


 Sign Out
Sign Out
Angiotensin II is the primary vasoactive hormone in the renin-angiotensin system. Its effects include vasoconstriction and the stimulation of aldosterone secretion by the adrenal cortex.
Irbesartan blocks the vasoconstrictor and aldosterone-secreting effects of angiotensin II by selectively blocking in a non-competitive manner the binding of angiotensin II to the AT1 receptor found in many tissues. Irbesartan has no agonist activity at the AT1 receptor. AT2 receptors have been found in many tissues, but to date they have not been associated with cardiovascular homeostasis. Irbesartan has essentially no affinity for the AT2 receptors.
Irbesartan does not inhibit angiotensin-converting enzyme, also known as kinase II, the enzyme that converts angiotensin I to angiotensin II and degrades bradykinin, nor does it affect renin or other hormone receptors or ion channels involved in cardiovascular regulation of blood pressure and sodium homeostasis.
Pharmacodynamics: Healthy Subjects: Single oral doses of irbesartan ≤ 300 mg produced dose-dependent inhibition of the pressor effect of angiotensin II infusions. The inhibition was complete (100%) 4 hours following oral doses of 150 mg or 300 mg. Partial inhibition of 40% and 60% was still present 24 hours post-dose with 150 mg and 300 mg irbesartan respectively.
Hypertensive Patients: Angiotensin II receptor inhibition following chronic administration of irbesartan causes a 1.5 - 2-fold rise in angiotensin II plasma concentration and a 2 - 3-fold increase in plasma renin levels. Aldosterone plasma concentrations generally decline following irbesartan administration; however, at recommended dose, serum potassium levels are not significantly affected.
During clinical trials, minimal incremental blood pressure (BP) response was observed at doses > 300 mg.
The BP lowering effect of irbesartan was apparent after the first dose and substantially present within 1 - 2 weeks, with the maximal effect occurring by 4 - 6 weeks. In long-term studies, the effect of irbesartan appeared to be maintained for more than one year. In controlled trials, there was essentially no change in average heart rate in patients treated with irbesartan.
There was no rebound effect after withdrawal of irbesartan.
Race: Black hypertensive patients had a smaller BP response to irbesartan monotherapy than Caucasians.
Clinical Trials: Trial Design and Study Demographics: Two trials were done to investigate the effects of irbesartan in patients with hypertension and type 2 diabetic nephropathy, the IDNT and IRMA 2 trials.
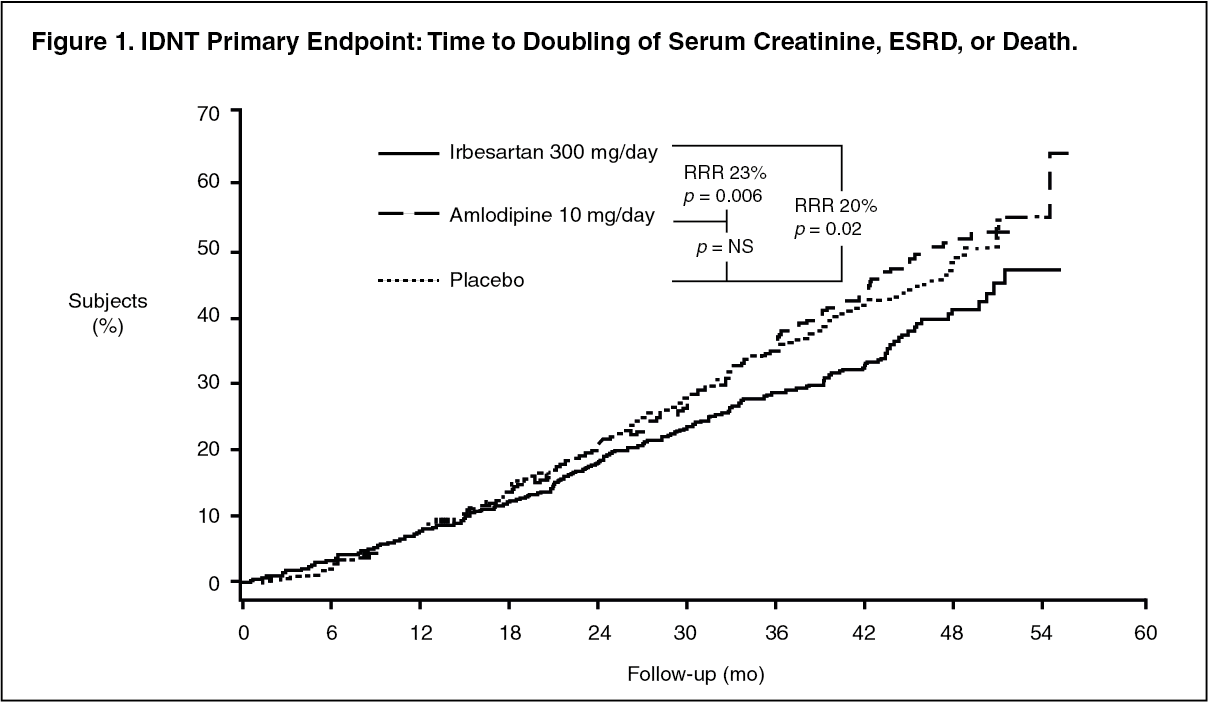
IDNT: The Irbesartan Diabetic Nephropathy Trial (IDNT) was a multicenter, randomized, controlled, double-blind, morbidity and mortality trial comparing irbesartan, amlodipine and placebo. In 1,715 hypertensive patients with type 2 diabetes (proteinuria ≥ 900 mg/day and serum creatinine 1.0 - 3.0 mg/dL) the long-term effects (mean 2.6 years) of irbesartan on the progression of renal disease and all-cause mortality were examined. In addition, as a secondary endpoint, the effect of irbesartan on the risk of fatal or non-fatal cardiovascular events was assessed. The most important exclusion criteria were: onset of type II diabetes mellitus at < 20 years of age, renovascular occlusive disease affecting both kidneys or a solitary kidney, and unstable angina pectoris.
Patients were randomized to receive once daily irbesartan 75 mg (n = 579), amlodipine 2.5 mg (n = 567), or matching placebo (n = 569). Patients were then titrated to a maintenance dose of 300 mg irbesartan, 10 mg amlodipine, or placebo as tolerated. Additional antihypertensive agents for the 3 study arms (excluding ACE inhibitors, other angiotensin II receptor blockers [ARBs] and calcium channel blockers [CCBs]) were added as needed to help achieve a BP goal of ≤ 135/85 mmHg in all groups, or a 10 mmHg reduction in systolic blood pressure (SBD) if baseline was > 160 mmHg. Of the total of 579 patients randomized to irbesartan, 442 completed the double-blind phase. All analyses were conducted on the intent to treat (ITT) patient population. (See Figure 1 and Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image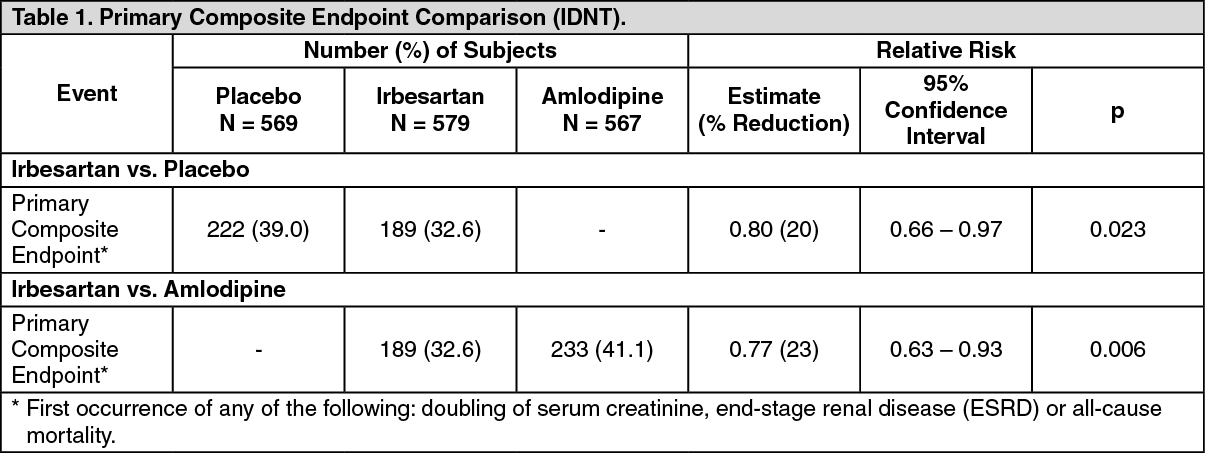 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIrbesartan demonstrated a 20% relative risk reduction (absolute risk reduction 6.4%) in the composite primary endpoint (1st occurrence of any of the following: doubling of serum creatinine, end-stage renal disease (ESRD) or all-cause mortality) compared to placebo (p=0.023), and a 23% relative risk reduction (absolute risk reduction 8.5%) compared to amlodipine (p=0.006). When the individual components of the primary composite endpoint were analysed, no effect in all-cause mortality and no significant effect on time to ESRD were observed. However, a significant reduction in doubling of serum creatinine was observed. Irbesartan decreased the progression of renal disease in patients with chronic renal insufficiency and overt proteinuria. Irbesartan also produced significant reduction in the rate of urine excretion of protein and albumin relative to placebo or amlodipine (p< 0.001 for both comparisons). Similar BP was achieved in the irbesartan 300 mg and amlodipine 10 mg groups.
Treatment with irbesartan reduced the occurrence of sustained doubling of serum creatinine as a separate endpoint (33%) with an absolute risk reduction of 6.8%.
The risk of developing a doubling of serum creatinine or ESRD was reduced by 26% relative to placebo with an absolute risk reduction of 6.2% and by 34% relative to amlodipine with an absolute risk reduction of 10.0% (pooled risk reduction 30%, p=0.0005). This renal protective effect of irbesartan appeared to be independent of systemic BP reduction.
There was no significant difference in the assessment of fatal or non-fatal cardiovascular events (cardiovascular death, non-fatal myocardial infarction, hospitalization for heart failure, permanent neurologic deficit attributed to stroke, or above-the-ankle amputation) among the 3 treatment groups.
Safety data from this trial are reported in Adverse Reactions.
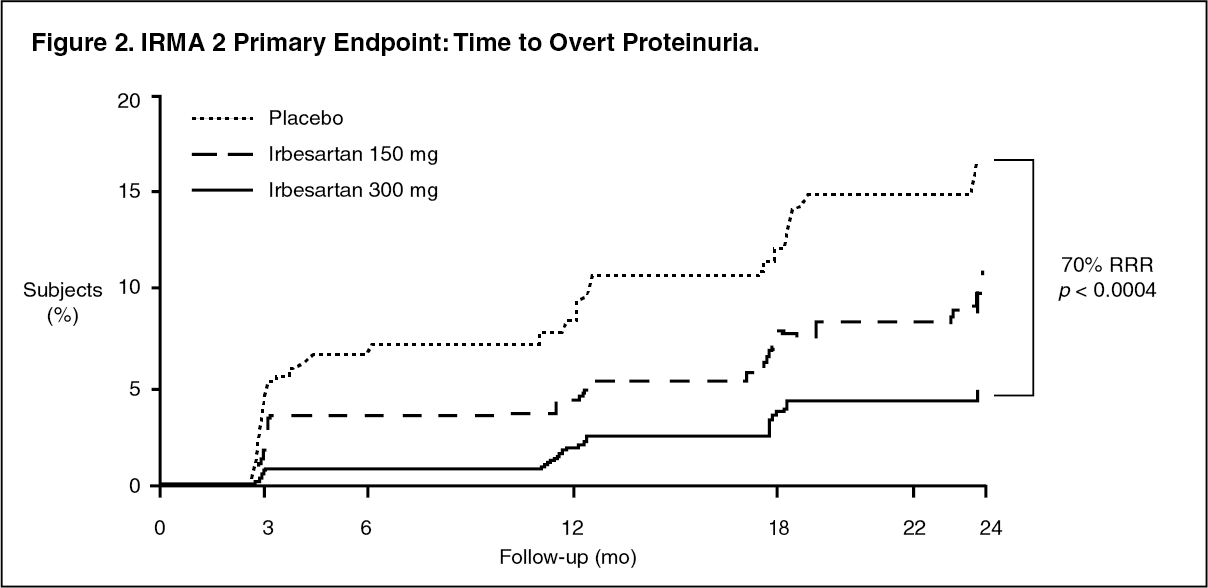
IRMA 2: The study of the Effects of Irbesartan on Microalbuminuria in Hypertensive Patients with Type 2 Diabetes Mellitus (IRMA 2) was a multicenter, randomized, placebo-controlled, double-blind morbidity study, conducted in 590 hypertensive patients with type 2 diabetes, microalbuminuria (20 - 200 mcg/min; 30 - 300 mg/day) and normal renal function (serum creatinine ≤ 1.5 mg/dL in males and ≤ 1.1 mg/dL in females). Screening of urine for albumin has revealed that patients with microalbuminuria have a 10 - 20-fold higher risk of developing diabetic nephropathy than patients with normoalbuminuria. Of the 590 patients, 201 received placebo, 195 received irbesartan 150 mg and 194 patients received irbesartan 300 mg.
The primary endpoint was the long-term effects (2 years) of irbesartan on the progression to clinical (overt) proteinuria (urinary albumin excretion rate [AER] > 200 mcg/min [> 300 mg/day] and an increase in AER of ≥ 30% from baseline). In addition, after 1 and 2 years of treatment, the effect of irbesartan on the change in overnight AER and the change in 24-hour creatinine clearance was assessed. The most important exclusion criteria were: onset of type II diabetes mellitus at < 20 years of age, renovascular occlusive disease affecting both kidneys or a solitary kidney, and unstable angina pectoris.
Irbesartan 300 mg demonstrated a 70% relative risk reduction (absolute risk reduction 9.8%) in the development of clinical (overt) proteinuria compared to placebo (p=0.0004). Relative risk reduction in the development of proteinuria with 150 mg irbesartan was not statistically significant. The slowing of progression to clinical (overt) proteinuria was evident as early as 3 months and continued over the 2-year period. (See Figure 2 and Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
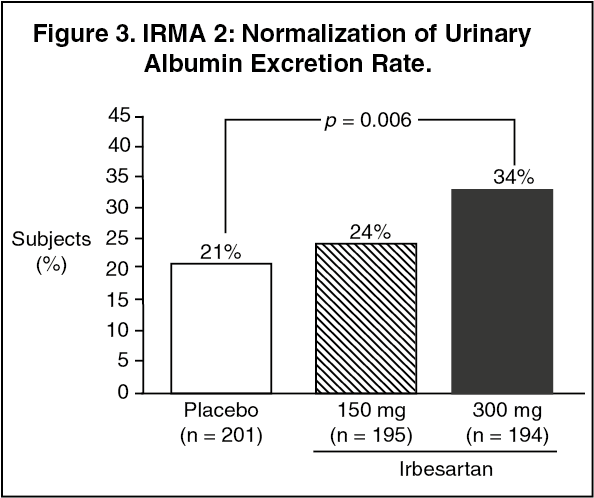
Click on icon to see table/diagram/imageRegression to normoalbuminuria (< 20 mcg/min; < 30 mg/day) was more frequent in the irbesartan 300 mg group (34%) than in the placebo group (21%). Irbesartan 300 mg reduced the level of urinary albumin excretion at 24 months by 43% (p = 0.0001). (See Figure 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSafety data from this trial has been reported in Adverse Reactions.
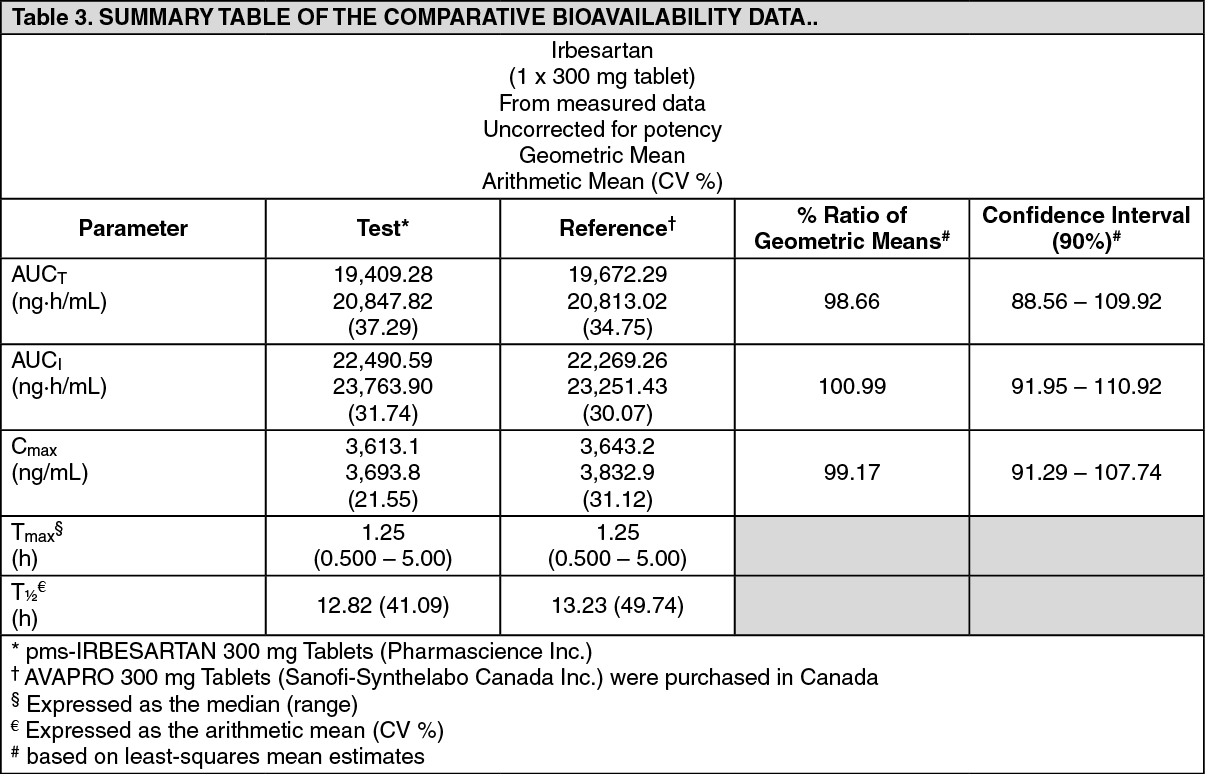
Comparative Bioavailability Studies: The objective of this study was to evaluate and compare the relative bioavailability and therefore the bioequivalence of two formulations of irbesartan tablets after a single oral dose administration under fasting conditions. The study was a single center, randomized, single dose, blinded, 2-way crossover study design performed in twenty-one healthy male subjects. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePharmacokinetics: Absorption: Irbesartan is an orally active agent. The oral absorption of irbesartan is rapid and complete with an average absolute bioavailability of 60%-80%. Irbesartan exhibits linear pharmacokinetics over the therapeutic dose range with an average terminal elimination half-life of 11 - 15 hours. Following oral administration, peak plasma concentrations are attained at 1.5 - 2 hours after dosing. Steady-state concentrations are achieved within 3 days.
Distribution: Irbesartan is approximately 96% protein-bound in the plasma, primarily to albumin and α1-acid glycoprotein.
The average volume of distribution of irbesartan is 53 - 93 L. Total plasma and renal clearances are in the range of 157 - 176 mL/min and 3.0 - 3.5 mL/minute, respectively.
Metabolism: Irbesartan is metabolized via glucuronide conjugation, and oxidation primarily by the cytochrome P-450 isoenzyme CYP 2C9. Metabolism of irbesartan by CYP 3A4 is negligible. In addition, irbesartan is not metabolized by the following isoenzymes: CYP 1A1, 1A2, 2A6, 2B6, 2D6, 2E1.
Following either oral or intravenous administration of 14C-labeled irbesartan, more than 80% of the circulating plasma radioactivity is attributable to unchanged irbesartan. The primary circulating metabolite is the inactive irbesartan glucuronide (approximately 6%). The remaining oxidative metabolites do not add appreciably to the pharmacologic activity.
Elimination: Irbesartan and its metabolites are excreted by both biliary and renal routes. Following either oral or intravenous administration of 14C-labeled irbesartan, about 20% of radioactivity is recovered in the urine and the remainder in the feces. Less than 2% of the dose is excreted in urine as unchanged irbesartan.
Special Populations and Conditions: Geriatrics: In subjects > 65 years of age, irbesartan elimination half-life was not significantly altered, but AUC and Cmax values were about 20 - 50% greater than those of young subjects.
Hepatic Insufficiency: The pharmacokinetics of irbesartan following repeated oral administration were not significantly affected in patients with mild to moderate cirrhosis of the liver. No data is available in patients with severe liver disease.
Renal Insufficiency: The mean AUC and Cmax were not altered in patients with any degree of renal impairment, including patients on hemodialysis. However, a wide variance was seen in patients with severe renal impairment.
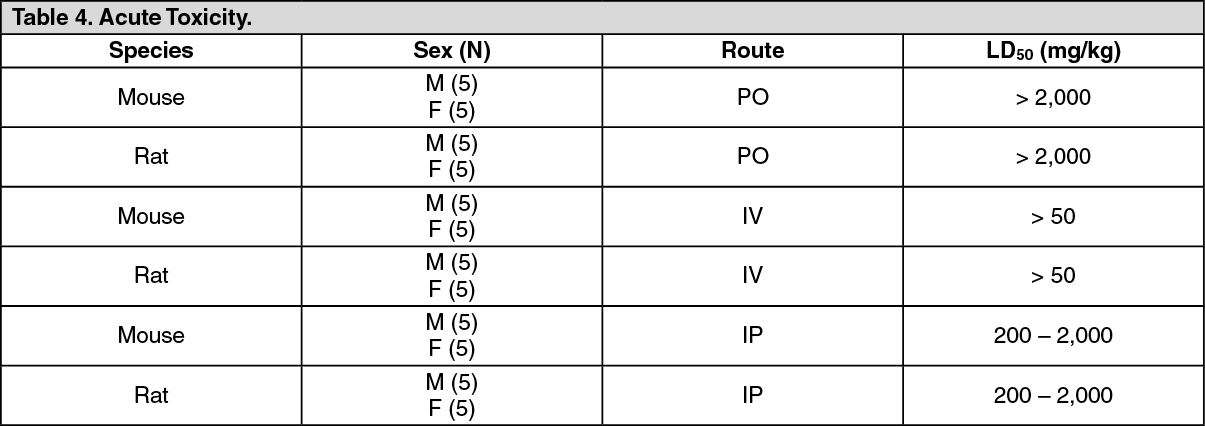
Toxicology: Non-clinical Toxicology: Acute Toxicity: See Table 4.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAfter single administration, toxicity was slight, and no target organ was identified. Very few toxic effects, characterized by pilo-erection and/or somnolence were noted at 2,000 mg/kg by the oral route, 200 mg/kg by the intraperitoneal route and 50 mg/kg by the intravenous route. Acute oral toxicity studies with irbesartan in mice and rats indicated acute lethal doses were in excess of 2,000 mg/kg, about 25 - 50-fold the maximum human dose (300 mg) on a mg/m2 basis, respectively.
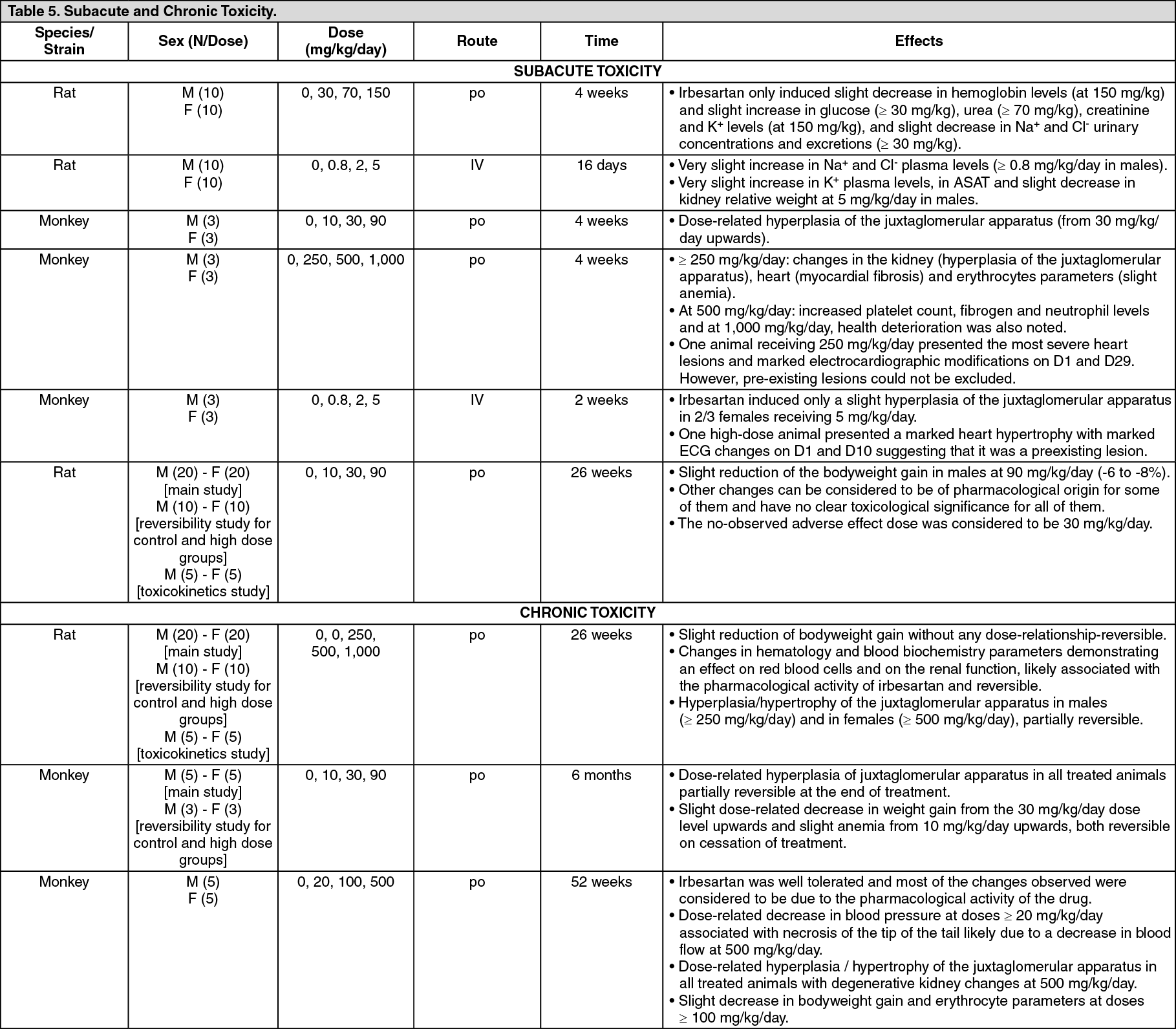
Subacute and Chronic Toxicity: See Table 5.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAfter repeated oral administrations at dose levels up to 1,000 mg/kg per day, most of the treatment-related effects noted in all species are linked to the pharmacological activity of irbesartan. The kidney can be considered as the primary target organ: hyperplasia/hypertrophy of the juxtaglomerular apparatus, which was observed in all species, is a direct consequence of the interaction with the renin-angiotensin system. Irbesartan also induced some hematology (slight decrease in erythrocyte parameters) and blood biochemistry variations (slight increase in urea, creatinine, phosphorus, potassium and calcium levels) likely due to a disturbance in the renal blood flow, and a slight decrease in heart weight which could result from a decrease in cardiac work load due to decreased peripheral vascular resistance. At high doses (> 500 mg/kg per day), degenerative changes of the kidney were noted which could be secondary to prolonged hypotensive effects.
Reproduction and Teratology: Fertility and reproductive performance were not affected in studies of male and female rats even at oral doses of irbesartan causing pronounced toxicity (up to 650 mg/kg/day). No significant effects on the number of corpora lutea, implants, or live fetuses were observed. Irbesartan did not affect survival, development, or reproduction of offspring except for a slight decrease of body weight gain during lactation which was reversible after weaning.
In a study of rats receiving maternally toxic doses of irbesartan (650 mg/kg/day), transient effects were observed in fetuses. These effects included increased incidences of renal pelvic cavitation at doses ≥ 50 mg/kg/day and subcutaneous edema at doses ≥ 180 mg/kg/day. Slight decreases in body weight gain were noted (prior to weaning) in offspring of females receiving irbesartan at doses ≥ 50 mg/kg/day. In rabbits, maternally toxic doses of irbesartan (30 mg/kg/day) were associated with maternal mortality and abortion. Surviving females receiving this dose had a slight increase in early resorption. However, no teratogenic effect was observed. Radioactivity was present in the rat and rabbit fetus during late gestation and in rat milk following oral doses of radiolabeled irbesartan. These findings are attributed to drug exposure in late gestation and during lactation.
Carcinogenicity and Mutagenicity: No evidence of carcinogenicity was observed when irbesartan was administered at doses of up to 500/1,000 mg/kg/day (males/females, respectively) in rats and 1,000 mg/kg/day in mice for 2 years. These doses provided systemic exposures of 3.6 - 24.9 times (rats) and 3.8 - 6.2 times (mice) the exposures in humans receiving 300 mg daily.
Irbesartan was not mutagenic in a battery of in vitro tests (Ames microbial test, rat hepatocyte DNA repair test, V79 mammalian cell forward gene mutation assay). Irbesartan was negative in several tests for induction of chromosomal aberrations (in vitro human lymphocyte assay; in vivo mouse micronucleus study).
Microbiology: No microbiological information is required for this drug product.