


 Sign Out
Sign Out


When given with KISQALI, refer to the Full Prescribing Information for the recommended dose of the aromatase inhibitor being used.
When given with KISQALI, the recommended dose of fulvestrant is 500 mg administered on Days 1, 15, 29, and once monthly thereafter. Please refer to the Full Prescribing Information of fulvestrant.
Pre/perimenopausal women treated with the combination KISQALI plus an aromatase inhibitor or fulvestrant should be treated with a luteinizing hormone-releasing hormone (LHRH) agonist according to current clinical practice standards.
Patients should take their dose of KISQALI at approximately the same time each day, preferably in the morning.
If the patient vomits after taking the dose, or misses a dose, no additional dose should be taken that day. The next prescribed dose should be taken at the usual time. KISQALI tablets should be swallowed whole (tablets should not be chewed, crushed or split prior to swallowing). No tablet should be ingested if it is broken, cracked, or otherwise not intact.
Dose Modifications: Dose Modifications for Adverse Reactions: The recommended dose modifications for adverse reactions are listed in Table 4. (See Table 4.)
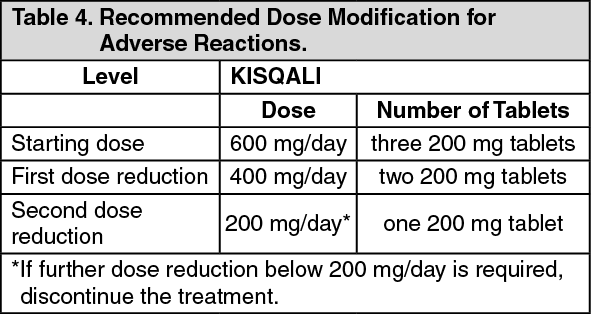 Click on icon to see table/diagram/image
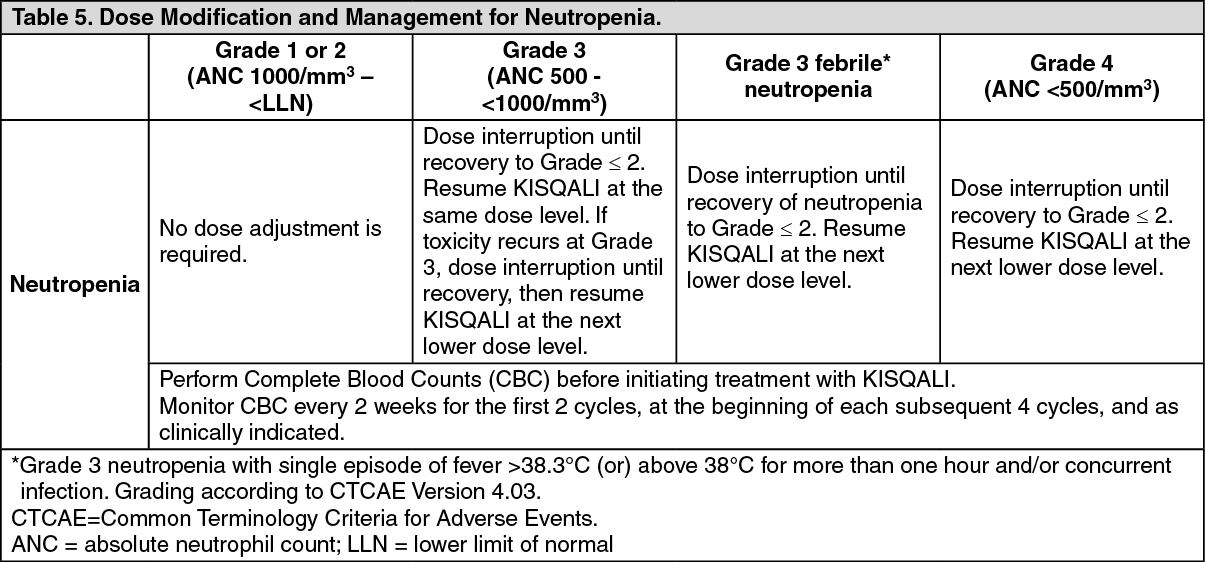
Click on icon to see table/diagram/imageTables 5, 6, 7 and 8 summarize recommendations for dose interruption, reduction, or discontinuation of KISQALI in the management of specific adverse reactions. Dose modification of KISQALI is recommended based on individual safety and tolerability. (See Tables 5, 6, 7, and 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image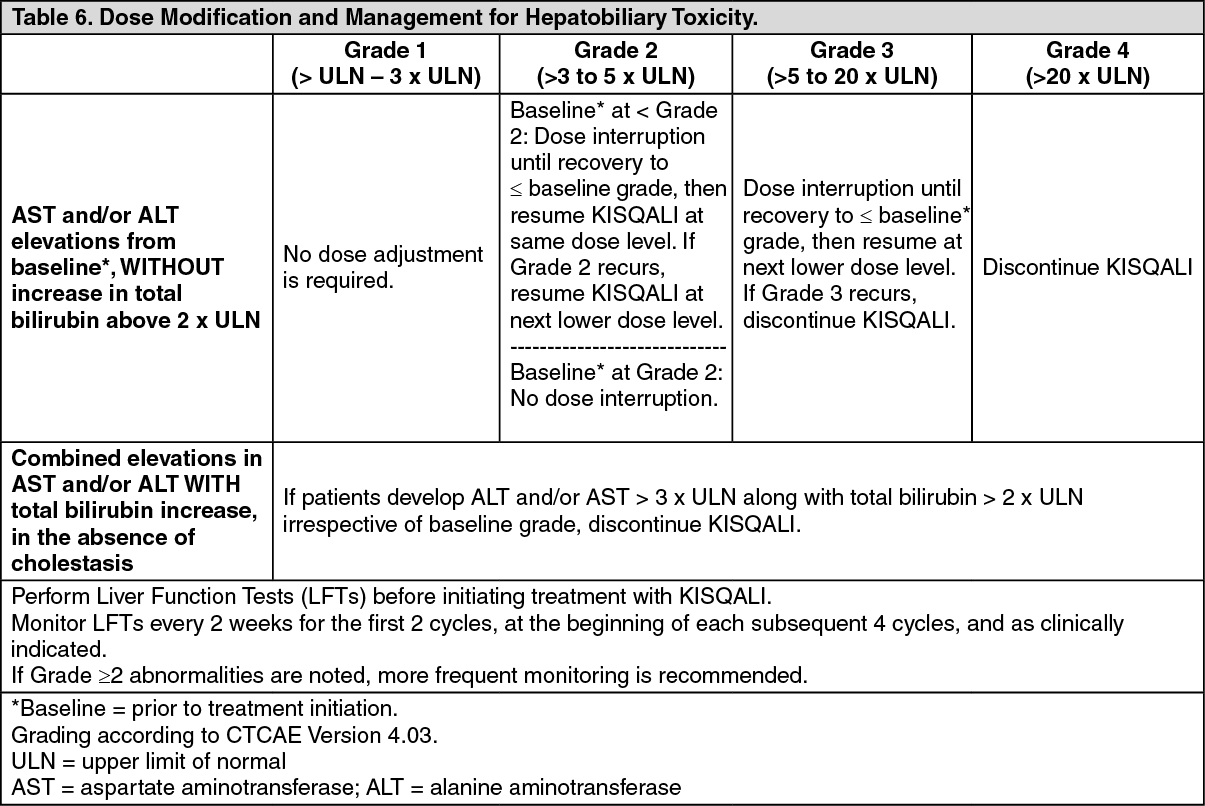 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image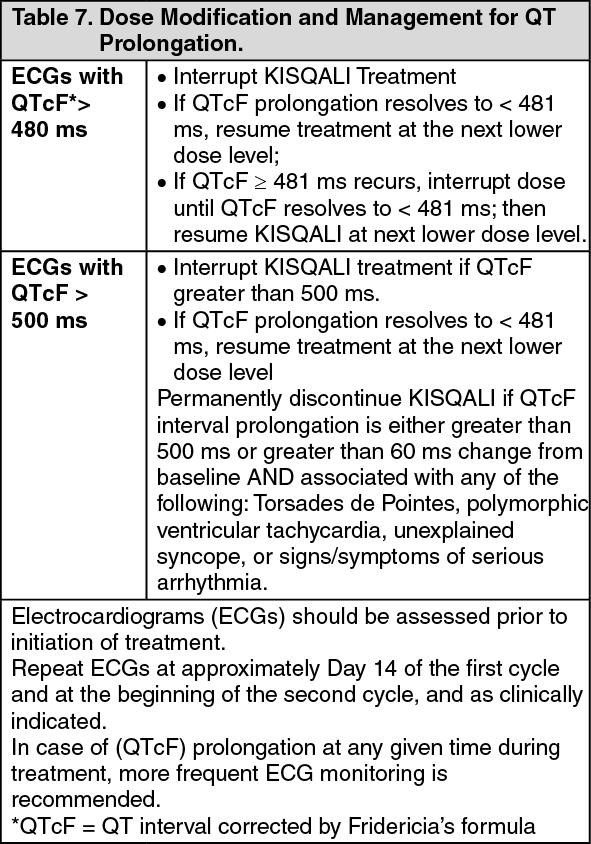 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image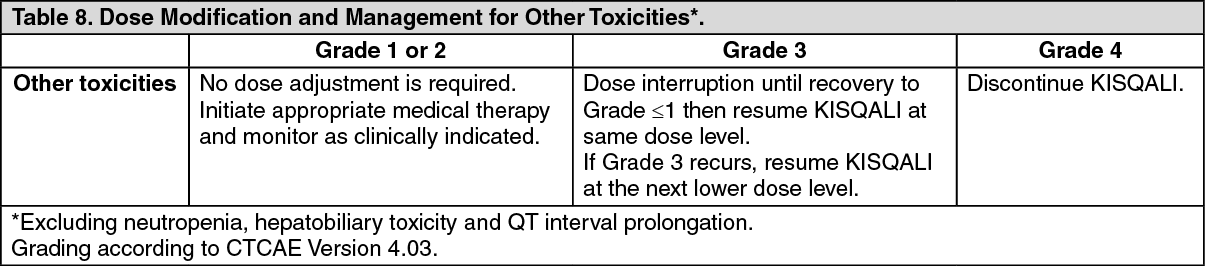 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRefer to the Full Prescribing Information for the coadministered aromatase inhibitor or fulvestrant for dose modification guidelines in the event of toxicity and other relevant safety information.
Dose Modification for Use with Strong CYP3A Inhibitors: Avoid concomitant use of KISQALI with strong CYP3A inhibitors and consider an alternative concomitant medication with less potential for CYP3A inhibition (see Drugs That May Increase Ribociclib Plasma Concentrations under Interactions). If a strong CYP3A inhibitor must be coadministered, reduce the KISQALI dose to 400 mg once daily. If the strong inhibitor is discontinued, change the KISQALI dose (after at least 5 half-lives of the strong CYP3A inhibitor) to the dose used prior to the initiation of the strong CYP3A inhibitor (see Drugs That May Increase Ribociclib Plasma Concentrations under Interactions and Pharmacology: Pharmacokinetics under Actions).
Dose Modification for Hepatic Impairment: No dose adjustment is necessary in patients with mild hepatic impairment (Child-Pugh class A). The recommended starting dose is 400 mg KISQALI once daily for patients with moderate (Child-Pugh class B) and severe hepatic impairment (Child-Pugh class C) (see Use in Specific Populations: Hepatic Impairment under Precautions and Pharmacology: Pharmacokinetics under Actions).
Review the Full Prescribing Information for the coadministered aromatase inhibitor or fulvestrant for dose modifications related to hepatic impairment.
Dose Modification for Renal Impairment: No dose adjustment is necessary in patients with mild or moderate renal impairment. The recommended starting dose is 200 mg KISQALI once daily for patients with severe renal impairment (see Use in Specific Populations: Renal Impairment under Precautions and Pharmacology: Pharmacokinetics under Actions).