The information given below is based on data from clinical studies on extensive post-marketing experience.
Frequencies are defined using the following convention: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1,000 to <1/100), rare (≥1/10,000 to <1/1,000), very rare (<1/10,000), not known (cannot be estimated from the available data). Within each frequency grouping, undesirable effects are presented in order of decreasing seriousness.
Infections and infestations: Uncommon: Fungal infection including Candida infection, pathogen resistance.
Blood and lymphatic system disorders: Uncommon: Eosinophilia, leukopenia.
Rare: Neutropenia, thrombocytopenia.
Not known: Haemolytic anaemia, pancytopenia, agranulocytosis.
Immune system disorders: Rare: Angioedema, hypersensitivity.
Not known: Anaphylactic shock, anaphylactoid shock (Anaphylactic and anaphylactoid reactions may sometimes occur even after the first dose).
Metabolism and nutrition disorders: Uncommon: Anorexia.
Rare: Hypoglycaemia, particularly in diabetic patients.
Not known: Hyperglycaemia, hypoglycaemic coma.
Psychiatric disorders: Common: Insomnia.
Uncommon: Confusional state, anxiety, nervousness.
Rare: Psychotic reactions (with e.g. hallucination, paranoia), depression, agitation, abnormal dreams, nightmares.
Not known: Psychotic disorders with self-endangering behaviour including suicidal ideation or suicide attempt.
Nervous system disorders: Common: Headache, dizziness.
Uncommon: Somnolence, tremor, dysgeusia.
Rare: Convulsion, paraesthesia.
Not known: Peripheral sensory neuropathy, peripheral sensory motor neuropathy, parosmia including anosmia, dyskinesia, extrapyramidal disorder, ageusia, syncope, benign intracranial hypertension.
Eye disorders: Rare: Visual disturbances such as blurred vision.
Not known: Transient vision loss, uveitis.
Ear and labyrinth disorders: Uncommon: Vertigo.
Rare: Tinnitus.
Not known: Hearing loss, hearing impaired.
Cardiac disorders: Rare: Tachycardia, palpitation.
Not known: Ventricular tachycardia, which may result in cardiac arrest, ventricular arrhythmia and torsades de pointes (reported predominantly in patients with risk factors for QT prolongation), electrocardiogram QT prolonged.
Vascular disorders: Rare: Hypotension.
Respiratory, thoracic and mediastinal disorders: Uncommon: Dyspnoea.
Not known: Bronchospasm, pneumonitis, allergic.
Gastrointestinal disorders: Common: Diarrhoea, vomiting, nausea.
Uncommon: Abdominal pain, dyspepsia, flatulence, constipation.
Not known: Diarrhoea-haemorrhagic which in very rare cases may be indicative of enterocolitis, including pseudomembranous colitis, pancreatitis.
Hepatobiliary disorders: Common: Hepatic enzyme increased (ALT/AST, alkaline phosphatase, GGT).
Uncommon: Blood bilirubin increased.
Not known: Jaundice and severe liver injury, including cases with fatal acute liver failure, primarily in patients with severe underlying diseases, hepatitis.
Skin and subcutaneous tissue disorders (Mucocutaneous reactions may sometimes occur even after the first dose): Uncommon: Rash, pruritus, urticarial, hyperhidrosis.
Not known: Toxic epidermal necrolysis, Stevens-Johnson syndrome, erythema multiforme, photosensitivity reaction, leukocytoclastic vasculitis, stomatitis.
Musculoskeletal and connective tissue disorders: Uncommon: Arthralgia, myalgia.
Rare: Tendon disorder including tendinitis (e.g. Achilles tendon), muscular weakness which may be of special importance in patients with myasthenia gravis.
Not known: Rhabdomyolysis, tendon rupture (e.g. Achilles tendon), ligament rupture, muscle rupture, arthritis.
Renal and urinary disorders: Uncommon: Blood creatinine increased.
Rare: Renal failure acute (e.g. due to interstitial nephritis).
General disorders and administration site conditions: Uncommon: Asthenia.
Rare: Pyrexia.
Not known: Pain (including pain in back, chest, and extremities).
Other undesirable effects which have been associated with fluoroquinolone administration include attacks of porphyria in patients with porphyria.


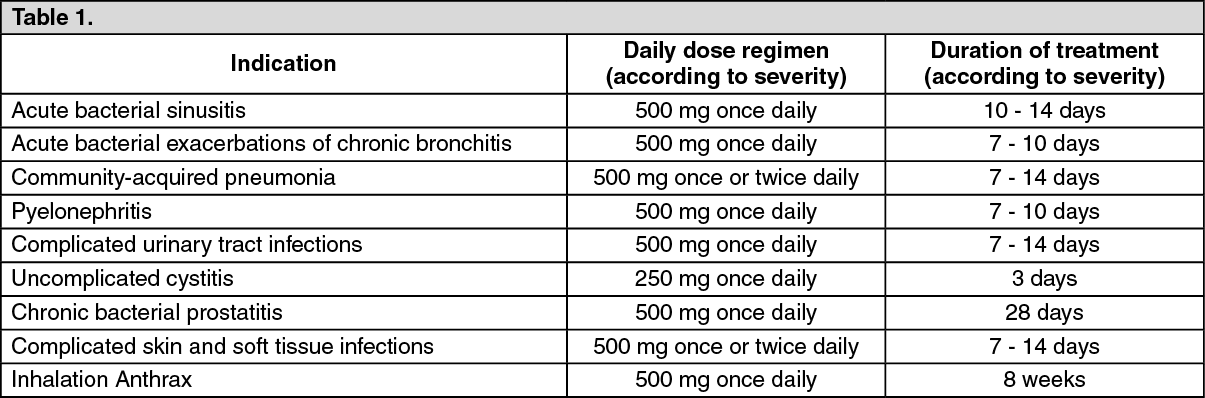 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image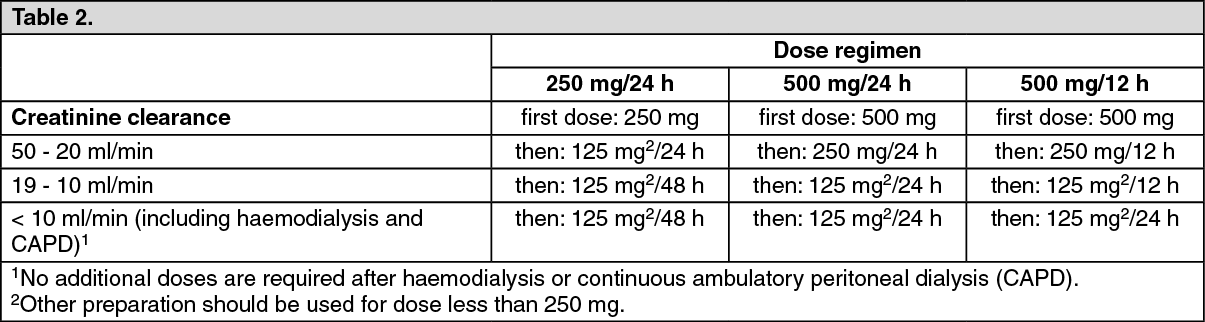 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out