Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a vaccine cannot be directly compared to rates in the clinical trials of another vaccine and may not reflect the rates observed in practice.
Children 9 Through 12 Months of Age: The safety of Menactra was evaluated in four clinical studies that enrolled 3721 participants who received Menactra at 9 and 12 months of age. At 12 months of age these children also received one or more other recommended vaccines [Measles, Mumps, Rubella and Varicella Virus Vaccine Live (MMRV) or Measles, Mumps, and Rubella Virus Vaccine (MMR) and Varicella Virus Vaccine Live (V) each manufactured by Merck & Co., Inc., Pneumococcal 7-valent Conjugate Vaccine (Diphtheria CRM197 Protein) manufactured by Wyeth Pharmaceuticals Inc. (PCV7), Hepatitis A Vaccine manufactured by Merck & Co., Inc. (HepA). A control group of 997 children was enrolled at 12 months of age and received two or more childhood vaccines [MMRV (or MMR+V), PCV7, HepA] at 12 months of age [see Pharmacology: Clinical Studies: Concomitant Vaccine Administration under Actions]. Three percent of individuals received MMR and V, instead of MMRV, at 12 months of age.
The primary safety study was a controlled trial that enrolled 1256 children who received Menactra at 9 and 12 months of age. At 12 months of age these children received MMRV (or MMR+V), PCV7 and HepA. A control group of 522 children received MMRV, PCV7 and HepA. Of the 1778 children, 78% of participants (Menactra, N=1056; control group, N=322) were enrolled at United States (US) sites and 22% at a Chilean site. (Menactra, N=200; control group, N=200).
Individuals 2 Through 55 Years of Age: The safety of Menactra was evaluated in eight clinical studies that enrolled 10,057 participants aged 2-55 years who received Menactra and 5,266 participants who received Menomune - A/C/Y/W-135, Meningococcal Polysaccharide Vaccine, Groups A, C, Y and W-135 Combined. There were no substantive differences in demographic characteristics between the vaccine groups. Among Menactra recipients 2-55 years of age 24.0%, 16.2%, 40.4% and 19.4% were in the 2-10, 11-14, 15-25 and 26-55-year age groups, respectively. Among Menomune - A/C/Y/W-135 recipients 2-55 years of age 42.3%, 9.3%, 30.0% and 18.5% were in the 2-10, 11-14, 15-25 and 26-55-year age groups, respectively. The three primary safety studies were randomized, active controlled trials that enrolled participants 2-10 years of age (Menactra, N=1713; Menomune - A/C/Y/W-135, N=1519), 11-18 years of age (Menactra, N=2270; Menomune - A/C/Y/W-135, N=972) and 18-55 years of age (Menactra, N=1384; Menomune - A/C/Y/W-135, N=1170), respectively. Of the 3232 children 2-10 years of age, 68% of participants (Menactra, N=1164; Menomune - A/C/Y/W-135, N=1031) were enrolled at US sites and 32% (Menactra, N=549; Menomune - A/C/Y/W-135, N=488) of participants at a Chilean site. The median ages in the Chilean and US subpopulations were 5 and 6 years, respectively. All adolescents and adults were enrolled at US sites. As the route of administration differed for the two vaccines (Menactra given intramuscularly, Menomune - A/C/Y/W-135 given subcutaneously), study personnel collecting the safety data differed from personnel administering the vaccine.
Booster Vaccination Study: In an open-label trial conducted in the US, 834 individuals were enrolled to receive a single dose of Menactra 4-6 years after a prior dose. The median age of participants was 17.1 years at the time of the booster dose.
Safety Evaluation: Participants were monitored after each vaccination for 20 or 30 minutes for immediate reactions, depending on the study. Solicited injection site and systemic reactions were recorded in a diary card for 7 consecutive days after each vaccination. Participants were monitored for 28 days (30 days for infants and toddlers) for unsolicited adverse events and for 6 months post-vaccination for visits to an emergency room, unexpected visits to an office physician, and serious adverse events.
Unsolicited adverse event information was obtained either by telephone interview or at an interim clinic visit. Information regarding adverse events that occurred in the 6-month post-vaccination time period was obtained via a scripted telephone interview.
Serious Adverse Events in All Safety Studies: Serious adverse events (SAEs) were reported during a 6-month time period following vaccinations in individuals 9 months through 55 years of age. In children who received Menactra at 9 months and at 12 months of age, SAEs occurred at a rate of 2.0% - 2.5%. In participants who received one or more childhood vaccine(s) (without co-administration of Menactra) at 12 months of age, SAEs occurred at a rate of 1.6% - 3.6%, depending on the number and type of vaccines received. In children 2-10 years of age, SAEs occurred at a rate of 0.6% following Menactra and at a rate of 0.7% following Menomune - A/C/Y/W-135. In adolescents 11 through 18 years of age and adults 18 years through 55 years of age, SAEs occurred at a rate of 1.0% following Menactra and at a rate of 1.3% following Menomune - A/C/Y/W-135. In adolescents and adults, SAEs occurred at a rate of 1.3% following booster vaccination with Menactra.
Solicited Adverse Events in the Primary Safety Studies: The most frequently reported solicited injection site and systemic adverse reactions within 7 days following vaccination in children 9 months and 12 months of age (Table 5) were injection site tenderness and irritability.
The most frequently reported solicited injection site and systemic adverse reactions in US children 2 aged 2-10 years of age (Table 6) were injection site pain and irritability. Diarrhea, drowsiness, 3 and anorexia were also common.
The most commonly reported solicited injection site and systemic adverse reactions in adolescents, ages 11-18 years (Table 7), and adults, ages 18-55 years (Table 8), after a single dose were injection site pain, headache and fatigue. Except for redness in adults, injection site reactions were more frequently reported after Menactra vaccination than after Menomune - A/C/Y/W-135 vaccination. (See Tables 5, 6, 7 and 8.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Solicited Adverse Events in a Booster Vaccination Study:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Solicited Adverse Events in a Booster Vaccination Study: For a description of the study design and number of participants, [see Clinical Trials Experience, Booster Vaccination Study as previously mentioned]. The most common solicited injection site and systemic reactions within 7 days of vaccination were pain (60.2%) and myalgia (42.8%), respectively. Overall rates of solicited injection site reactions and solicited systemic reactions were similar to those observed in adolescents and adults after a single Menactra dose. The majority of solicited reactions were Grade 1 or 2 and resolved within 3 days.
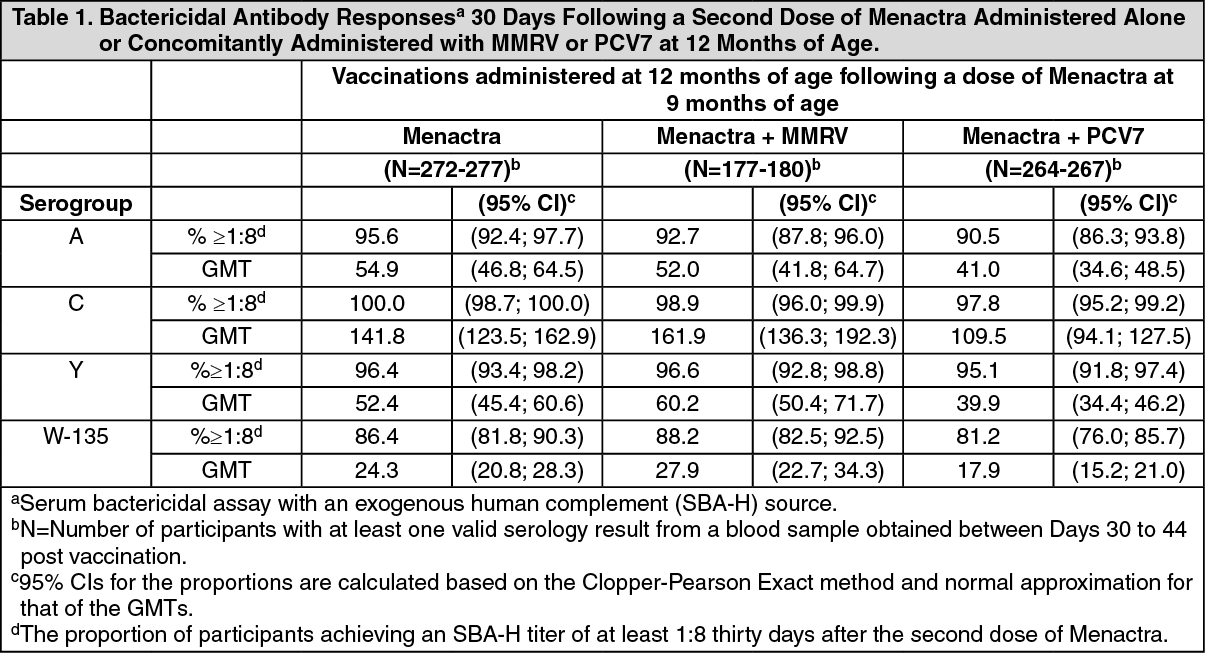
Adverse Events in Concomitant Vaccine Studies: Solicited Injection Site and Systemic Reactions when Given with Routine Pediatric Vaccines: For a description of the study design and number of participants, [see Clinical Trials Experience as previously mentioned, Pharmacology: Clinical Studies: Concomitant Vaccine Administration under Actions]. In the primary safety study, 1378 US children 19 were enrolled to receive Menactra alone at 9 months of age and Menactra plus one or more other 20 routinely administered vaccines (MMRV, PCV7 and HepA) at 12 months of age (N=961).
Another group of children received two or more routinely administered vaccines (MMRV, PCV7 and HepA) (control group, n=321) at 12 months of age. The frequency of occurrence of solicited adverse events is presented in Table 5. Participants who received Menactra and the concomitant vaccines at 12 months of age described above reported similar frequencies of tenderness, redness and swelling at the Menactra injection site and at the concomitant vaccine injection sites. Tenderness was the most frequent injection site reaction (48%, 39%, 46% and 43% at the Menactra, MMRV, PCV7 and HepA sites, respectively). Irritability was the most frequent systemic reaction, reported in 62% of recipients of Menactra plus concomitant vaccines, and 65% of the control group. [See Pharmacology: Clinical Studies: Concomitant Vaccine Administration under Actions.]
In a randomized, parallel group, US multi-center clinical trial conducted in children 4 through 6 years of age, Menactra was administered as follows: 30 days after concomitant DAPTACEL, Diphtheria and Tetanus Toxoids and Acellular Pertussis Vaccine Adsorbed, (DTaP), manufactured by Sanofi Pasteur Limited + IPOL, Poliovirus Vaccine Inactivated, (IPV), manufactured by Sanofi Pasteur SA [Group A]; concomitantly with DAPTACEL followed 30 days later by IPV [Group B]; concomitantly with IPV followed 30 days later by DAPTACEL [Group C]. Solicited injection site and systemic reactions were recorded in a diary card for 7 consecutive days after each vaccination. For all study groups, the most frequently reported solicited local reaction at the Menactra site was pain: 52.2%, 60.9% and 56.0% of participants in Groups A, B and C, respectively. For all study groups, the most frequently reported systemic reaction following the administration of Menactra alone or with the respective concomitant vaccines was myalgia: 24.2%, 37.3% and 26.7% of participants in Groups A, B and C, respectively. Fever >39.5ºC occurred at <1.0% in all groups. [See Pharmacology: Clinical Studies: Concomitant Vaccine Administration under Actions.]
Solicited Injection Site and Systemic Reactions when Given with Tetanus and Diphtheria: Toxoid Adsorbed Vaccine: In a clinical study, rates of local and systemic reactions after Menactra and Tetanus and Diphtheria Toxoid Adsorbed (Td) vaccine manufactured by Sanofi Pasteur Inc. were compared [see Interactions, and Pharmacology: Clinical Studies: Concomitant Vaccine Administration under Actions for study description]. Injection site pain was reported more frequently after Td vaccination than after Menactra vaccination (71% versus 53%). The overall rate of systemic adverse events was higher when Menactra and Td vaccines were given concomitantly than when Menactra was administered 28 days after Td vaccine (59% versus 36%). In both groups, the most common reactions were headache (Menactra + Td vaccine, 36%; Td vaccine + Placebo, 34%; Menactra alone, 22%) and fatigue (Menactra + Td vaccine, 32%; Td vaccine + Placebo, 29%; Menactra alone, 17%). Fever ≥40.0ºC occurred at ≤0.5% in all groups.
Solicited Injection Site and Systemic Reactions when Given with Typhoid Vi Polysaccharide: Vaccine: In a clinical study, rates of local and systemic reactions after Menactra and Typhim Vi [Typhoid Vi Polysaccharide Vaccine] (Typhoid), produced by Sanofi Pasteur SA were compared [see Interactions and Pharmacology: Clinical Studies: Concomitant Vaccine Administration under Actions)] for a description of the concomitantly administered vaccine, study design and number of participants. More participants experienced pain after Typhoid vaccination than after Menactra vaccination (Typhoid + Placebo, 76% versus Menactra + Typhoid, 47%). The majority (70%-77%) of injection site solicited reactions for both groups at either injection site were reported as Grade 1 and resolved within 3 days post-vaccination. In both groups, the most common systemic reaction was headache (Menactra + Typhoid, 41%; Typhoid + Placebo, 42%; Menactra alone, 33%) and fatigue (Menactra + Typhoid, 38%; Typhoid + Placebo, 35%; Menactra alone, 27%). Fever ≥40.0ºC and seizures were not reported in either group.
Post-Marketing Experience: In addition to reports in clinical trials, worldwide voluntary adverse events reports received since market introduction of Menactra are listed as follows. This list includes serious events and/or events which were included based on severity, frequency of reporting or a plausible causal connection to Menactra. Because these events were reported voluntarily from a population of uncertain size, it is not possible to reliably estimate their frequency or establish a causal relationship to vaccination.
Blood and Lymphatic System Disorders: Lymphadenopathy.
Immune System Disorders: Hypersensitivity reactions such as anaphylaxis/anaphylactic reaction, wheezing, difficulty breathing, upper airway swelling, urticaria, erythema, pruritus, hypotension.
Nervous System Disorders: Guillain-Barre syndrome, paraesthesia, vasovagal syncope, dizziness, convulsion, facial palsy, acute disseminated encephalomyelitis, transverse myelitis.
Musculoskeletal and Connective Tissue Disorders: Myalgia.
General Disorders and Administrative Site Conditions: Large injection site reactions, extensive swelling of the injected limb (may be associated with erythema, warmth, tenderness or pain at the injection site).
Post-marketing Safety Study: The risk of GBS following receipt of Menactra was evaluated in a US retrospective cohort study using healthcare claims data from 9,578,688 individuals 11 through 18 years of age, of whom 1,431,906 (15%) received Menactra. Of 72 medical chart-confirmed GBS cases, none had received Menactra within 42 days prior to symptom onset. An additional 129 potential cases of GBS could not be confirmed or excluded due to absent or insufficient medical chart information. In an analysis that took into account the missing data, estimates of the attributable risk of GBS ranged from 0 to 5 additional cases of GBS per 1,000,000 vaccinees within the 6-week period following vaccination.





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image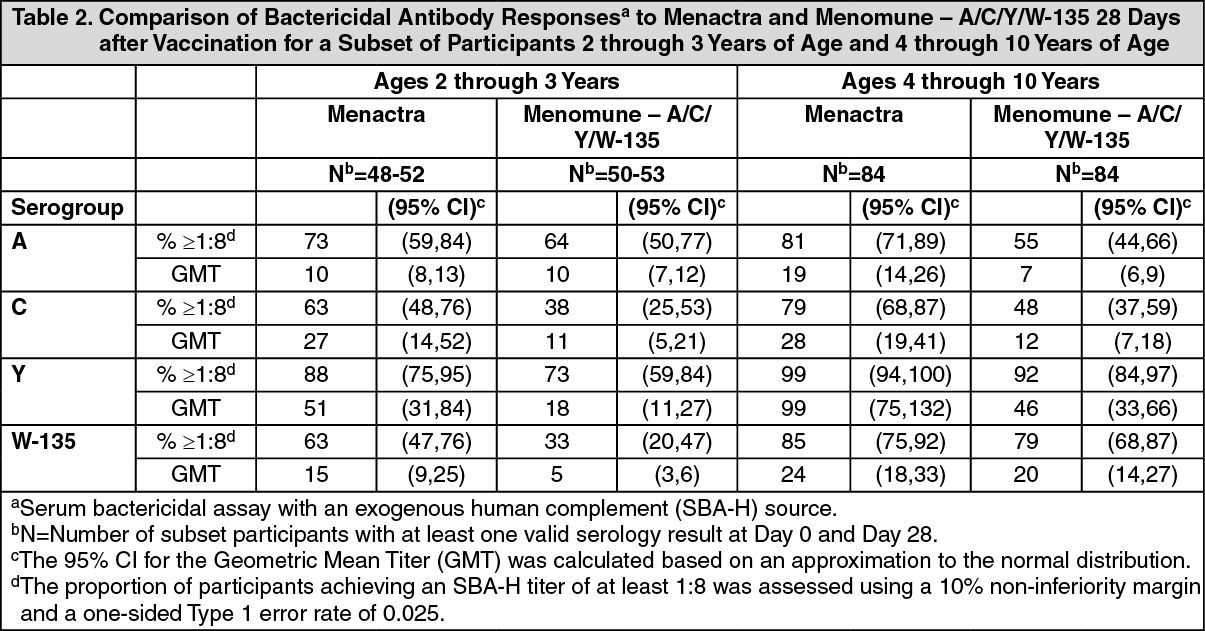 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image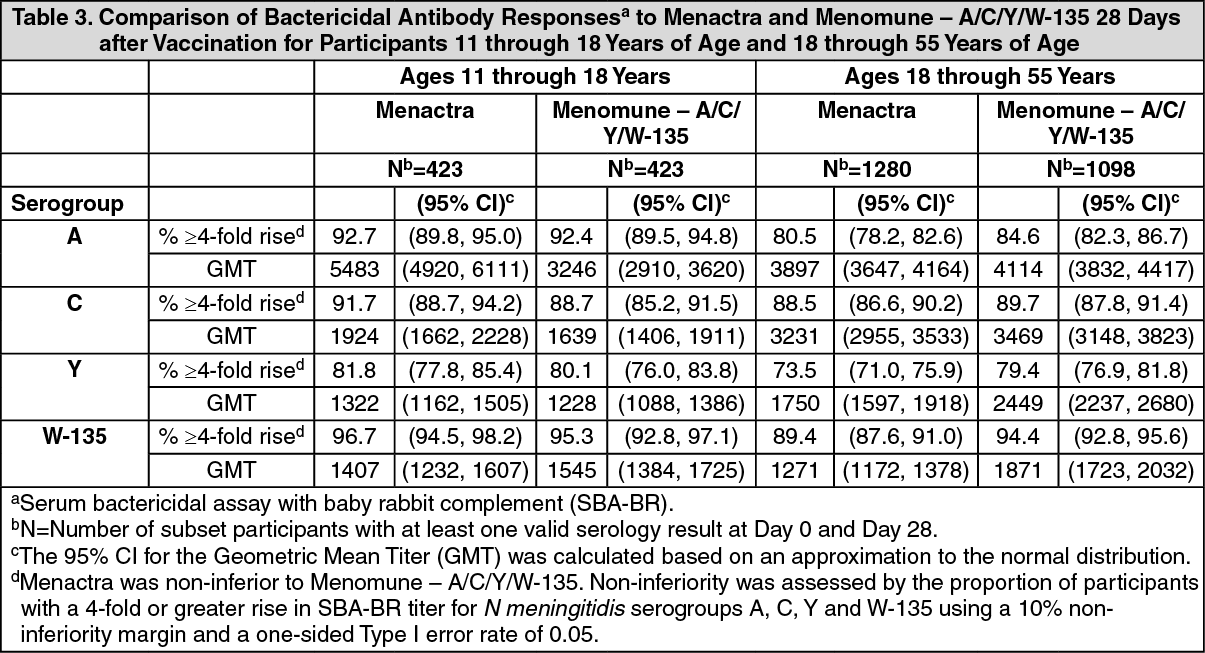 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image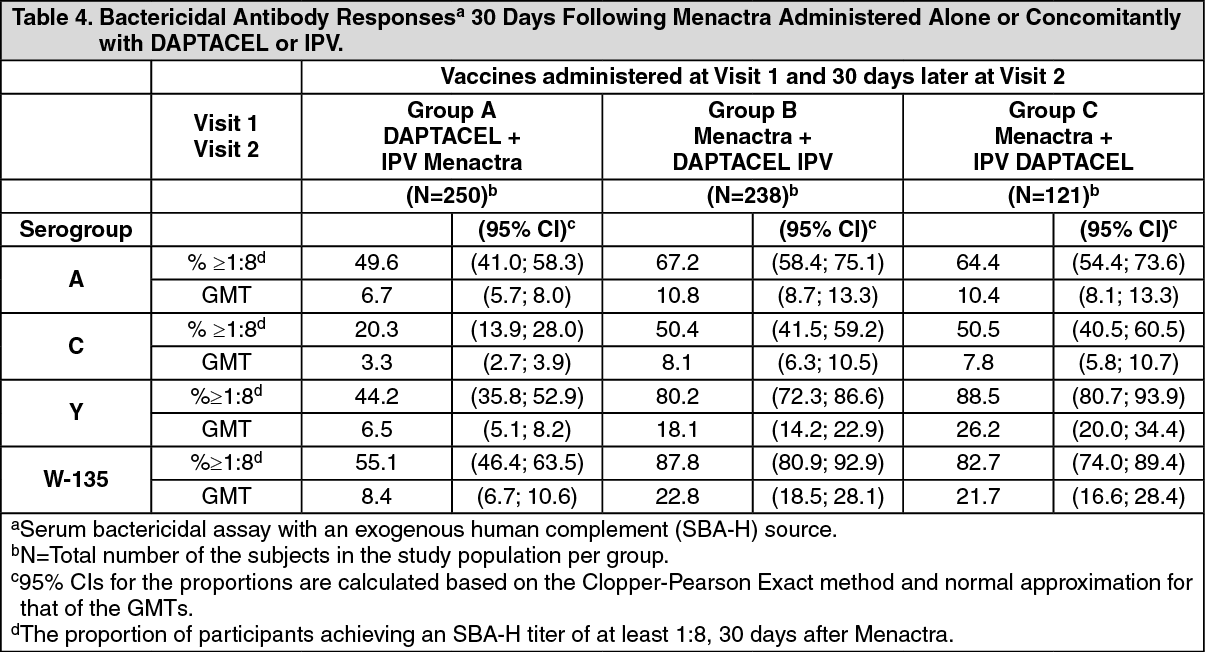 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image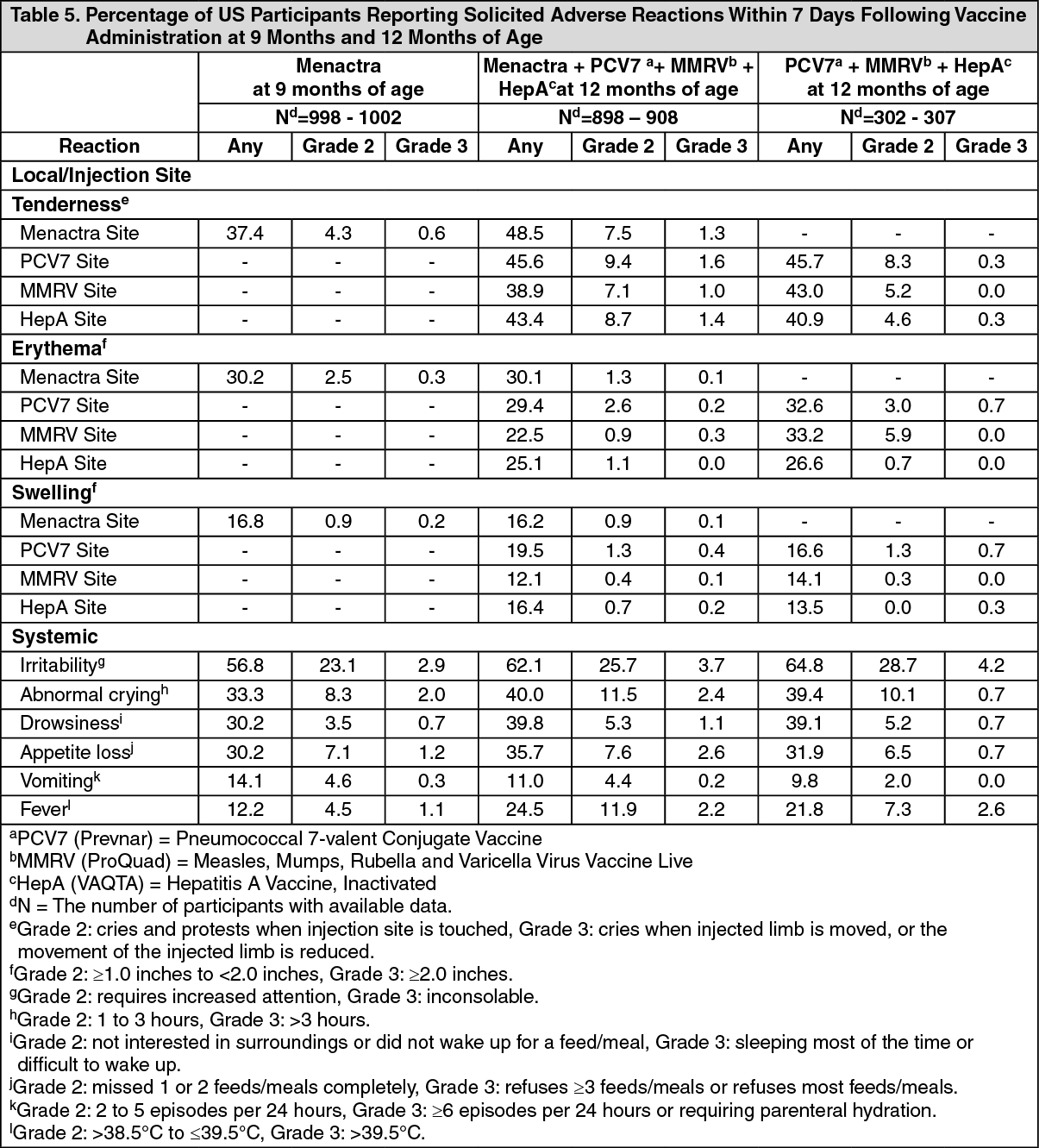 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image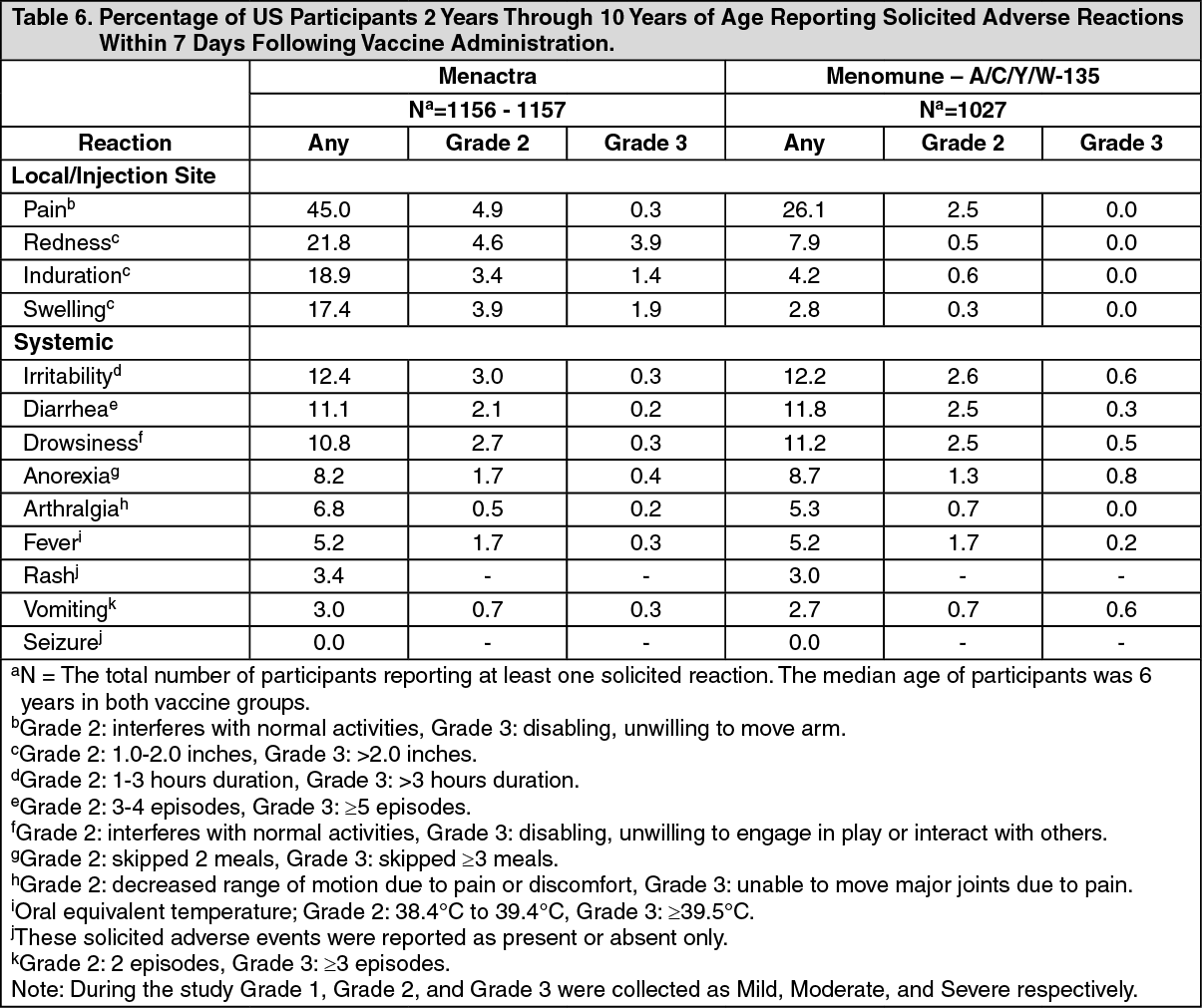 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image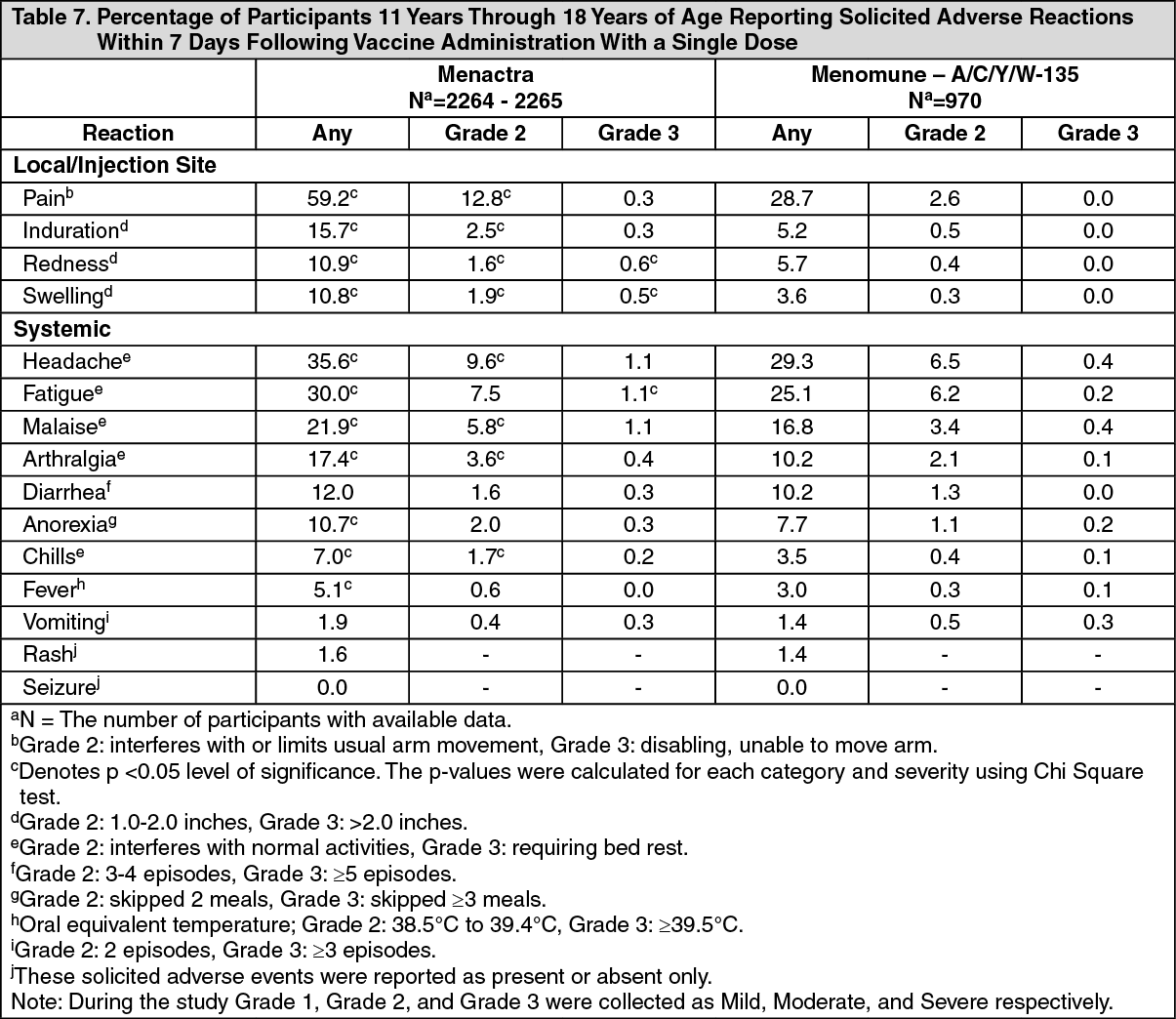 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image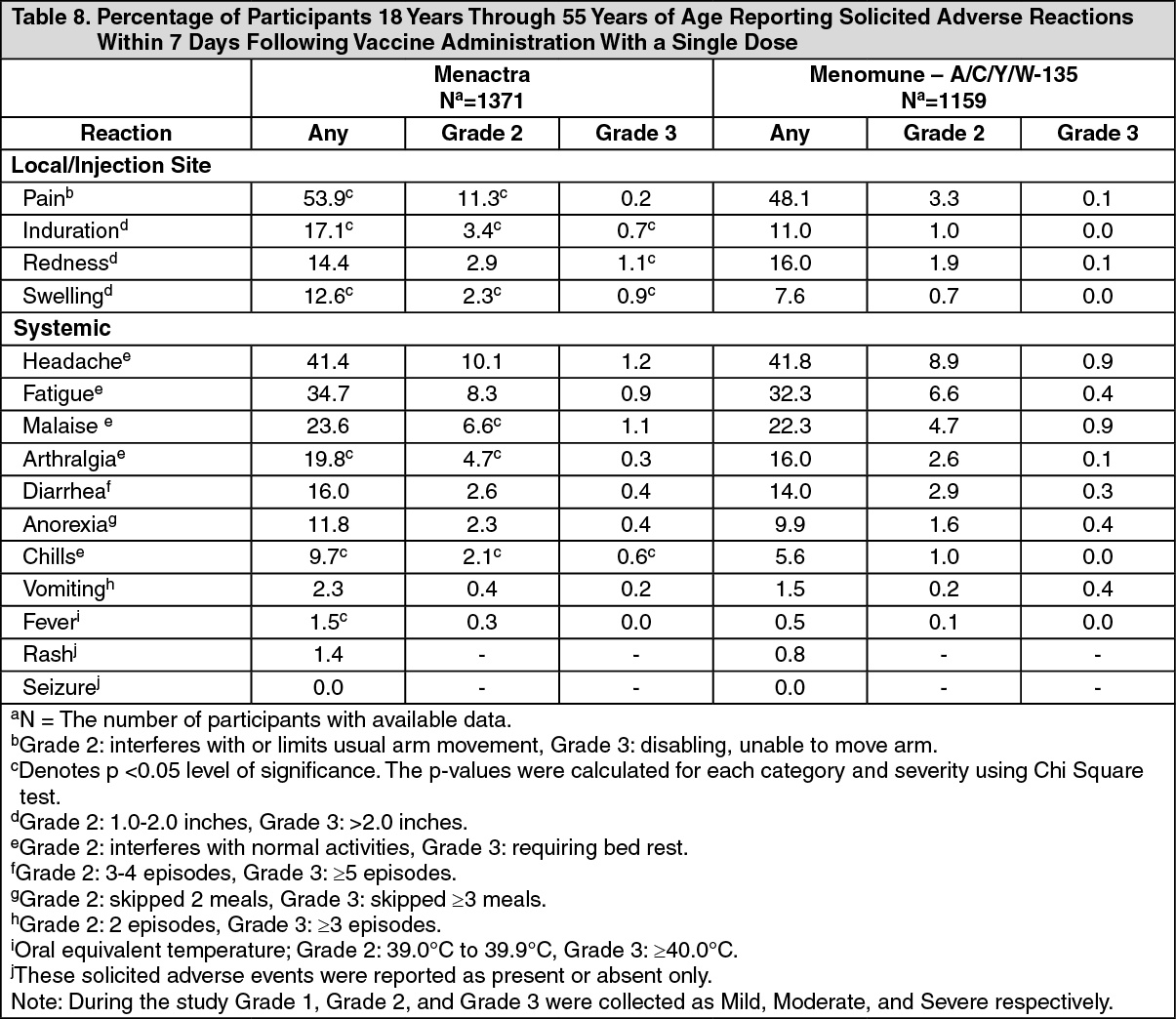 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out