


 Sign Out
Sign Out


Clinical Trial Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
MONALEESA-2: KISQALI in combination with Letrozole: Postmenopausal women with HR-positive, HER2-negative advanced or metastatic breast cancer for initial endocrine based therapy: The safety data reported as follows are based on (MONALEESA-2), a clinical study of 668 postmenopausal women receiving KISQALI plus letrozole or placebo plus letrozole. The median duration of exposure to KISQALI plus letrozole was 13 months with 58% of patients exposed for ≥ 12 months.
Dose reductions due to adverse reactions (ARs) occurred in 45% of patients receiving KISQALI plus letrozole and in 3% of patients receiving placebo plus letrozole. Among patients receiving KISQALI plus letrozole, 7% were reported to have permanently discontinued both KISQALI and letrozole and 7% were reported to have permanently discontinued KISQALI alone due to ARs. Among patients receiving placebo plus letrozole, 2% were reported to have permanently discontinued both and 0.9% were reported to have permanently discontinued placebo alone due to ARs. Adverse reactions leading to treatment discontinuation of KISQALI in patients receiving KISQALI plus letrozole were ALT increased (4%), AST increased (3%), vomiting (2%). Antiemetics and antidiarrhea medications were used to manage symptoms as clinically indicated.
On-treatment deaths, regardless of causality, were reported in three cases (0.9%) of KISQALI plus letrozole treated patients vs. one case (0.3%) of placebo plus letrozole treated patients. Causes of death on KISQALI plus letrozole included one case each of the following: progressive disease, death (cause unknown), and sudden death (in the setting of Grade 3 hypokalemia and Grade 2 QT prolongation).
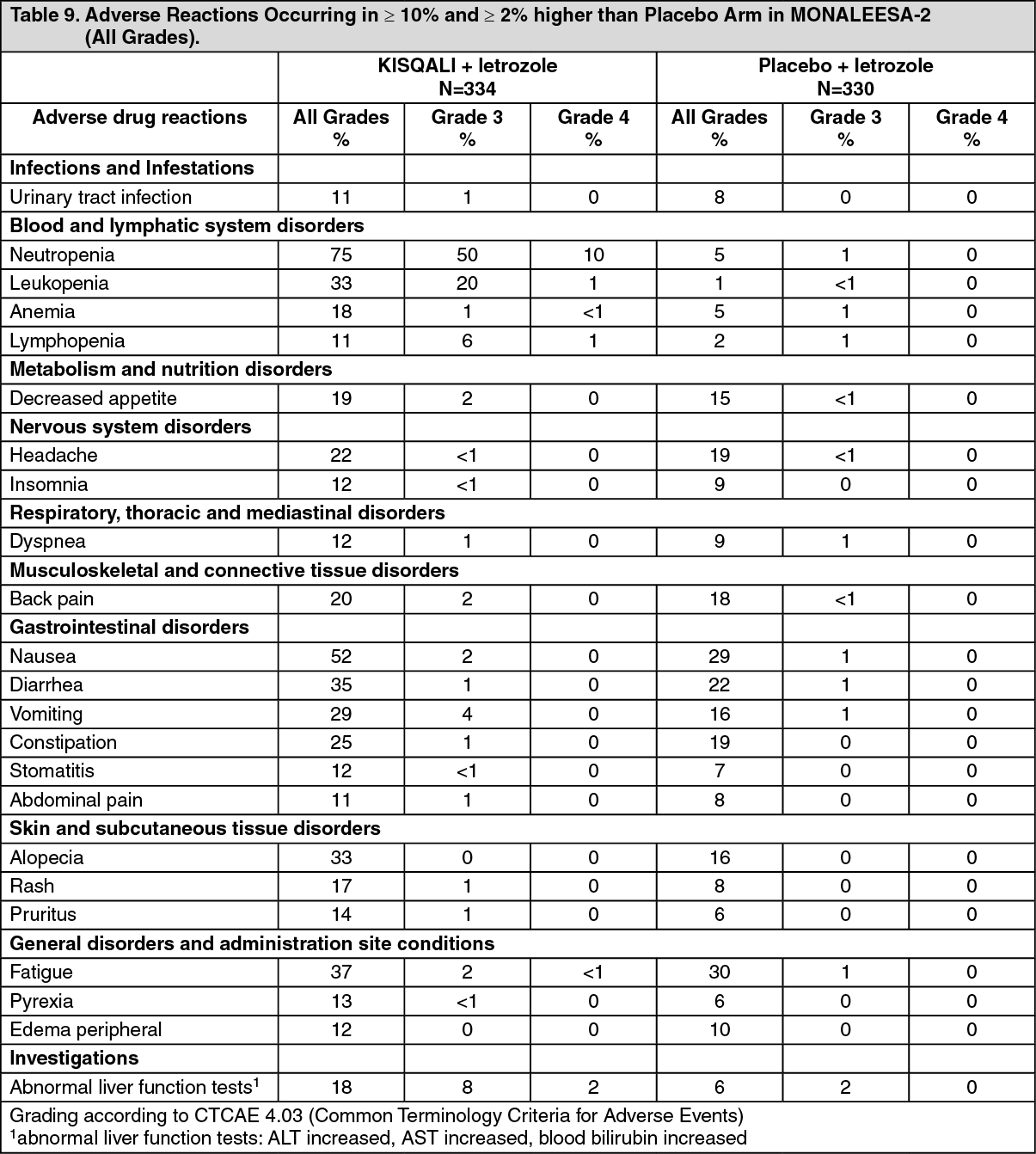
The most common ARs (reported at a frequency ≥ 20% on the KISQALI arm and ≥ 2% higher than placebo) were neutropenia, nausea, fatigue, diarrhea, leukopenia, alopecia, vomiting, constipation, headache, back pain.
The most common Grade 3/4 ARs (reported at a frequency > 5%) were neutropenia, leukopenia, abnormal liver function tests, and lymphopenia.
In MONALEESA-2, syncope occurred in 9 patients (3%) in the KISQALI plus letrozole arm vs. 3 (1%) in placebo plus letrozole arm.
Adverse reactions and laboratory abnormalities occurring in patients in MONALEESA-2 are listed in Table 9 and Table 10, respectively. (See Tables 9 and 10.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image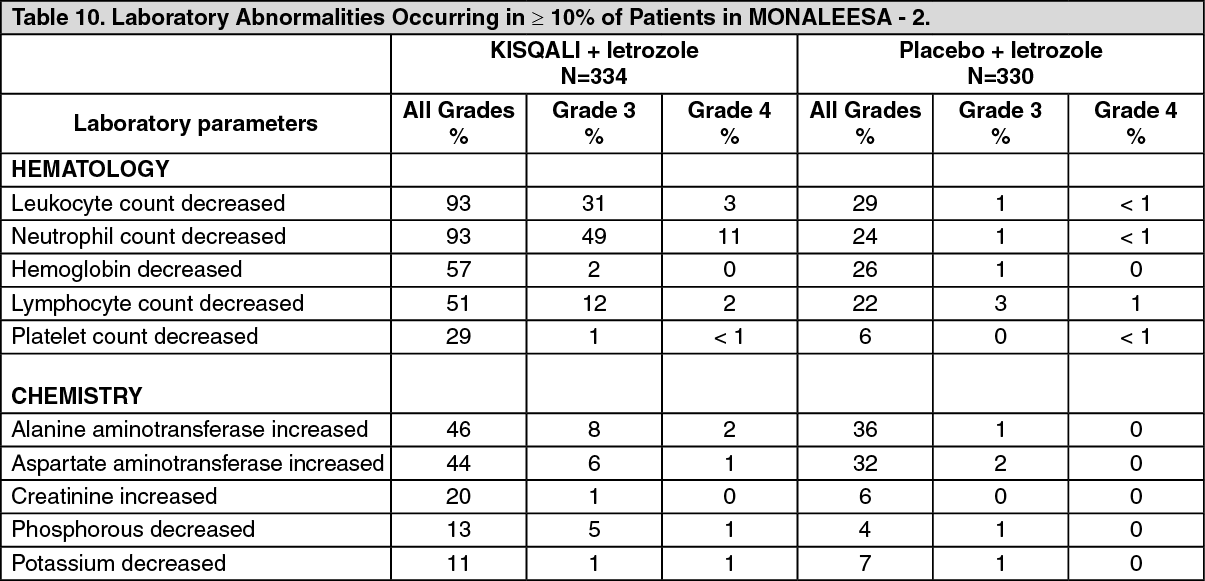 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMONALEESA-7: KISQALI in combination with an Aromatase Inhibitor: Pre/perimenopausal patients with HR-positive, HER2-negative advanced or metastatic breast cancer for initial endocrine based therapy: MONALEESA-7 was conducted in 672 pre/perimenopausal patients with HR-positive, HER2-negative advanced or metastatic breast cancer receiving either KISQALI plus a non-steroidal aromatase inhibitor (NSAI) or tamoxifen plus goserelin or placebo plus NSAI or tamoxifen plus goserelin. The median duration of exposure on the KISQALI arm was 15.2 months with 66% of patients exposed for ≥ 12 months. The safety data reported as follows are based on 495 pre/perimenopausal patients receiving KISQALI plus NSAI plus goserelin or placebo plus NSAI plus goserelin.
Dose reductions due to ARs occurred in 33% of patients receiving KISQALI plus NSAI plus goserelin, and in 4% of patients receiving placebo plus NSAI plus goserelin. Among patients receiving KISQALI plus NSAI, 3% were reported to have permanently discontinued both KISQALI and NSAI and 3% were reported to have permanently discontinued KISQALI alone due to ARs. Among patients receiving placebo plus NSAI, 2% were reported to have permanently discontinued both and 0.8% were reported to have permanently discontinued placebo alone due to ARs. Adverse reactions leading to treatment discontinuation on KISQALI in patients receiving KISQALI plus NSAI (as compared to the placebo arm) were ALT increased (2% vs. 0.8%), AST increased (2% vs. 0.8%), drug-induced liver injury (1% vs. 0.4%).
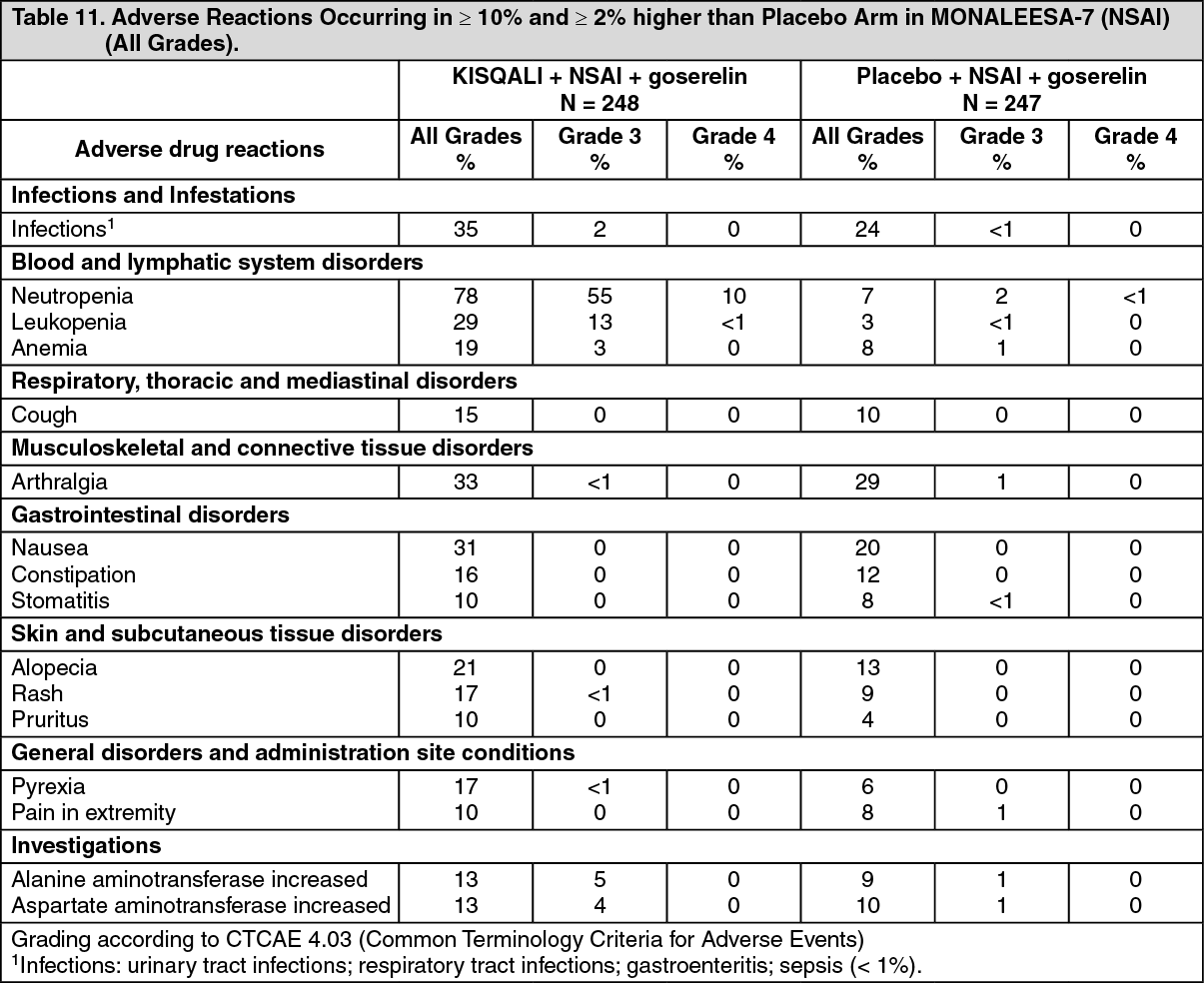
The most common ARs (reported at a frequency ≥ 20% on the KISQALI arm and ≥ 2% higher than placebo) were neutropenia, infections, leukopenia, arthralgia, nausea, and alopecia. The most common Grade 3/4 ARs (reported at a frequency ≥ 5%) were neutropenia, leukopenia, and abnormal liver function tests. See Table 11 as follows.
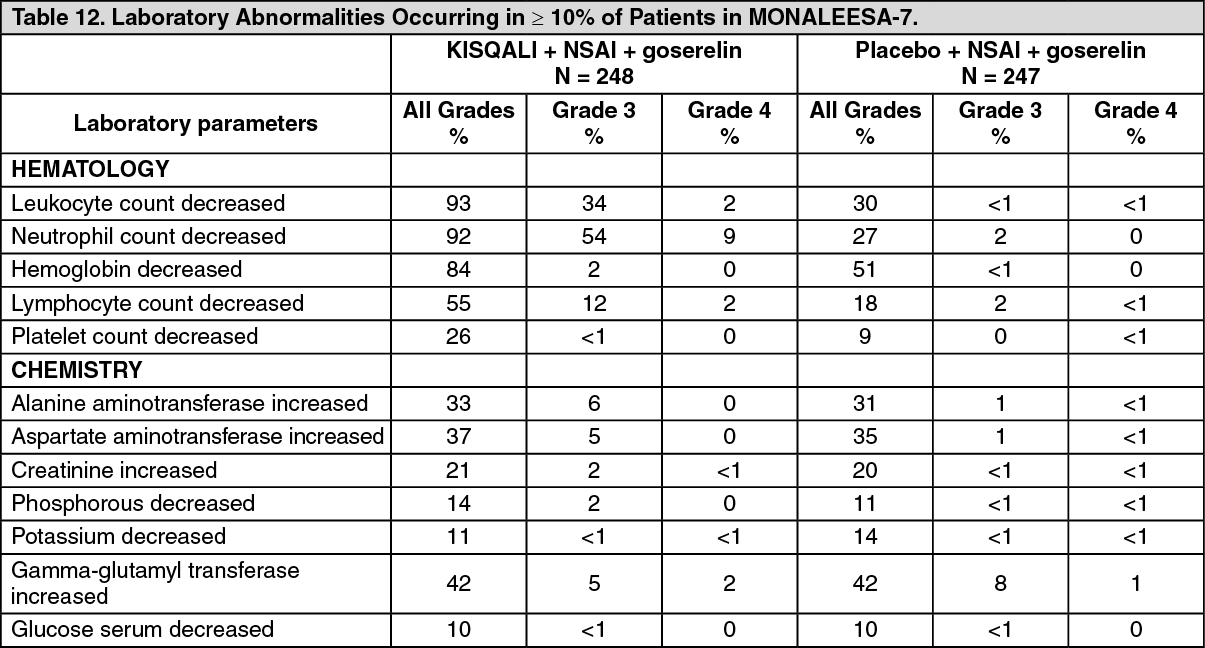
Adverse reactions and laboratory abnormalities occurring in patients in MONALEESA-7 are listed in Table 11 and Table 12, respectively. (See Table 11.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional adverse reactions in MONALEESA-7 for patients receiving KISQALI plus NSAI included asthenia (12%), thrombocytopenia (9%), dry skin (8%), oropharyngeal pain (7%), dyspepsia (5%), lacrimation increased (4%), dry eye (4%), vitiligo (3%), hypocalcemia, (2%), blood bilirubin increased (1%) and syncope (0.4%). (See Table 12.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMONALEESA-3: KISQALI in combination with Fulvestrant: Postmenopausal patients with HR-positive, HER2-negative advanced or metastatic breast cancer for initial endocrine based therapy or after disease progression on endocrine therapy: The safety data reported as follows are based on MONALEESA-3, a clinical study of 724 postmenopausal women receiving KISQALI plus fulvestrant or placebo plus fulvestrant. The median duration of exposure to KISQALI plus fulvestrant was 15.8 months with 58% of patients exposed for ≥ 12 months.
Dose reductions due to ARs occurred in 32% of patients receiving KISQALI plus fulvestrant and in 3% of patients receiving placebo plus fulvestrant. Among patients receiving KISQALI plus fulvestrant, 8% were reported to have permanently discontinued both KISQALI and fulvestrant and 9% were reported to have discontinued KISQALI alone due to ARs. Among patients receiving placebo plus fulvestrant, 4% were reported to have permanently discontinued both and 2% were reported to have discontinued placebo alone due to ARs. Adverse reactions leading to treatment discontinuation of KISQALI in patients receiving KISQALI plus fulvestrant (as compared to the placebo arm) were ALT increased (5% vs. 0%), AST increased (3% vs. 0.6%), and vomiting (1% vs. 0%).
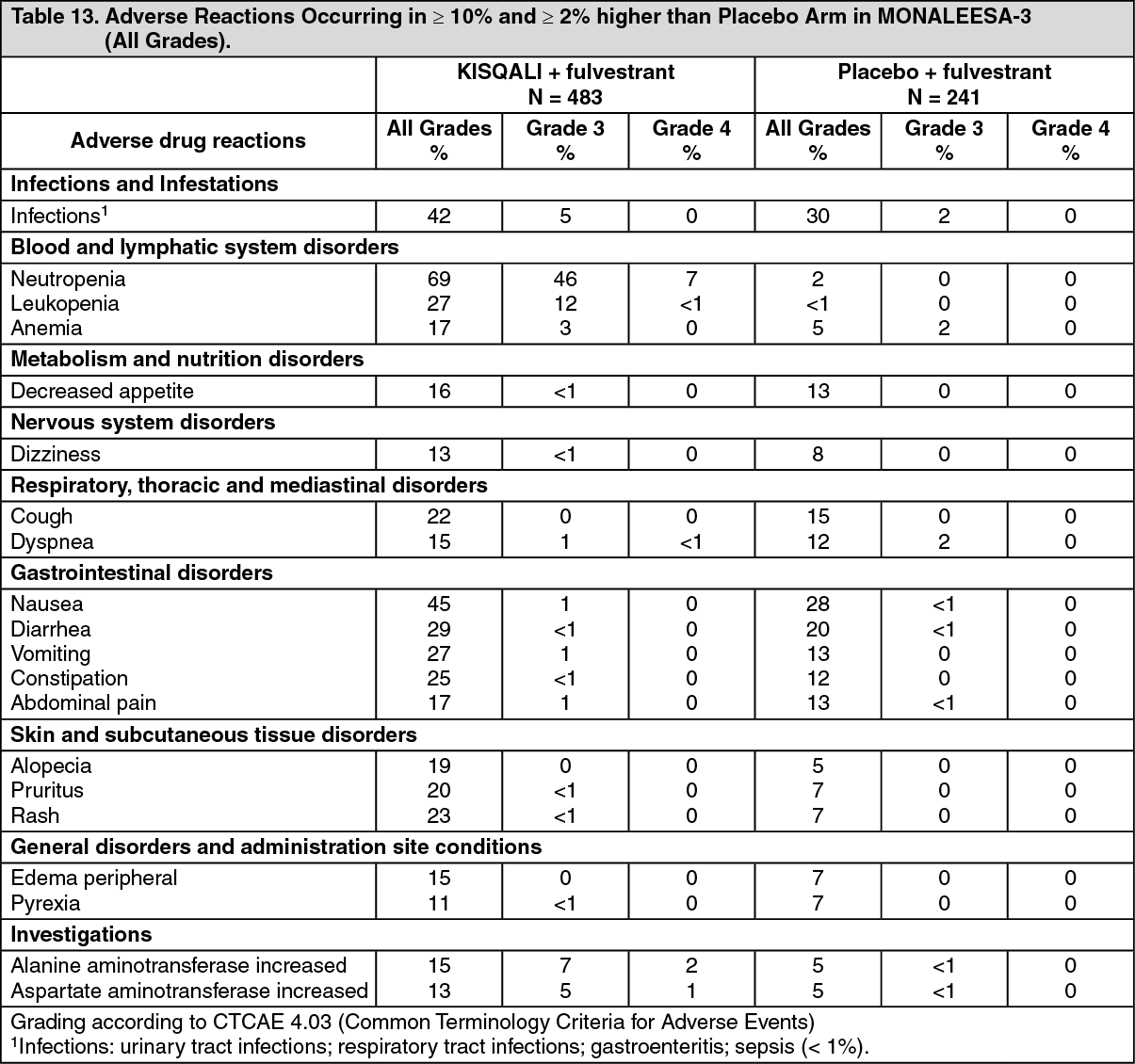
The most common ARs (reported at a frequency ≥ 20% on the KISQALI arm and ≥ 2% higher than placebo) were neutropenia, infections, leukopenia, cough, nausea, diarrhea, vomiting, constipation, pruritus, and rash. The most common Grade 3/4 ARs (reported at a frequency ≥ 5%) were neutropenia, leukopenia, infections, and abnormal liver function tests. See Table 13.
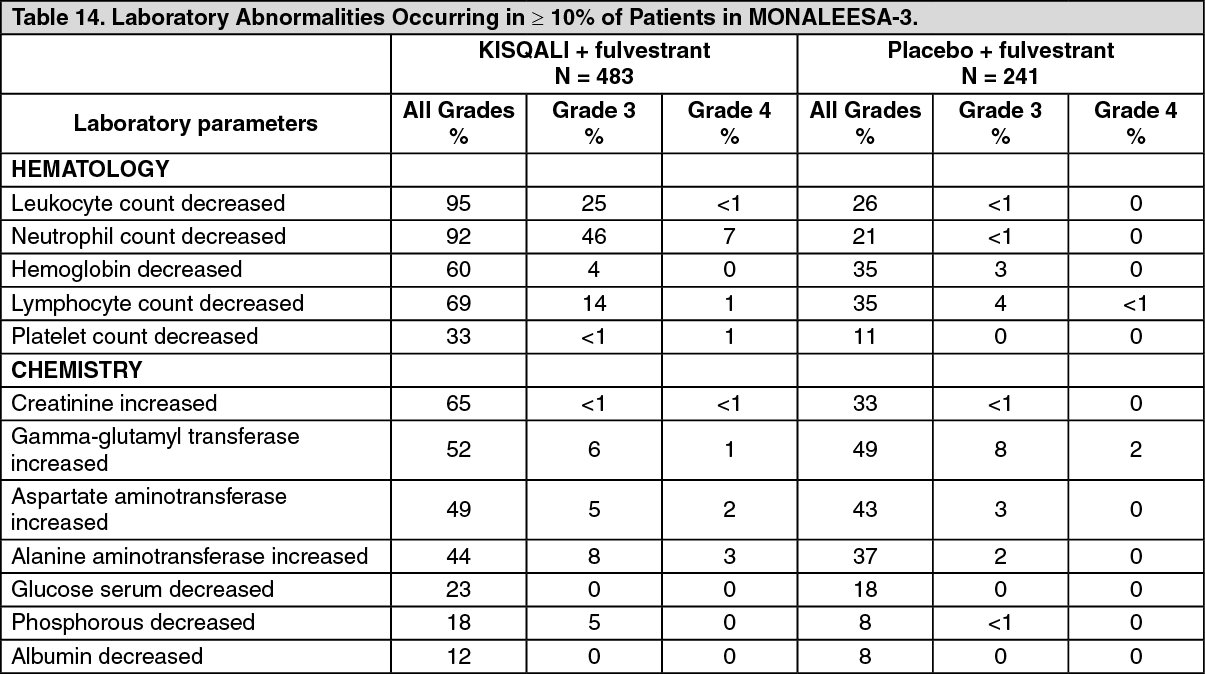
Adverse reactions and laboratory abnormalities occurring in patients in MONALEESA-3 are listed in Table 13 and Table 14, respectively. (See Tables 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional adverse reactions in MONALEESA-3 for patients receiving KISQALI plus fulvestrant included asthenia (14%), dyspepsia (10%), thrombocytopenia (9%) dry skin (8%), dysgeusia (7%), dry mouth (5%), vertigo (5%), dry eye (5%), lacrimation increased (4%), erythema (4%), hypocalcemia (4%), blood bilirubin increased (1%), and syncope (1%). (See Table 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
View ADR Monitoring Form