


 Sign Out
Sign Out
Overview: Alcohol: Although citalopram hydrobromide did not potentiate the cognitive and psychomotor effects of alcohol in volunteers, the concomitant use of alcohol and citalopram hydrobromide should be avoided.
Cimetidine: Citalopram hydrobromide should not be dosed above 20 mg/day in patients receiving cimetidine.
CNS drugs: Drug interactions have not been specifically studied between citalopram and other centrally acting drugs. Given the primary CNS effects of citalopram, caution should be used as with other SSRIs when citalopram is taken in combination with other centrally acting drugs.
Cytochrome P450 Isozymes: Using in vitro models of human liver microsomes, the biotransformation of citalopram to its demethyl metabolites was shown to depend on both CYP2C19 and CYP3A4, with a small contribution from CYP2D6. Studies have also indicated that citalopram is a weak inhibitor of CYP2D6 and CYP2C19 and a weak or negligible inhibitor of CYP3A4, CYP1A2, CYP2C9 and CYP2E1. Although citalopram has a low potential for clinically significant drug interactions, caution is recommended, when citalopram is co-administered with drugs that are mainly metabolized by CYP2D6, and that have a narrow therapeutic index.
One in vitro study using human liver microsomes has shown that ketoconazole and omeprazole reduced the rate of formation of the demethylcitalopram metabolite of citalopram to 45-60% and 75-85% of control, respectively. As data are not available from multi-dose pharmacokinetic studies, the possibility that the clearance of citalopram will be decreased when citalopram hydrobromide is administered with a potent inhibitor of CYP3A4 (e.g., ketoconazole, itraconazole, fluconazole or erythromycin), or a potent inhibitor of CYP2C19 (e.g., omeprazole, esomeprazole, fluvoxamine, lansoprazole, ticlopidine), should be considered.
Citalopram 20 mg/day is the maximum recommended dose for patients taking concomitant CYP2C19 inhibitors because of the risk of QT prolongation.
In addition, a single-dose study of escitalopram co-administered with a multiple-dose regimen of cimetidine, a non-specific CYP inhibitor, led to significant changes in most of the pharmacokinetic parameters of escitalopram. The overall metabolic pathways for escitalopram and citalopram are qualitatively similar and the interaction potential for escitalopram is expected to closely resemble that of citalopram. Thus, this allows for extrapolation to previous studies with escitalopram.
Various scientific publications have acknowledged that the main components in grapefruit juice may act as a CYP3A4 inhibitor. Citalopram is also metabolized by other isoenzymes not affected by grapefruit juice, namely CYP2C19 and CYP2D6.
Drugs Affecting Platelet Function (e.g. NSAIDs, ASA and other anticoagulants): Serotonin release by platelets plays an important role in hemostasis. Epidemiological studies of the case-control and cohort design that have demonstrated an association between use of psychotropic drugs that interfere with serotonin reuptake and the occurrence of upper gastrointestinal bleeding have also shown that concurrent use of an NSAID, ASA or other anticoagulants may potentiate the risk of bleeding.
Altered anticoagulant effects, including increased bleeding, have been reported when SSRIs and SNRIs are co-administered with warfarin. Patients receiving warfarin therapy should be carefully monitored when citalopram is initiated or discontinued. (See Hematologic: Abnormal Bleeding under Precautions.)
Drugs That Prolong the QT Interval: ECG monitoring is recommended if citalopram hydrobromide is administered with concomitant medications that have demonstrated prolongation of the QT interval. (See Dosage & Administration; QT Prolongation under Contraindications; Cardiovascular: QT Prolongation and Torsades de Pointes under Precautions; Post-Market Adverse Drug Reactions under Adverse Reactions; Cimetidine and Cytochrome P450 Isozymes as previously mentioned.)
Drugs known to prolong the QT/QTc: The concomitant use of citalopram with another drug known to prolong the QT/QTc interval should be carefully considered to determine that the therapeutic benefit outweighs the potential risk. Drugs that have been associated with QT/QTc interval prolongation and/or torsade de pointes include, but are not limited to, the examples in the following list. Chemical/pharmacological classes are listed if some, although not necessarily all, class members have been implicated in QT/QTc prolongation and/or torsade de pointes: class IA antiarrhythmics (e.g., procainamide, disopyramide); class III antiarrhythmics (e.g., amiodarone, sotalol, ibutilide); class IC antiarrhythmics (e.g., propafenone); antipsychotics (e.g., chlorpromazine, pimozide, haloperidol, droperidol, ziprasidone); antidepressants (e.g., fluoxetine, venlafaxine, tricyclic/tetracyclic antidepressants e.g., amitriptyline, imipramine, maprotiline); opioids (e.g., methadone); macrolide antibiotics and analogues (e.g., erythromycin, clarithromycin, telithromycin, tacrolimus); quinolone antibiotics (e.g., moxifloxacin, levofloxacin, ciprofloxacin); antimalarials (e.g., quinine, chloroquine); azole antifungals (e.g., ketoconazole, fluconazole, voriconazole); domperidone; 5-hydroxytryptamine (5-HT)3 receptor antagonists (e.g., ondansetron); tyrosine kinase inhibitors (e.g., sunitinib, nilotinib, lapatinib); histone deacetylase inhibitors (e.g., vorinostat); beta-2 adrenoceptor agonists (e.g., salmeterol, formoterol).
The use of citalopram should be carefully considered with drugs that can disrupt electrolyte levels (see Precautions), including, but not limited to, the following: loop, thiazide, and related diuretics; laxatives and enemas; amphotericin B; high dose corticosteroids.
Monoamine Oxidase Inhibitors: In patients receiving SSRIs in combination with a monoamine oxidase inhibitor (MAOI), there have been reports of serious, sometimes fatal, reactions including hyperthermia, rigidity, myoclonus, autonomic instability with possible rapid fluctuations of vital signs, and mental status changes, including extreme agitation progressing to delirium and coma. These reactions have also been reported in patients who have recently discontinued SSRI treatment and have been started on a MAOI. Some cases presented with features resembling serotonin syndrome or neuroleptic malignant syndrome. Citalopram hydrobromide should not be used in combination with a MAOI, (including linezolid, an antibiotic which is a reversible non-selective MAO inhibitor and methylene blue, which is a MAOIs) or within 14 days of discontinuing treatment with a MAOI. Similarly, at least 14 days should elapse after discontinuing citalopram hydrobromide treatment before starting a MAOI (see Monoamine Oxidase Inhibitors under Contraindications).
Serotonergic Drugs: Based on the mechanism of action of citalopram and the potential for serotonin syndrome, caution is advised when citalopram hydrobromide is coadministered with other drugs or agents that may affect the serotonergic neurotransmitter systems, such as tryptophan, triptans, serotonin reuptake inhibitors, lithium, St. John's Wort, fentanyl and its analogues, dextromethorphan, tramadol, tapentadol, meperidine, methadone and pentazocine. (See Neurologic: Serotonin Syndrome/Neuroleptic Malignant Syndrome (NMS)-Like Events under Precautions.) Concomitant use of citalopram hydrobromide and MAO inhibitors (including linezolid and methylene blue), is contraindicated (see Monoamine Oxidase Inhibitors under Contraindications).
Triptans (5HT1 agonists): Cases of life-threatening serotonin syndrome have been reported during combined use of selective serotonin reuptake inhibitors (SSRIs)/serotonin norepinephrine reuptake inhibitors (SNRIs) and triptans. If concomitant treatment with citalopram hydrobromide and a triptan is clinically warranted, careful observation of the patient is advised, particularly during treatment initiation and dose increases (see Neurologic: Serotonin Syndrome/Neuroleptic Malignant Syndrome (NMS)-Like Events under Precautions).
Racemic Citalopram: pms-CITALOPRAM is a racemic mixture of R-citalopram and S-citalopram, the latter being the active isomer. As escitalopram, is the active isomer of racemic citalopram, the two drugs should not be taken together.
Other Drugs: No pharmacodynamic interactions have been noted in clinical trials where citalopram hydrobromide has been given concomitantly with benzodiazepines (anxiolytics/hypnotics), analgesics (NSAIDs, non-NSAIDs), antihistamines, antihypertensives or other cardiovascular drugs. Pharmacokinetic interactions between citalopram and these drugs were not specifically studied.
Drug-Drug Interactions: Where studies are described in this section, they were carried out in young, healthy, mostly male volunteers. In addition, some of the studies, namely interactions with metoprolol, warfarin, digoxin, imipramine, and levomepromazine, utilized only single doses of these drugs, although citalopram hydrobromide was given repeatedly to attain steady state. Thus, data are not available in patients who would be receiving these drugs on an ongoing basis at therapeutic doses. (See Tables 8a and 8b.)
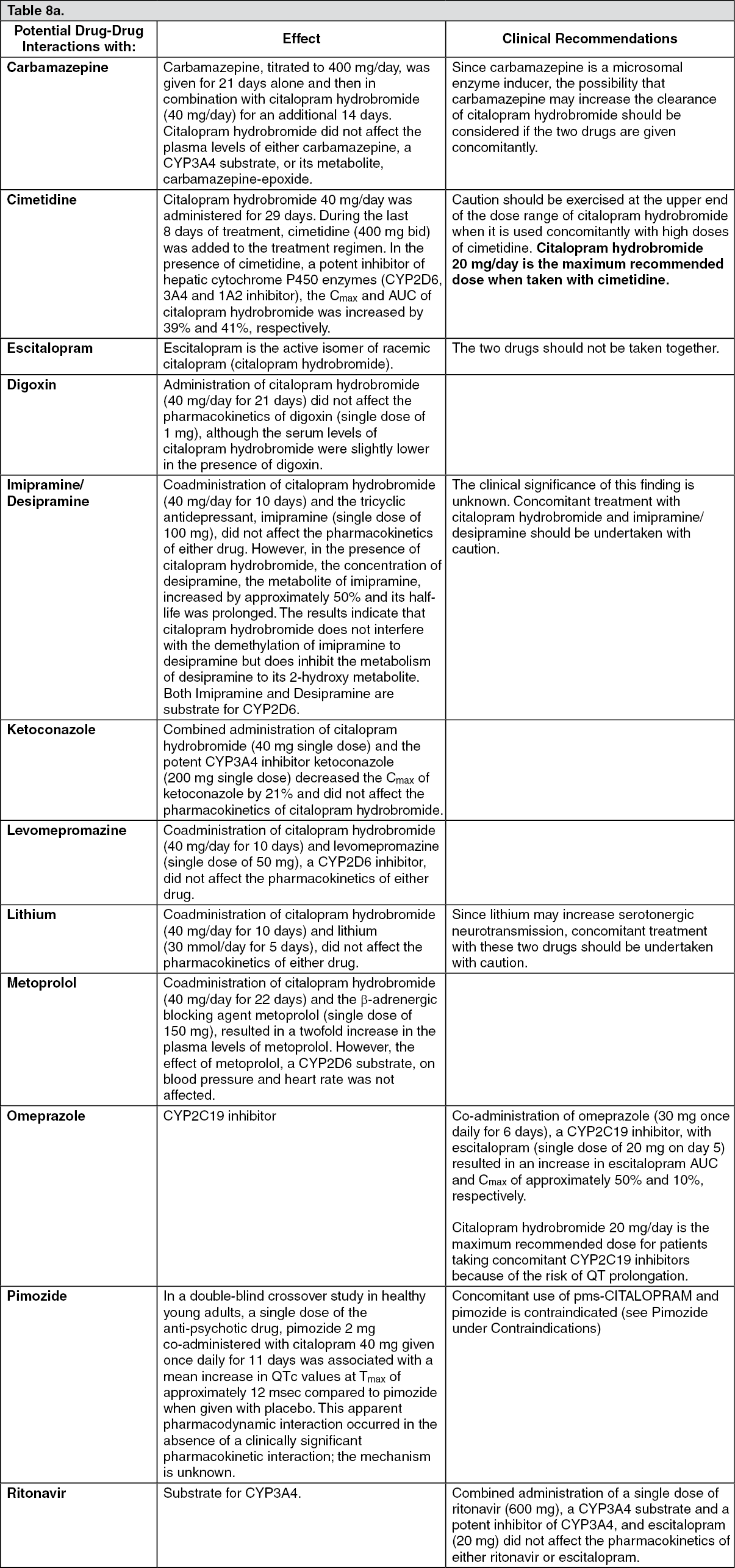 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image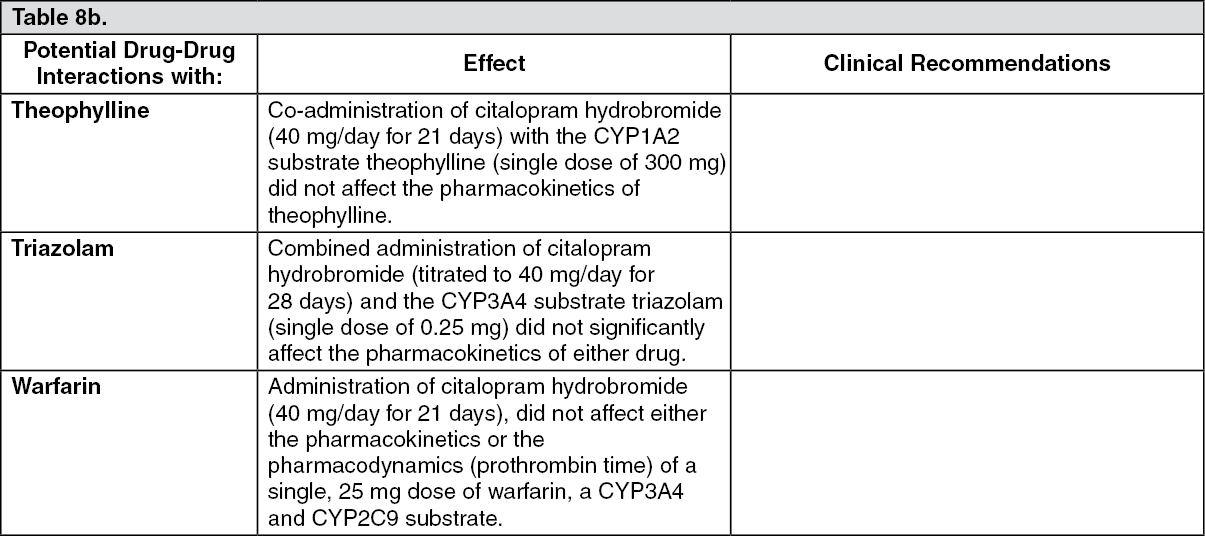 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDrug-Food Interactions: Although there is a theoretical possibility of pharmacokinetic drug product interactions resulting from co-administration of citalopram with grapefruit juice, the onset of an interaction is considered unlikely (see Overview: Cytochrome P450 Isozymes as previously mentioned).
Drug-Herb Interactions: St. John's Wort: In common with other SSRIs, pharmacodynamic interactions between citalopram and the herbal remedy St. John's Wort may occur and may result in undesirable effects.
Drug-Laboratory Interactions: Interactions with laboratory tests have not been established.