


 Sign Out
Sign Out

Posology: The dose and dose regimen is dependent on the indication.
In replacement therapy, the dose may need to be individualised for each patient depending on the clinical response. Dose based on body weight may require adjustment in underweight or overweight patients. The following dose regimens are given as a guideline.
Replacement therapy in primary immunodeficiency (PID) syndromes: The dose regimen should achieve a trough IgG level (measured before the next infusion) of at least 6 g/l or within the normal reference range for the population age. Three to six months are required after the initiation of therapy for equilibration to occur. The recommended starting dose is 0.4 to 0.8 g/kg body weight (bw) given once, followed by at least 0.2 g/kg bw every 3 to 4 weeks.
The dose required to achieve a trough level of IgG of 6 g/l is of the order of 0.2 to 0.8 g/kg bw/month. The dosage interval when steady state has been reached varies from 3 to 4 weeks.
IgG trough levels should be measured and assessed in conjunction with the incidence of infection. To reduce the rate of bacterial infections, it may be necessary to increase the dosage and aim for higher trough levels.
Secondary immunodeficiencies (as defined in Indications/Uses): The dose regimen should achieve a trough IgG level (measured before the next infusion) of at least 6 g/l or within the normal reference range for the population age. The recommended dose is 0.2-0.4 g/kg bw every three to four weeks.
IgG trough levels should be measured and assessed in conjunction with the incidence of infection. Dose should be adjusted as necessary to achieve optimal protection against infections, an increase may be necessary in patients with persisting infection; a dose decrease can be considered when the patient remains infection free.
Primary immune thrombocytopenia (ITP): There are two alternative treatment schedules: 0.8 to 1 g/kg bw given on day 1 - this dose may be repeated once within 3 days; 0.4 g/kg bw given daily for 2 to 5 days.
The treatment can be repeated if relapse occurs.
Guillain-Barré syndrome: 0.4 g/kg bw/day over 5 days (possible repeat of dosing in case of relapse).
Kawasaki disease: 2.0 g/kg bw should be administered as a single dose.
Patients should receive concomitant treatment with acetylsalicylic acid.
Chronic inflammatory demyelinating polyneuropathy (CIDP)*: The recommended starting dose is 2 g/kg bw divided over 2 to 5 consecutive days followed by maintenance doses of 1 g/kg bw over 1 to 2 consecutive days every 3 weeks.
The treatment effect should be evaluated after each cycle; if no treatment effect is seen after 6 months, the treatment should be discontinued.
If the treatment is effective, long-term treatment should be subject to the physician's discretion based upon the patient response and maintenance response. The dosing and intervals may have to be adapted according to the individual course of the disease.
Multifocal Motor Neuropathy (MMN): Starting dose: 2 g/kg given over 2-5 consecutive days.
Maintenance dose: 1 g/kg every 2 to 4 weeks or 2 g/kg every 4 to 8 weeks.
The treatment effect should be evaluated after each cycle. If insufficient treatment effect is seen after 6 months, the treatment should be discontinued.
If the treatment is effective, long-term treatment should be subject to the physician's discretion based upon the patient response. The dosing and intervals may have to be adapted according to the individual course of the disease.
The dosage recommendations are summarised in the following table: See Table 3.
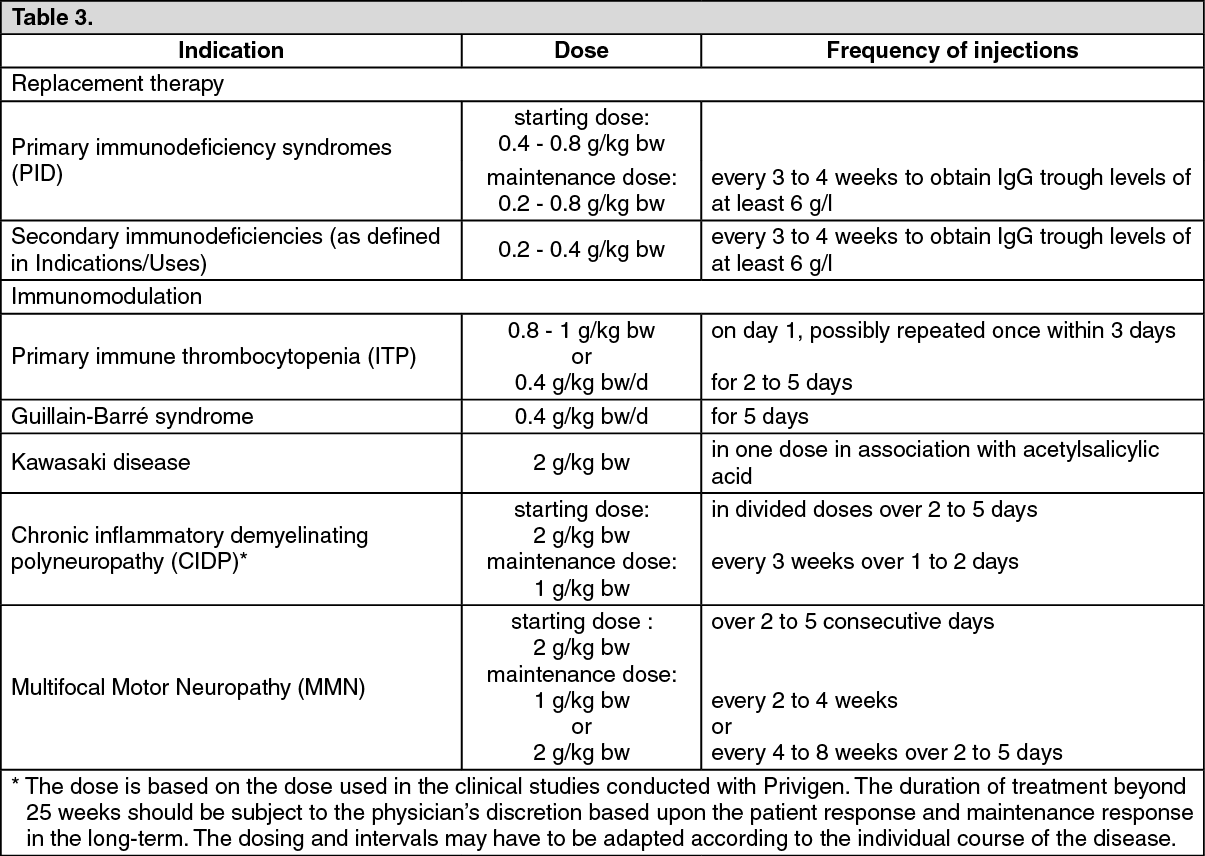 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imagePaediatric population: The posology in children and adolescents (0-18 years) is not different from that of adults as the posology for each indication is given by body weight and adjusted to the clinical outcome of the previously mentioned conditions.
Hepatic impairment: No evidence is available to require a dose adjustment.
Renal impairment: No dose adjustment unless clinically warranted, see Precautions.
Elderly: No dose adjustment unless clinically warranted, see Precautions.
Method of administration: For intravenous use.
Privigen should be infused intravenously at an initial infusion rate of 0.3 ml/kg bw/hr for approximately 30 min. If well tolerated (see Precautions), the rate of administration may gradually be increased to 4.8 ml/kg bw/hr.
In PID patients who have tolerated the infusion rate of 4.8 ml/kg bw/hr well, the rate may be further gradually increased to a maximum of 7.2 ml/kg bw/hr.
If dilution prior to infusion is desired, Privigen may be diluted with 5% glucose solution to a final concentration of 50 mg/ml (5%). For instruction, see Special precautions for disposal and other handling under Cautions for Usage.