomiting; headache; arthralgia; myalgia; pain in extremity; back pain; pruritus.
Laboratory Test Findings: Sitagliptin phosphate: The incidence of laboratory adverse experiences was similar in patients treated with sitagliptin and metformin (7.6%) compared to patients treated with placebo and metformin (8.7%). Across clinical studies, a small increase in white blood cell count (approximately 200 cells/microL difference in WBC vs. placebo; mean baseline WBC approximately 6600 cells/microL) was observed due to a small increase in neutrophils. This observation was seen in most but not all studies. This change in laboratory parameters is not considered to be clinically relevant.
Metformin hydrochloride: In controlled clinical trials of metformin of 29 weeks duration, a decrease to subnormal levels of previously normal serum Vitamin B
12 levels, without clinical manifestations, was observed in approximately 7% of patients. Such decrease, possibly due to interference with B
12 absorption from the B
12-intrinsic factor complex, is, however, very rarely associated with anemia and appears to be rapidly reversible with discontinuation of metformin or Vitamin B
12 supplementation (see Metformin hydrochloride: Vitamin B
12 levels under Precautions).




 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image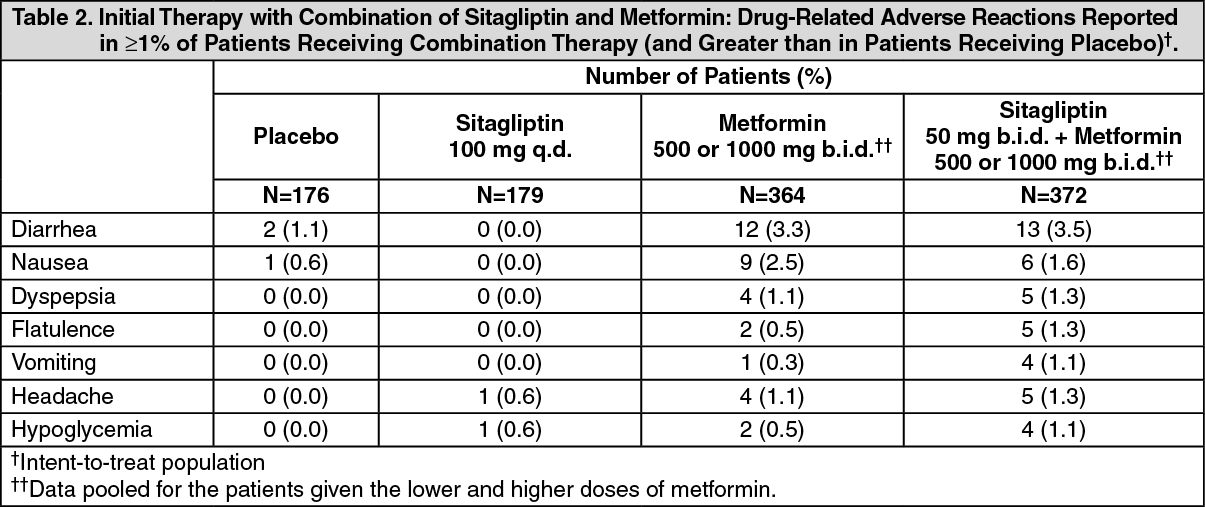 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image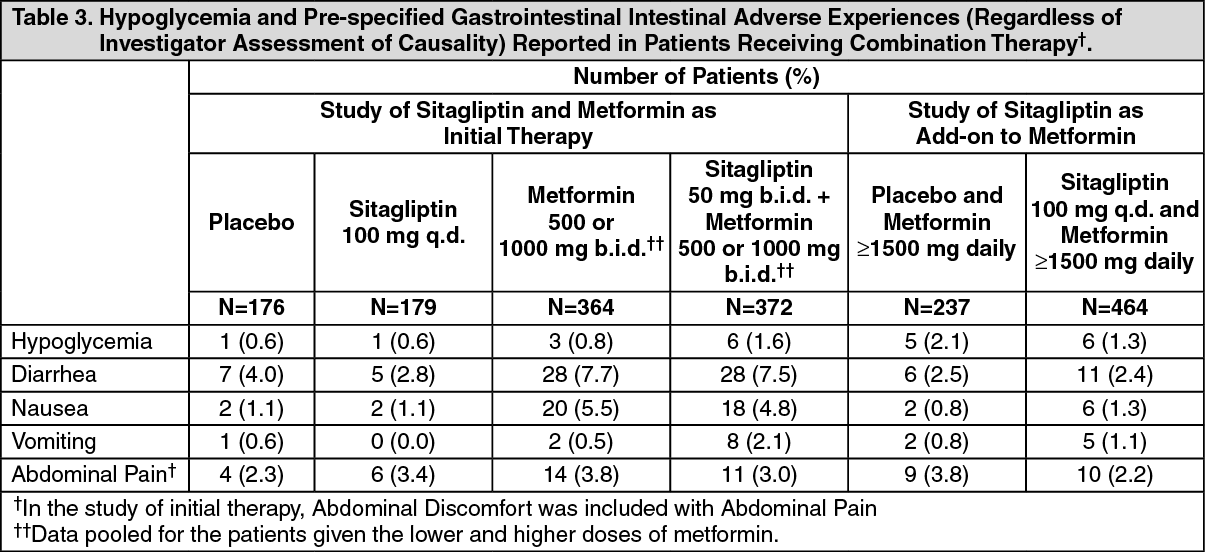 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
