


 Sign Out
Sign Out



Clinical Studies: Efficacy: The serum bactericidal assay (SBA) used to test sera contained an exogenous complement source 23 that was either human (SBA-H) or baby rabbit (SBA-BR).
The response to vaccination following two doses of vaccine administered to children 9 and 12 months of age and following one dose of vaccine administered to children 2 through 10 years of age was evaluated by the proportion of participants having an SBA-H antibody titer of 1:8 or greater, for each serogroup. In individuals 11 through 55 years of age, the response to vaccination with a single dose of vaccine was evaluated by the proportion of participants with a 4-fold or greater increase in bactericidal antibody to each serogroup as measured by SBA-BR. For individuals 2 through 55 years of age, vaccine efficacy after a single dose was inferred from the demonstration of immunologic equivalence to a US-licensed meningococcal polysaccharide vaccine, Menomune - A/C/Y/W-135 vaccine as assessed by SBA.
Immunogenicity: Children 9 through 12 Months of Age: In a randomized, US, multi-center trial, children received Menactra at 9 months and 12 months of age. The first Menactra dose was administered alone, followed by a second Menactra dose given alone (N=404), or with MMRV (N=302), or with PCV7 (N=422). For all participants, sera were obtained approximately 30 days after last vaccination. There were no substantive differences in demographic characteristics between the vaccine groups. The median age range for administration of the first dose of Menactra was 278-279 days of age. (See Table 1.)
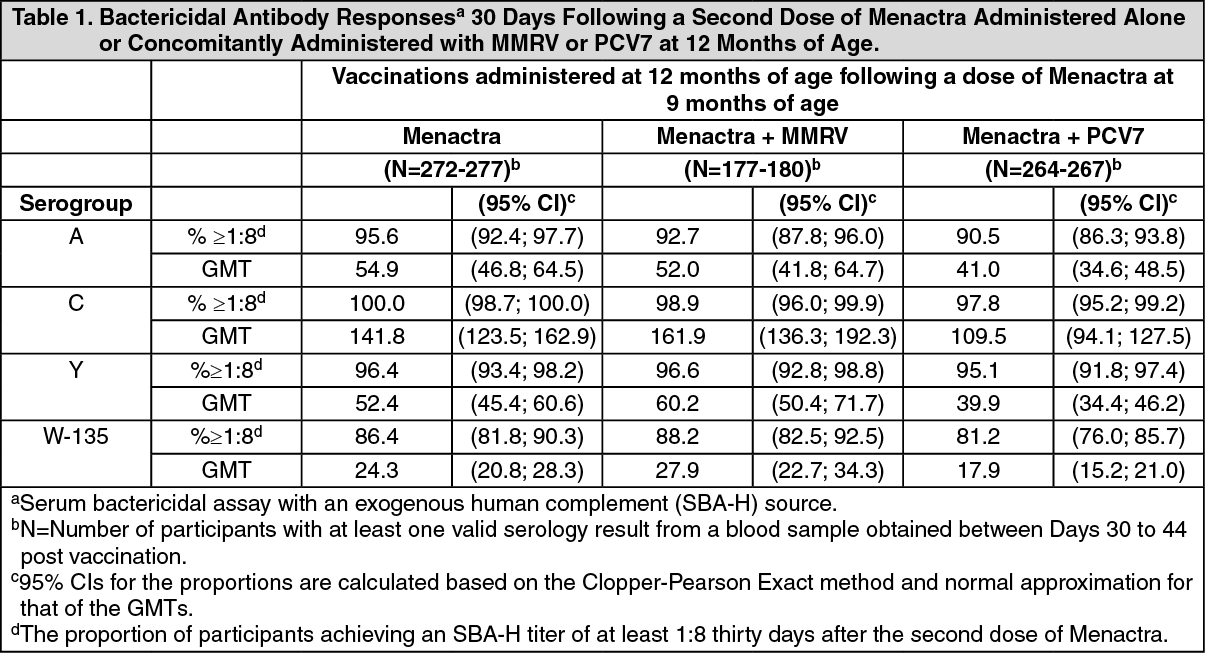 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdministration of Menactra to children at 12 months and 15 months of age was evaluated in a US study. Prior to the first dose, 33.3% [n=16/48] of participants had an SBA-H titer >1:8 to Serogroup A, and 0-2% [n=0-1 of 50-51] to Serogroups C, Y and W-135. After the second dose, percentages of participants with an SBA-H titer >1:8 were: 85.2%, Serogroup A [n=46/54]; 100.0%, Serogroup C [n=54/54]; 96.3%, Serogroup Y [n=52/54]; 96.2%, Serogroup W-135 [n=50/52].
Individuals 2 through 55 Years of Age: Immunogenicity was evaluated in three comparative, randomized, US, multi-center, active controlled clinical trials that enrolled children (2 through 10 years of age), adolescents (11 through 18 years of age), and adults (18 through 55 years of age). Participants received a single dose of Menactra (N=2526) or Menomune - A/C/Y/W-135(N=2317). For all age groups studied, sera were obtained before and approximately 28 days after vaccination. [Blinding procedures for safety assessments are described in Adverse Reactions.]
In each of the trials, there were no substantive differences in demographic characteristics between the vaccine groups, between immunogenicity subsets or the overall study population. In the study of children 2 through 10 years of age, the median age of participants was 3 years; 95% completed the study. In the adolescent trial, the median age for both groups was 14 years; 99% completed the study. In the adult trial, the median age for both groups was 24 years; 94% completed the study.
Immunogenicity in Children 2 through 10 Years of Age: Of 1408 enrolled children 2 through 10 years of age, immune responses evaluated in a subset of Menactra participants (2 through 3 years of age, n=52; 4-10 years of age, n=84) and Menomune - A/C/Y/W-135 participants (2 through 3 years of age, n=53; 4-10 years of age, n=84) were comparable for all four serogroups (Table 2).
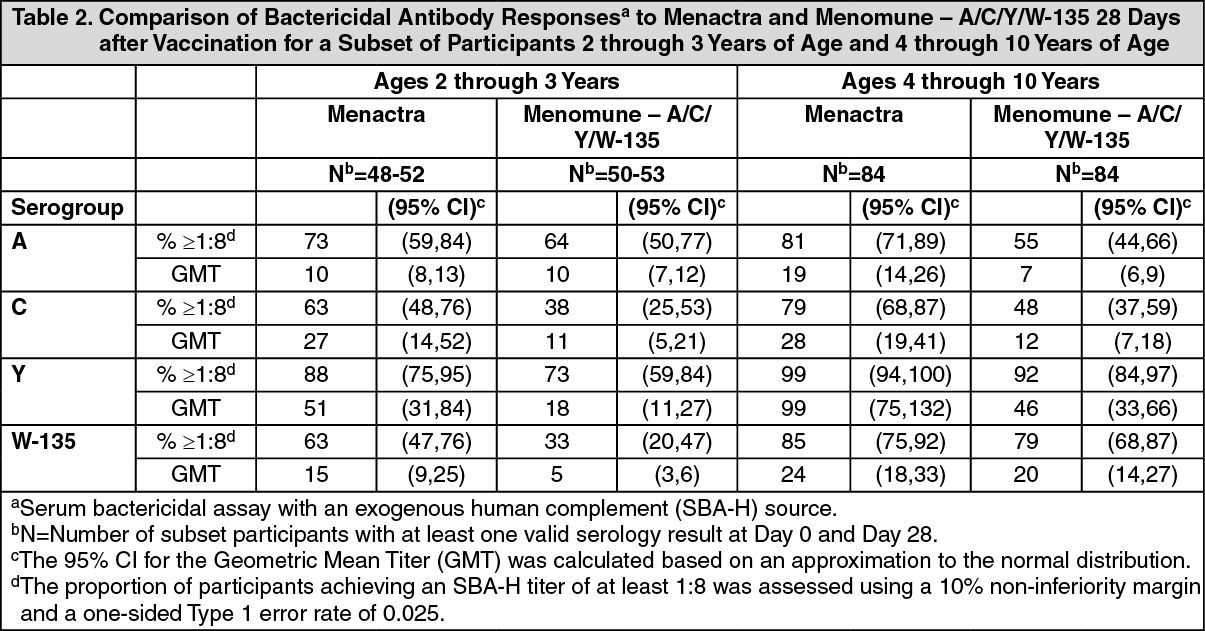 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the subset of participants 2 through 3 years of age with undetectable pre-vaccination titers (ie, SBA-H titers <1:4 at Day 0), seroconversion rates (defined as the proportions of participants with SBA-H titers ≥1:8 by Day 28) were similar between the Menactra and Menomune - A/C/Y/W- 135 recipients. Menactra participants achieved seroconversion rates of: 57%, Serogroup A (n=12/21); 62%, Serogroup C (n=29/47); 84%, Serogroup Y (n=26/31); 53%, Serogroup W-135 (n=20/38). The seroconversion rates for Menomune - A/C/Y/W-135 recipients were: 55%, Serogroup A (n=16/29); 30%, Serogroup C (n=13/43); 57%, Serogroup Y (n=17/30); 26%, Serogroup W-135 (n=11/43).
In the subset of participants 4 through 10 years of age with undetectable pre-vaccination titers (ie, SBA-H titers <1:4 at Day 0), seroconversion rates (defined as the proportions of participants with SBA-H titers ≥1:8 by Day 28) were similar between the Menactra and Menomune - A/C/Y/W- 135 recipients. Menactra participants achieved seroconversion rates of: 69%, Serogroup A (n=11/16); 81%, Serogroup C (n=50/62); 98%, Serogroup Y (n=45/46); 69%, Serogroup W-135 (n=27/39). The seroconversion rates for Menomune - A/C/Y/W-135 recipients were: 48%, Serogroup A (n=10/21); 38%, Serogroup C (n=19/50); 84%, Serogroup Y (n=38/45); 68%, Serogroup W-135 (n=26/38).
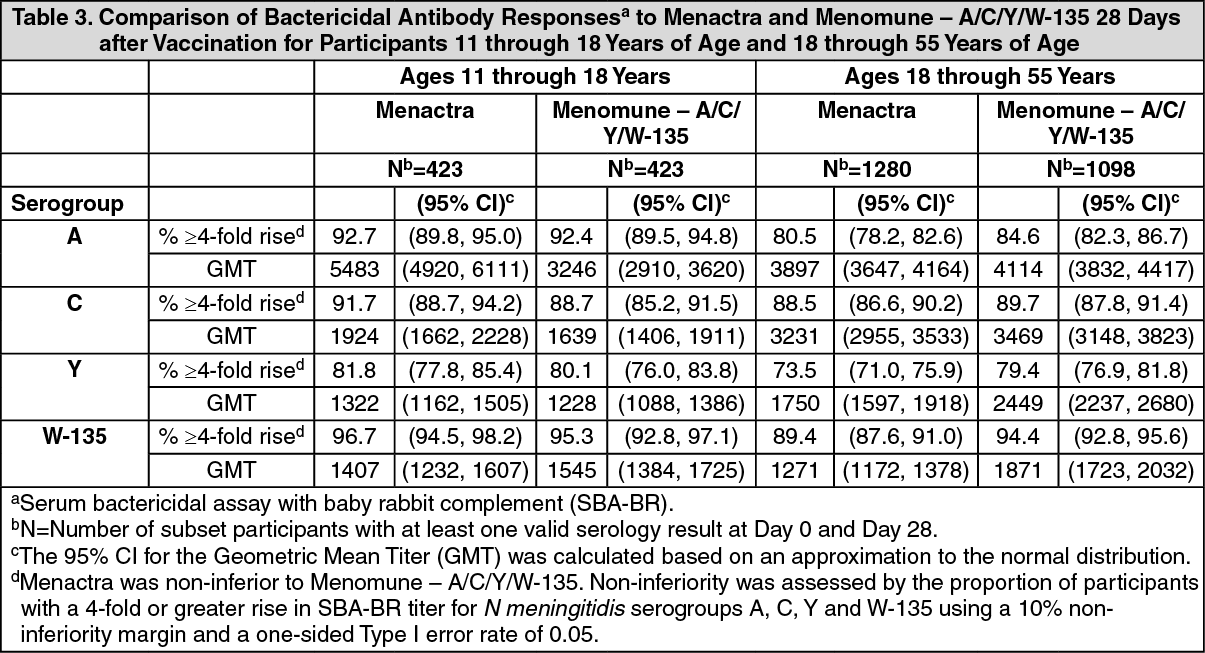
Immunogenicity in Adolescents 11 through 18 Years of Age: 20 Results from the comparative clinical trial conducted in 881 adolescents aged 11 through 18 years 21 showed that the immune responses to Menactra and Menomune - A/C/Y/W-135 were similar for 22 all four serogroups (Table 3).
In participants with undetectable pre-vaccination titers (ie, SBA-BR titers <1:8 at Day 0), seroconversion rates (defined as the proportions of participants achieving a ≥4-fold rise in SBA- BR titers by Day 28) were similar between the Menactra and Menomune - A/C/Y/W-135 recipients. Menactra participants achieved seroconversion rates of: 100%, Serogroup A (n=81/81); 99%, Serogroup C (n=153/155); 98%, Serogroup Y (n=60/61); 98%, Serogroup W- 135 (n=161/164). The seroconversion rates for Menomune - A/C/Y/W-135 recipients were: 100%, Serogroup A (n=93/93); 99%, Serogroup C (n=151/152); 100%, Serogroup Y (n=47/47); 99%, Serogroup W-135 (n=138/139).
Immunogenicity in Adults 18 through 55 Years of Age: Results from the comparative clinical trial conducted in 2554 adults aged 18 through 55 years showed that the immune responses to Menactra and Menomune - A/C/Y/W-135 were similar for all four serogroups (Table 3).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn participants with undetectable pre-vaccination titers (ie, SBA-BR titers <1:8 at Day 0), seroconversion rates (defined as the proportions of participants achieving a ≥4-fold rise in SBA- BR titers by Day 28) were similar between the Menactra and Menomune - A/C/Y/W-135 recipients. Menactra participants achieved seroconversion rates of: 100%, Serogroup A (n=156/156); 99%, Serogroup C (n=343/345); 91%, Serogroup Y (n=253/279); 97%, Serogroup W-135 (n=360/373). The seroconversion rates for Menomune - A/C/Y/W-135 recipients were: 99%, Serogroup A (n=143/144); 98%, Serogroup C (n=297/304); 97%, Serogroup Y (n=221/228); 99%, Serogroup W-135 (n=325/328).
Immunogenicity in Adolescents and Adults Following Booster Vaccination: For a description of the study design and number of participants, [see Clinical Trials Experience, Booster Vaccination Study (see Adverse Reactions).] Prior to revaccination, the percentage of participants (n=781) with an SBA-H titer >1:8 were 64.5%, 44.2%, 38.7%, and 68.5% for Serogroups A, C, Y, and W- 135, respectively. Among the subset of trial participants (n=112) for whom SBA-H responses at Day 6 were assessed, 86.6%, 91.1%, 94.6%, and 92.0% achieved a ≥4-fold rise in SBA-H titer for Serogroups A, C, Y, and W-135, respectively. The proportions of participants (n=781) who achieved a ≥4-fold rise in SBA-H titer by Day 28 were 95.0%, 95.3%, 97.1%, and 96% for Serogroups A, C, Y, and W-135, respectively. The proportions of participants who achieved an SBA-H titer ≥1:8 by Day 28 were >99% for each serogroup.
Concomitant Vaccine Administration: MMRV (or MMR + V) or PCV7: In a US, active-controlled trial, 1179 children received Menactra at 9 months and 12 months of age. At 12 months of age these children received Menactra concomitantly with MMRV (N=616), or MMR + V (N=48), or PCV7 (N=250). Another group of 12-month old children received MMRV + PCV7 (N=485). Sera were obtained approximately 30 days after the last vaccinations. Measles, mumps, rubella and varicella antibody responses among children who received Menactra and MMRV (or MMR and V) were comparable to corresponding antibody responses among children who received MMRV and PCV7.
When Menactra was given concomitantly with PCV7, the non-inferiority criteria for comparisons of pneumococcal IgG GMCs (upper limit of the two-sided 95% CI of the GMC ratio ≤2) were not met for 3 of 7 serotypes (4, 6B, 18C). In a subset of participants with available sera, pneumococcal opsonophagocytic assay GMT data were consistent with IgG GMC data.
Td Vaccine: In a double-blind, randomized, controlled trial, 1021 participants aged 11 through 17 years received Td vaccine and Menactra concomitantly (N=509), or Td vaccine followed one month later by Menactra (N=512). Sera were obtained approximately 28 days after each respective vaccination. The proportions of participants with a 4-fold or greater increase in SBA-BR titer to meningococcal Serogroups C, Y and W-135 were higher when Menactra was given concomitantly with Td vaccine (86%-96%) than when Menactra was given one month following Td vaccine (65%-91%). Anti-tetanus and anti-diphtheria antibody responses were similar in both study groups.
Typhim Vi: In a double-blind, randomized, controlled trial, 945 participants aged 18 through 55 years received Typhim Vi and Menactra concomitantly (N=469), or Typhim Vi followed one month later by Menactra (N=476). Sera were obtained approximately 28 days after each respective vaccination. The antibody responses to Menactra and to Typhim Vi components were similar in both study groups.
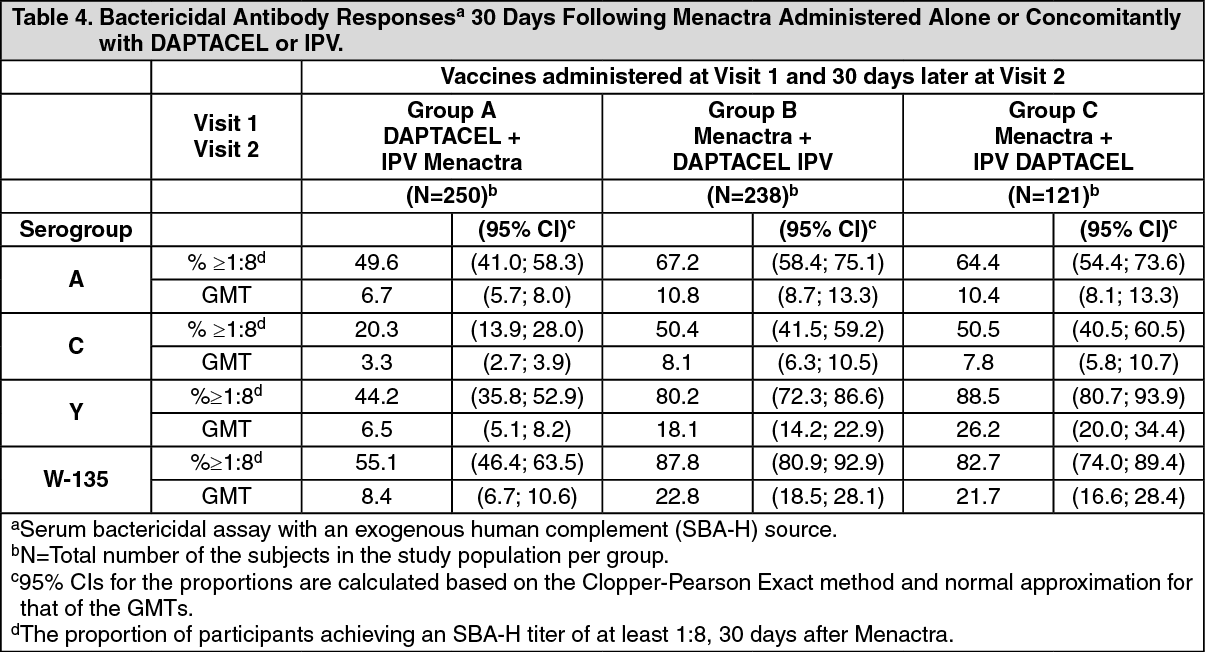
DAPTACEL and IPV: In a randomized, parallel group, US multi-center clinical trial conducted in children 4 through 6 years of age, Menactra was administered as follows: 30 days after concomitant DTaP (DAPTACEL, Sanofi Pasteur Limited) + IPV (IPOL, Sanofi Pasteur SA) [Group A]; concomitantly with DAPTACEL followed 30 days later by IPV [Group B]; concomitantly with IPV followed 30 days later by DAPTACEL [Group C]. Sera were obtained approximately 30 days after each respective vaccination. [See Clinical Trials Experience under Adverse Reactions).
When Menactra was administered 30 days after DAPTACEL (and IPV) [Group A], significantly lower SBA-H GMTs to all 4 meningococcal serogroups were observed compared to Menactra (and IPV) administered 30 days prior to DAPTACEL [Group C]. When Menactra was administered concomitantly with DAPTACEL [Group B], SBA-H GMTs to meningococcal serogroups A, C, and W-135 were non-inferior to those observed after Menactra (and IPV) [Group C]. The non-inferiority criterion was marginally missed for meningococcal serogroup Y. Non-inferiority of SBA-H GMTs following concomitant administration of Menactra and DAPTACEL compared to those after concomitant Menactra and IPV was concluded if the upper limit of the 2-sided 95% CI of (GMTGroup C divided by GMTGroup B) computed separately for each of the serogroups was < 2.
The respective SBA-H GMTs and proportion (%) of Group A, B, and C study participants 6 achieving an SBA-H titer of ≥1:8 are displayed in Table 4. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageWhen Menactra was administered concomitantly with DAPTACEL, antibody responses to three of the pertussis antigens (pertussis toxin, filamentous hemagglutinin, and pertactin) (GMCs), tetanus toxin (% participants with antibody concentrations > 1.0 IU/mL), and diphtheria toxin (% participants with antibody concentrations > 1.0 IU/mL) were non-inferior to those observed after DAPTACEL and IPV. The pertussis anti-fimbriae GMCs were marginally lower when Menactra and DAPTACEL were administered concomitantly.
Non-Clinical Toxicology: Carcinogenesis, Mutagenesis, Impairment of Fertility: Menactra has not been evaluated for carcinogenic or mutagenic potential, or for impairment of male fertility. A developmental animal toxicity study showed that Menactra had no effects on female fertility in mice [see Pregnancy under Use in Pregnancy & Lactation].