


 Sign Out
Sign Out




Short-term and long-term, Placebo-controlled Trials of Adult Patients with Schizophrenia: The following findings are based on two 6-week, placebo-controlled, fixed-dose clinical trials, and one long-term 52-week double-blind placebo-controlled randomized-withdrawal trial for schizophrenia in which REXULTI was administered at daily doses between 1 mg and 4 mg. These are referred to as Trials 1, 2 and 3 respectively. In Trials 1 and 2, 852 patients received REXULTI at fixed daily doses of 1, 2 or 4 mg and 368 patients received placebo. In Trial 3, following an open-label stabilization period of up to 36 weeks, 97 patients received REXULTI at flexible daily doses between 1 and 4 mg and 104 patients received placebo in the double-blind randomized-withdrawal period; the mean daily REXULTI dose was 3.6 mg at the last visit in the study. This trial was terminated after efficacy was demonstrated in an interim analysis, and only 23 patients (11%), 14 in the REXULTI group and 9 in the placebo group, completed the 52 weeks of the double-blind, controlled period.
Safety data is also available for 1265 patients who participated in uncontrolled, open-label studies and received REXULTI daily doses from 1 mg to 4 mg; 604 patients completed at least 26 weeks and 372 completed at least 52 weeks in the open-label studies.
Most Common Adverse Events: There are no common adverse events that meet the criteria incidence of ≥5% and at least twice the rate of placebo in the Trials 1 and 2, the 6-week, placebo-controlled, fixed-dose trials, or Trial 3, during the double-blind randomized-withdrawal period.
Adverse Events Reported as Reasons for Discontinuation of Treatment: A total of 7.8% (67/852) REXULTI-treated subjects and 14.7% (54/368) of placebo-treated subjects discontinued due to adverse events. There were no adverse events associated with discontinuation in subjects treated with REXULTI that were at least 2% and at least twice the placebo rate.
Treatment-emergent adverse events (TEAEs) associated with REXULTI (incidence of 2% or greater and REXULTI incidence greater than placebo) that occurred during acute therapy (up to 6 weeks in subjects with schizophrenia) are shown in Table 5. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the longer-term randomized-withdrawal Trial 3, the general treatment-emergent adverse event profile for the initial 12- to 36-week single-blind REXULTI treatment phase of this study was comparable to the one characterised in the 6-week, placebo-controlled, fixed-dose studies 1 and 2 described previously. In the double-blind, randomized-withdrawal phase of the study, there was only one potentially drug-related adverse event that occurred at a rate greater than 2% and double that of placebo (tremor 3%). No additional safety concerns were noted, however, the exposure in the double-blind phase was limited (97 in REXULTI and 104 in placebo, about 40% overall completed at least 6 months, and 11% overall completed the 52 weeks).
Short-term Placebo-Controlled Clinical Trials in Adult Patients Receiving REXULTI as Adjunctive Treatment in Major Depressive Disorder (MDD): The following findings are based on four phase 3, 6-week, placebo-controlled trials (331-10-228, 331-10-227, 331-13-214, 331-12-282), three of which were fixed-dose and one which was flexible-dose with an active reference. These are referred to as Trials 4, 5, 6 and 7 respectively. In total 1032 patients were treated with REXULTI in the 6-week trials. In Trials 4, 5 and 6, 835 patients received REXULTI at fixed daily doses of 1, 2 or 3 mg and 613 patients received placebo, added to their current antidepressant therapy (ADT). In Trial 7, 197 patients received REXULTI at flexible daily doses of 2 to 3 mg + ADT, 100 patients received an active reference + ADT, and 206 patients received placebo + ADT. In Trial 7 the mean daily REXULTI dose was 2.2 mg at the last visit in the study.
Safety data are also available for 2240 patients who participated in uncontrolled, open-label studies and received REXULTI daily doses from 1 mg to 3 mg with ADT; 1304 patients completed at least 26 weeks and 1002 completed at least 52 weeks in the open-label studies.
Most Common Adverse Events: The most common adverse events (incidence of ≥ 5% in the REXULTI + ADT group and at least twice the rate of placebo + ADT) during short-term and long-term studies were akathisia and weight increased.
Adverse Events Reported as Reasons for Discontinuation of Treatment: In the 6-week studies a total of 2.4% (37/1520) REXULTI+ADT-treated subjects and 0.7% (8/1132) of placebo+ADT-treated subjects discontinued due to adverse events. There were no adverse event associated with discontinuation in subjects treated with REXULTI + ADT that were at least 2% and at least twice the placebo + ADT rate.
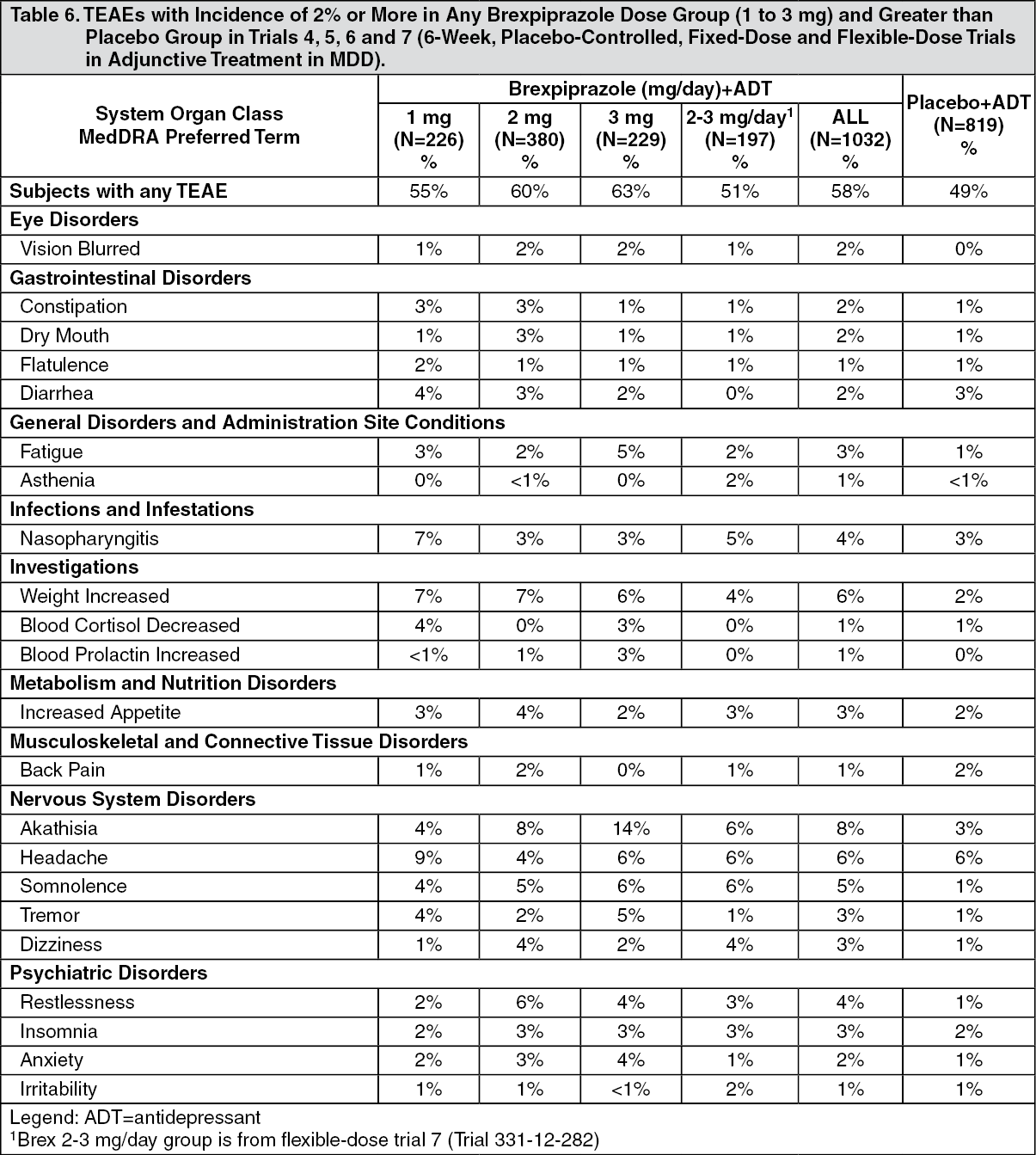
Treatment emergent adverse events associated with the use of REXULTI + ADT (incidence of 2% or greater and REXULTI + ADT incidence greater than adjunctive placebo + ADT) that occurred during acute therapy (6 weeks in patients with MDD) in fixed- and flexible-dose trials are shown in Table 6. (See Table 6.)
 Click on icon to see table/diagram/image
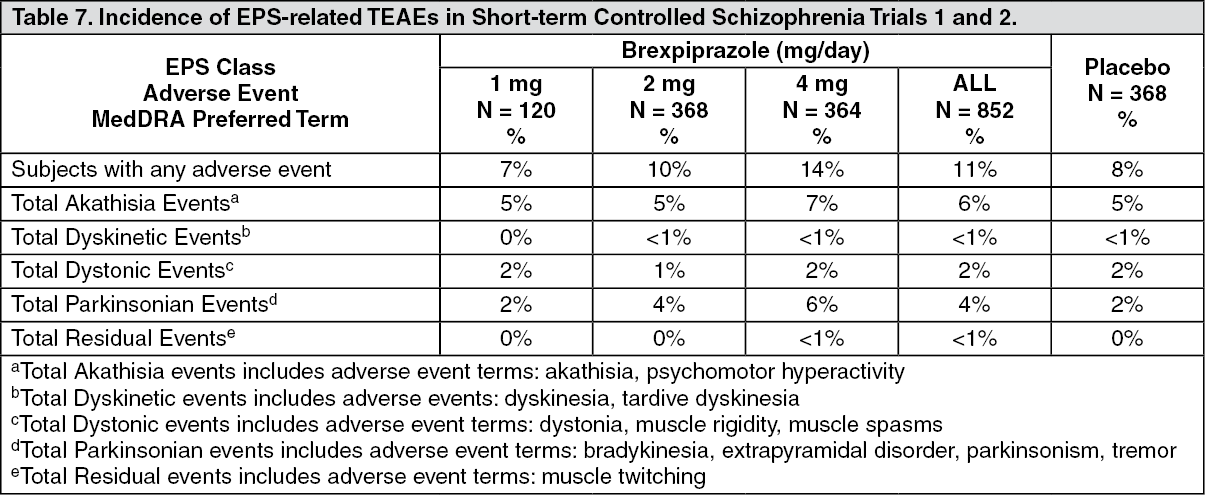
Click on icon to see table/diagram/imageSelected Adverse Events: Extrapyramidal Symptoms: Schizophrenia: In Trials 1 and 2, the incidence of reported EPS-related events, excluding akathisia events, was 5.1% versus 3.5% for placebo-treated subjects. The incidence of akathisia events for REXULTI-treated subjects was 5.4% versus 4.9% for placebo-treated subjects. Akathisia was reported more often during Weeks 1 through 3 and was mild to moderate in severity. The incidence of EPS-related TEAEs is presented in Table 7. (See Table 7.)
 Click on icon to see table/diagram/image
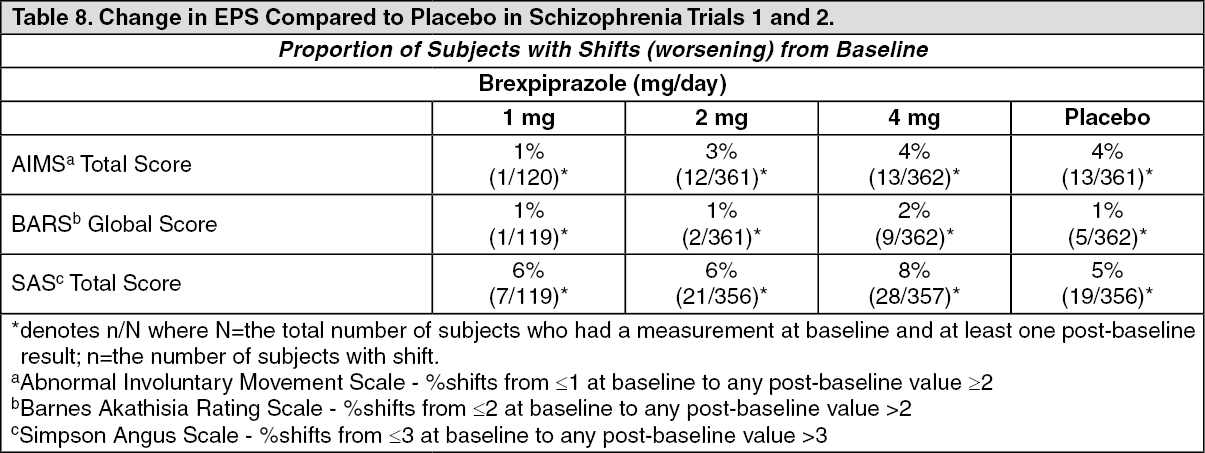
Click on icon to see table/diagram/imageIn Trials 1 and 2, data was objectively collected on the Simpson Angus Rating Score (SAS) for extrapyramidal symptoms (EPS), the Barnes Akathisia Global Score (BARS) for akathisia and the Abnormal Involuntary Movement Score (AIMS) for dyskinesia. The incidence of EPS change is presented in Table 8. (See Table 8.)
 Click on icon to see table/diagram/image
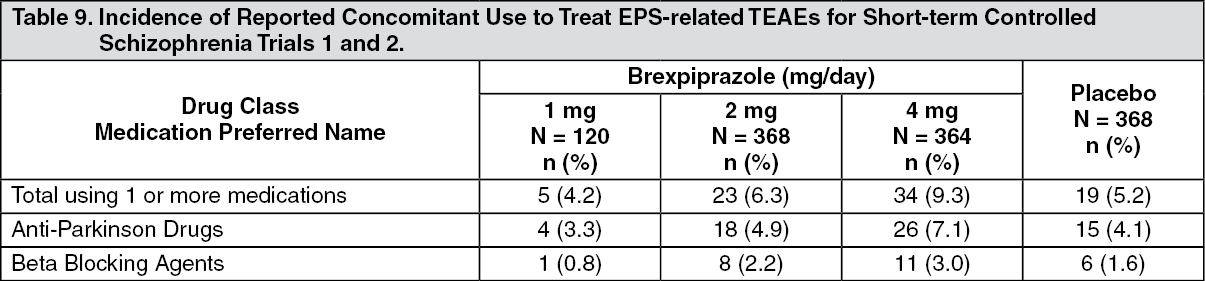
Click on icon to see table/diagram/imageTable 9 presents the reported incidence of concomitant medications used to treat EPS-related TEAEs, including akathisia. (See Table 9.)
 Click on icon to see table/diagram/image
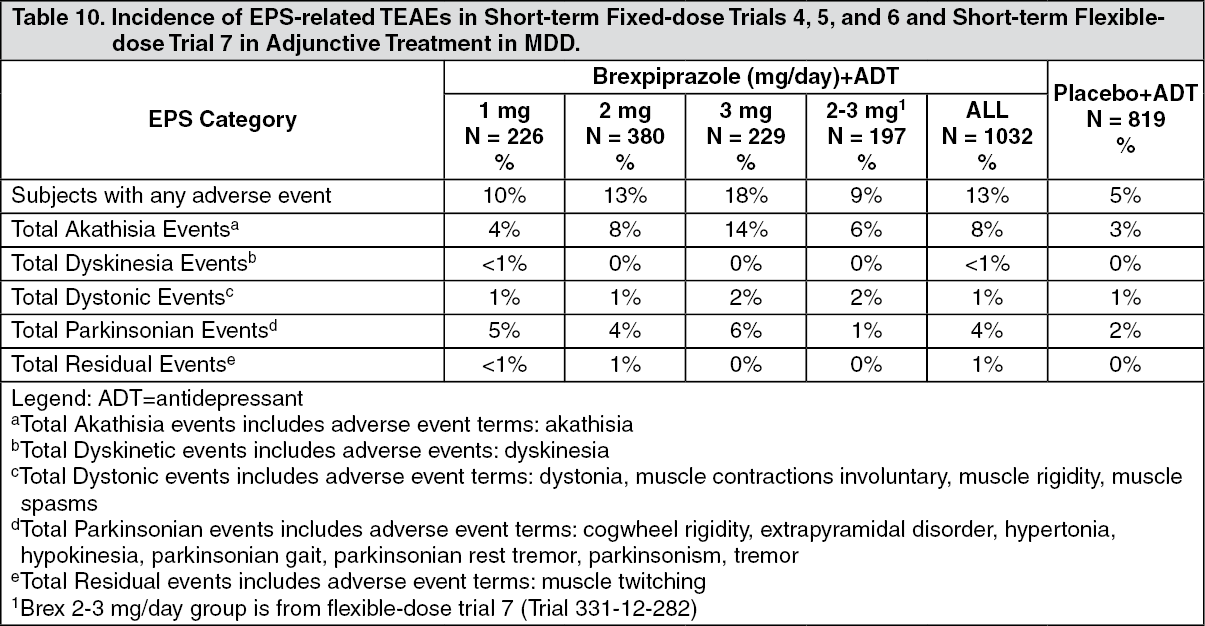
Click on icon to see table/diagram/imageAdjunctive Treatment in Major Depressive Disorder (MDD): In Trials 4, 5 and 6, the incidence of reported EPS-related events, excluding akathisia events, was 5.3% versus 2.4% for placebo-treated subjects. The incidence of akathisia events for REXULTI-treated subjects was dose-dependent. In most cases, akathisia was assessed as mild or moderate in severity. Discontinuations due to akathisia were reported only for REXULTI-treated subjects (0.3% for REXULTI 2 mg/day + ADT, 2.2% for REXULTI 3 mg/day + ADT).
In Trial 7, the incidence of reported EPS-related events, excluding akathisia events, was 2.5% versus 0.5% for placebo-treated subjects. The incidence of akathisia events for REXULTI-treated subjects was 6.1% (2-3 mg) in the REXULTI + ADT group versus 1.9% in the placebo + ADT group. In most cases, akathisia was assessed as mild or moderate in severity.
The incidence of EPS-related TEAEs in the short-term fixed-dose and flexible-dose trials is presented in Table 10. (See Table 10.)
 Click on icon to see table/diagram/image
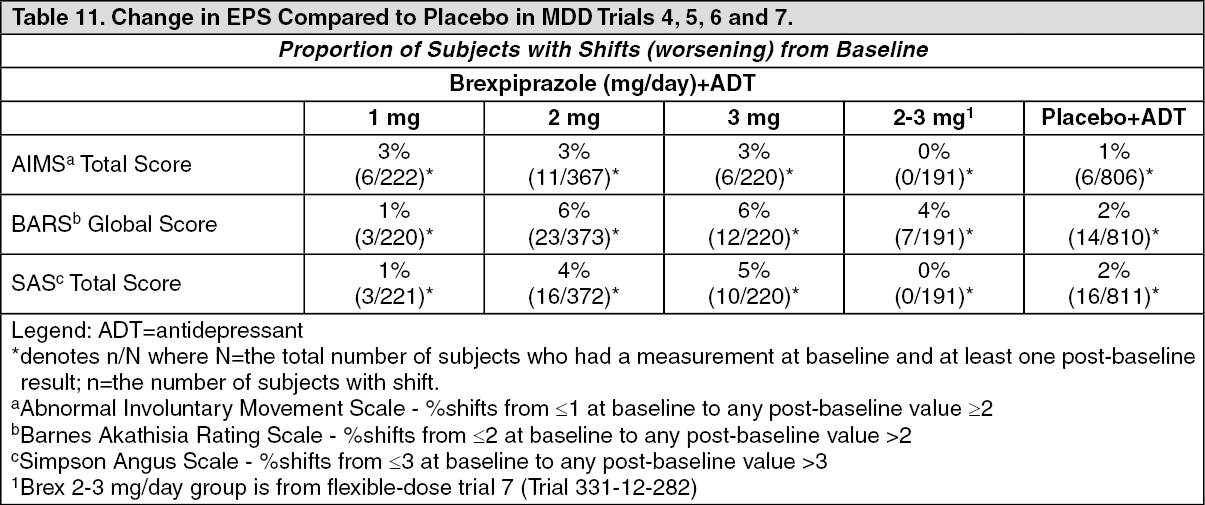
Click on icon to see table/diagram/imageIn Trials 4, 5, 6 and 7, data was objectively collected on the Simpson Angus Rating Score (SAS) for extrapyramidal symptoms (EPS), the Barnes Akathisia Global Score (BARS) for akathisia and the Abnormal Involuntary Movement Score (AIMS) for dyskinesia. The incidence of EPS change is presented in Table 11. (See Table 11.)
 Click on icon to see table/diagram/image
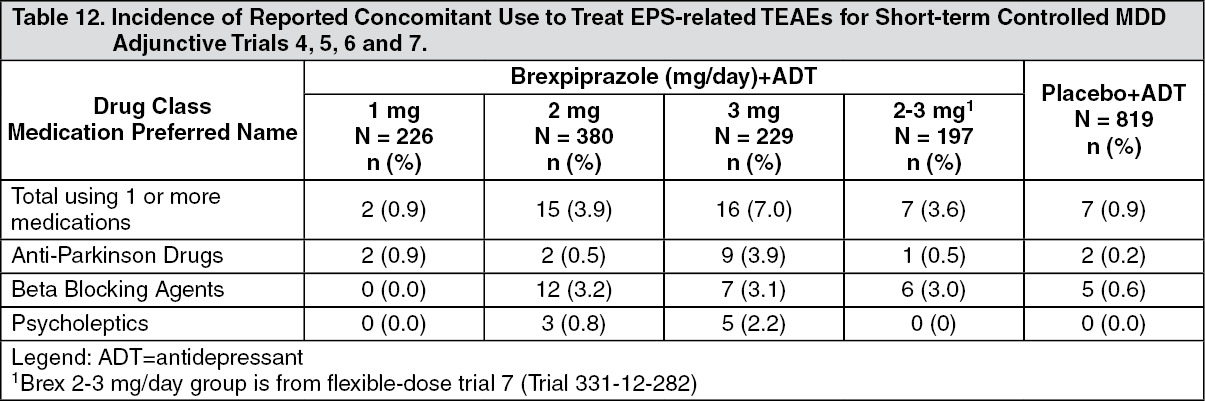
Click on icon to see table/diagram/imageTable 12 presents the reported incidence of concomitant medications used to treat EPS-related TEAEs, including akathisia during Trials 4, 5, 6 and 7. (See Table 12.)
 Click on icon to see table/diagram/image
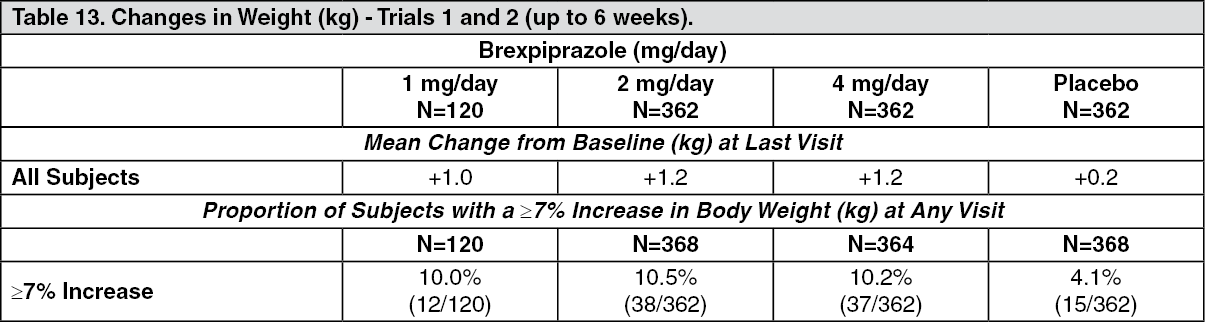
Click on icon to see table/diagram/imageWeight Gain: Schizophrenia: Table 13 shows weight gain data at last visit and percentage of adult subjects with ≥7% increase in body weight at any visit from Trials 1 and 2. (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe percentage of subjects in the 6-week Trials 1 and 2 with an increase of ≥7% in body weight was 10.5% and 10.2% in the REXULTI 2 and 4 mg/day group respectively, compared with 4.1% in the placebo group.
During the longer-term randomized-withdrawal Trial 3 the proportion of subjects with a ≥7% increase in body weight at any visit was 5.2% (5/96) in the REXULTI-treated group compared to 1.0% (1/104) in the placebo group. The proportion of subjects with a ≥7% decrease in body weight at any visit was 9.3% (9/96) in the REXULTI-treated group compared to 15.3% (16/104) in the placebo group. In the stabilization phase of this trial, the proportion of subjects with a ≥7% increase in body weight at any visit was 11.3% (52/462) and with a ≥7% decrease in body weight at any visit was 3.9% (18/462).
In the long-term, open-label schizophrenia studies, the mean change in body weight from baseline to last visit was 1.0 kg (N=1468). The proportion of subjects with a ≥7% increase in body weight at any visit was 17.9% (226/1257) and with a ≥7% decrease in body weight at any visit was 8.2% (104/1257). Weight gain led to discontinuation of study medication in 0.4% (5/1265) of subjects.
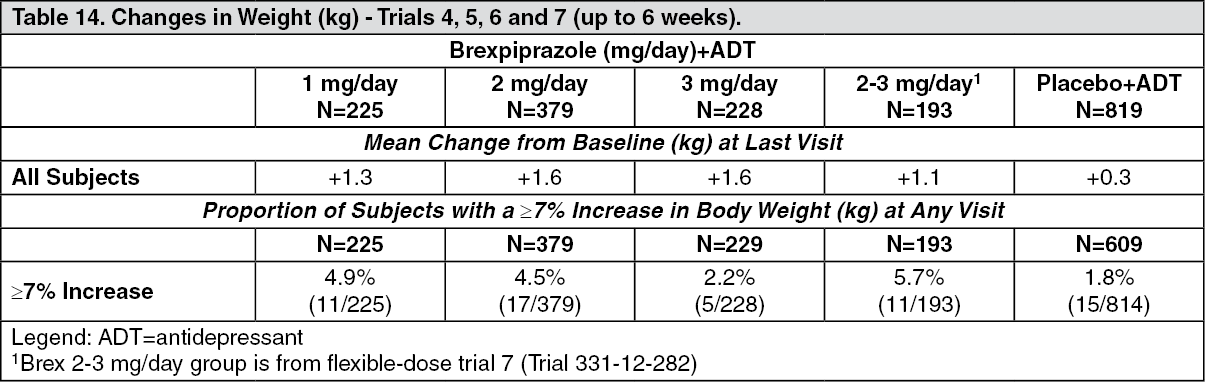
Adjunctive Treatment in Major Depressive Disorder (MDD): Table 14 shows weight gain data at last visit and percentage of adult subjects with ≥7% increase in body weight at any visit from Trials 4, 5, 6 and 7. (See Table 14.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the long-term open-label studies the proportion of subjects with a ≥7% increase in body weight at last visit (LOCF) was 22.1% (494/2232) and with a ≥7% decrease in body weight was 3.2% (72/2232). At 52 weeks (completers), the proportion of subject with a ≥7% increase in body weight at was 28.2 % (286/1013) and with a ≥7% decrease in body weight was 3.7% (37/1013). Weight gain led to discontinuation of study medication in 3.8% (84/2240) of subjects.
Constipation: Patients should be advised of the risk of severe constipation during REXULTI treatment, and they should tell their doctor if constipation occurs or worsens, since they may need medical intervention.
Less Common Clinical Trial Adverse Drug Reactions: Other adverse reactions (<2% frequency in REXULTI-treated patients and greater than placebo) reported in the short-term, placebo-controlled trials in subjects with schizophrenia and MDD (N=2926) and in the long-term placebo-controlled trials in subjects with schizophrenia (N=97), are shown as follows. The following listing does not include adverse reactions: 1) already listed in previous tables or elsewhere in the monograph, 2) for which a drug cause was remote, 3) which were so general as to be uninformative, 4) which were not considered to have clinically significant implications, or 5) which occurred at a rate equal to or less than placebo.
Blood and Lymphatic System Disorders: Infrequent: Anemia.
Cardiovascular Disorders: Infrequent: Vision Blurred, Sinus Bradycardia, Atrioventricular Block First Degree, Palpitations.
Endocrine Disorders: Infrequent: Hyperprolactinemia.
Eye Disorders: Infrequent: Lacrimation increased, Blepharospasm.
Gastrointestinal Disorders: Infrequent: Salivary Hypersecretion, Dental Caries, Abdominal Distension, Gastroesophageal Reflux Disease, Toothache.
General Disorders & Administration Site Conditions: Infrequent: Asthenia, Pyrexia, Chest Pain.
Infections and Infestations: Frequent: Upper Respiratory Tract Infection.
Infrequent: Bronchitis, Conjunctivitis, Urinary Tract Infection.
Investigations: Infrequent: Hepatic Enzyme Increased, Blood Triglycerides Increased, Aspartate Aminotransferase Increased.
Musculoskeletal and Connective Tissue Disorders: Infrequent: Musculoskeletal Pain, Musculoskeletal Stiffness, Rhabdomyolysis.
Nervous System Disorders: Infrequent: Psychomotor Activity, Extrapyramidal Disorder.
Psychiatric Disorders: Infrequent: Abnormal Dreams, Bruxism, Tension.
Respiratory, Thoracic and Mediastinal Disorders: Infrequent: Cough, Dyspnea.
Skin and Subcutaneous Tissue Disorders: Infrequent: Night Sweats.
Vascular Disorders: Infrequent: Hypertension, Orthostatic Hypotension, Hypotension, Flushing.
Abnormal Laboratory Findings: Hematologic and Clinical Chemistry and Other Quantitative Data: Fasting Glucose: Schizophrenia: In the 6-week Trials 1 and 2, the proportion of patients with changes in fasting glucose to post-baseline high (≥126 mg/dL) results were comparable between REXULTI- and placebo-treated subjects.
In the longer-term randomized-withdrawal Trial 3, 7% of patients with normal baseline fasting glucose (N=388) had changes to high fasting glucose during the single-blind REXULTI treatment in the Stabilization phase. During the double-blind phase, from the patients with normal baseline fasting glucose, 4.5% in the REXULTI group (3/66) and 0% in the placebo group (0/62) had changes to high fasting glucose.
In the long-term, open-label schizophrenia studies, 7% of patients with normal baseline fasting glucose experienced a shift from normal to high while taking REXULTI, 17% of subjects with borderline fasting glucose experienced shifts from borderline to high. Combined, 9% of subjects with normal or borderline fasting glucose experienced shifts to high fasting glucose during the long-term schizophrenia studies.
Adjunctive Treatment in Major Depressive Disorder (MDD): In the 6-week Trials 4, 5 and 6, the proportion of patients with changes in fasting glucose from normal values at baseline (ie, < 100 mg/dL) to post-baseline high (≥126 mg/dL) results were comparable between REXULTI+ADT- and placebo+ADT-treated subjects. In Trial 7, the percentage of patients with a shift in fasting glucose from a normal value (ie, < 100 mg/dL) at baseline to a high value (ie, ≥ 126 mg/dL) was 0.8% in the flexible-dose REXULTI + ADT group compared to 0% in the placebo + ADT group. Mean changes from baseline to last visit in the REXULTI + ADT groups were similar to the placebo + ADT group for HbA1c.
In the long-term, open-label MDD studies, 5.2% of patients with normal baseline fasting glucose experienced a shift from normal to high while taking REXULTI + ADT, 24.4% of subjects with borderline fasting glucose experienced shifts from borderline to high. Combined, 9.1% of subjects with normal or borderline fasting glucose experienced shifts to high fasting glucose during the long-term MDD studies.
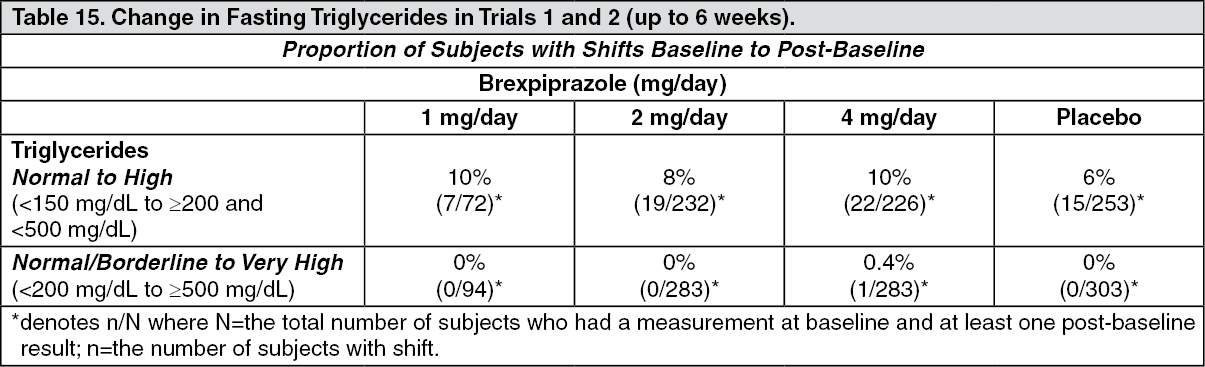
Fasting Lipids: Schizophrenia: In Trials 1 and 2, the proportion of patients with clinically significant changes from baseline in fasting total cholesterol, LDL cholesterol, and HDL cholesterol were similar in REXULTI- and placebo-treated subjects. Table 15 shows the proportions of subjects with changes in fasting triglycerides. (See Table 15.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the longer-term randomized-withdrawal Trial 3, 22% of patients with normal baseline fasting triglycerides (N=394) had changes to high or very high fasting triglycerides during single-blind REXULTI treatment in the Stabilization phase. During the double-blind phase, from the patients with normal baseline fasting triglycerides, 7% in the REXULTI group (4/57) and 0% in the placebo group (0/60) had changes to high fasting triglycerides.
In the long-term open-label studies, shifts in baseline fasting cholesterol from normal to high were reported in 6% (total cholesterol), 3% (LDL cholesterol), and shifts in baseline from normal to low were reported in 20% (HDL cholesterol) of patients taking REXULTI. Of patients with normal baseline triglycerides, 14% experienced shifts to high, and 0.3% experienced shifts to very high triglycerides. Combined, 0.5% of subjects with normal or borderline fasting triglycerides experienced shifts to very high fasting triglycerides during the long-term schizophrenia studies.
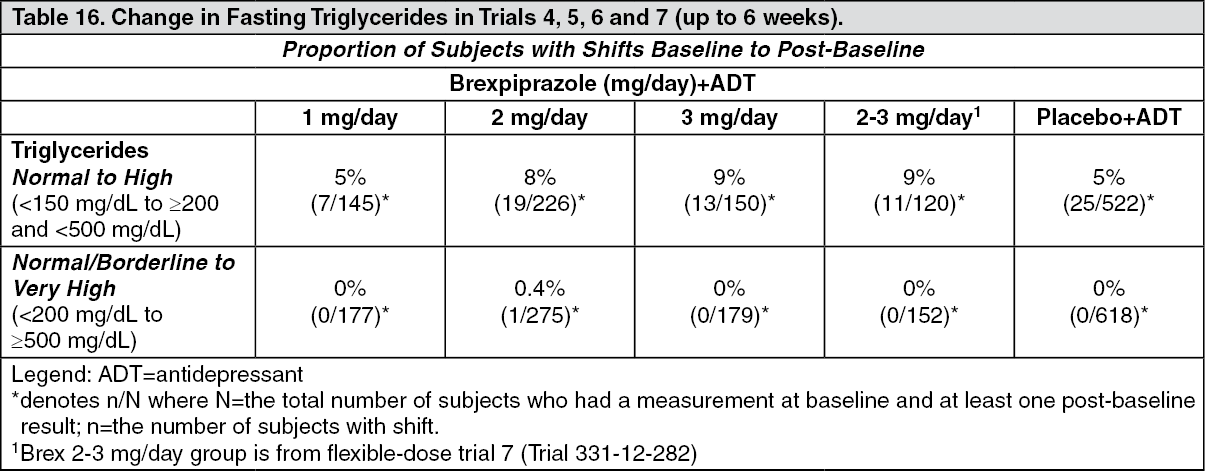
Adjunctive Treatment in Major Depressive Disorder (MDD): In Trials 4, 5, 6, and 7, the proportion of patients with clinically significant changes from baseline in fasting total cholesterol, LDL cholesterol, and HDL cholesterol were similar in REXULTI+ADT- and placebo+ADT-treated subjects. Table 16 shows the proportions of subjects with changes in fasting triglycerides in Trials 4, 5, 6 and 7. (See Table 16.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the long-term open-label studies, shifts in baseline fasting cholesterol from normal to high were reported in 8.7% (total cholesterol), 3.2% (LDL cholesterol), and shifts in baseline from normal to low were reported in 13.3% (HDL cholesterol) of patients taking REXULTI + ADT. Of patients with normal baseline triglycerides, 17.3% experienced shifts to high, and 0.2% experienced shifts to very high triglycerides. Combined, 0.6% of subjects with normal or borderline fasting triglycerides experienced shifts to very high fasting triglycerides during the long-term MDD studies.
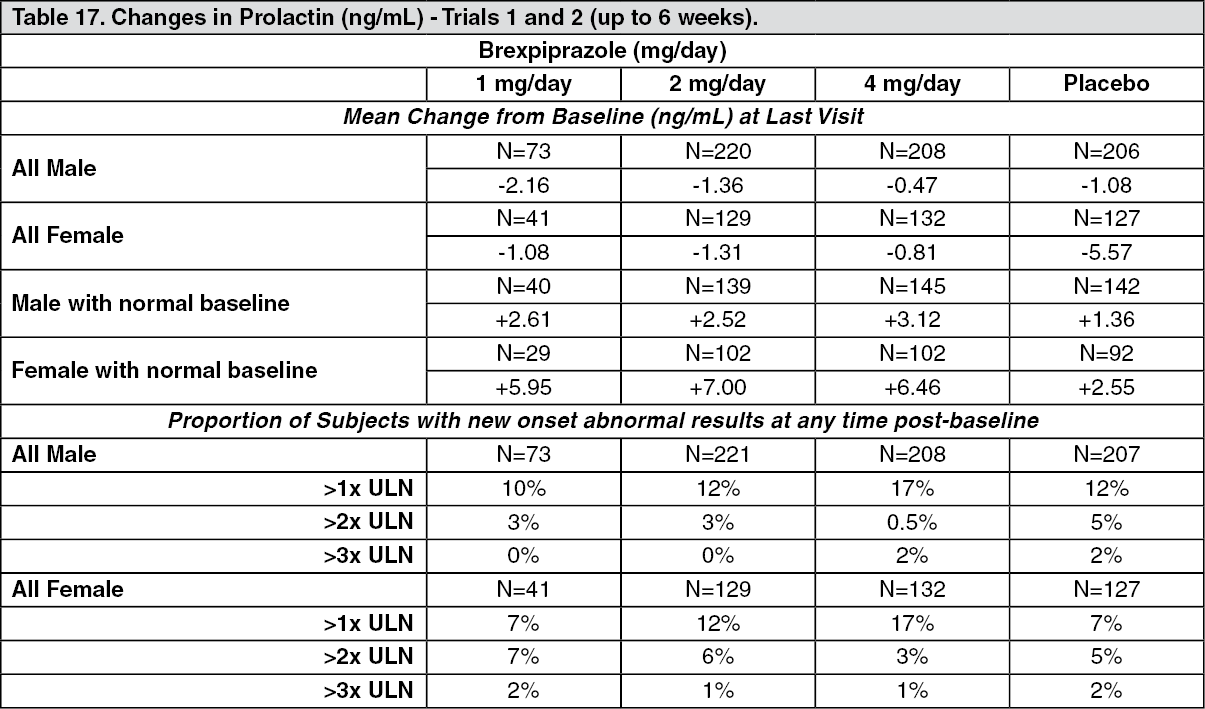
Prolactin: Schizophrenia: Table 17 shows the mean change from baseline in prolactin and the proportion of subjects with prolactin elevations. (See Table 17.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the longer-term randomized-withdrawal Trial 3, the mean change from baseline at last visit in prolactin in females was -2.17 ng/mL in REXULTI-treated group compared with -4.25 ng/mL in the placebo group. In males, mean change from baseline at last visit in prolactin was -1.73 ng/mL in REXULTI-treated group compared with 1.38 ng/mL in the placebo group. For females with normal prolactin results at baseline, the mean changes to last visit were 4.04 ng/mL in the REXULTI-treated group and -5.95 ng/mL in the placebo group; for males with normal baseline, the mean changes to last visit were 0.05 ng/mL in the REXULTI-treated group and 2.61 ng/mL in the placebo group. The proportion of subjects with prolactin elevations >1X ULN in females was 5.2% in the REXULTI-treated group compared with 2.6% in the placebo group. In males, the proportion of subjects with prolactin elevations >1X ULN was 3.6% in the REXULTI-treated group compared with 4.9% in the placebo group. Similarly, prolactin elevations >3X ULN in females was 0.0% in the REXULTI-treated group compared with 5.2% in the placebo group. In males, prolactin elevations >3X ULN was 0.0% in the REXULTI-treated group compared with 3.2% in the placebo group.
In the long-term open-label schizophrenia trials, the mean change from baseline at last visit in prolactin in females was 2.78 ng/mL in REXULTI-treated group and 0.60 ng/mL in males. The proportion of subjects with prolactin elevations >1X ULN was 17.5% in females and 14.0% in males in the REXULTI-treated group, and prolactin elevations >3X ULN was 4.1% in females and 1.7% in males.
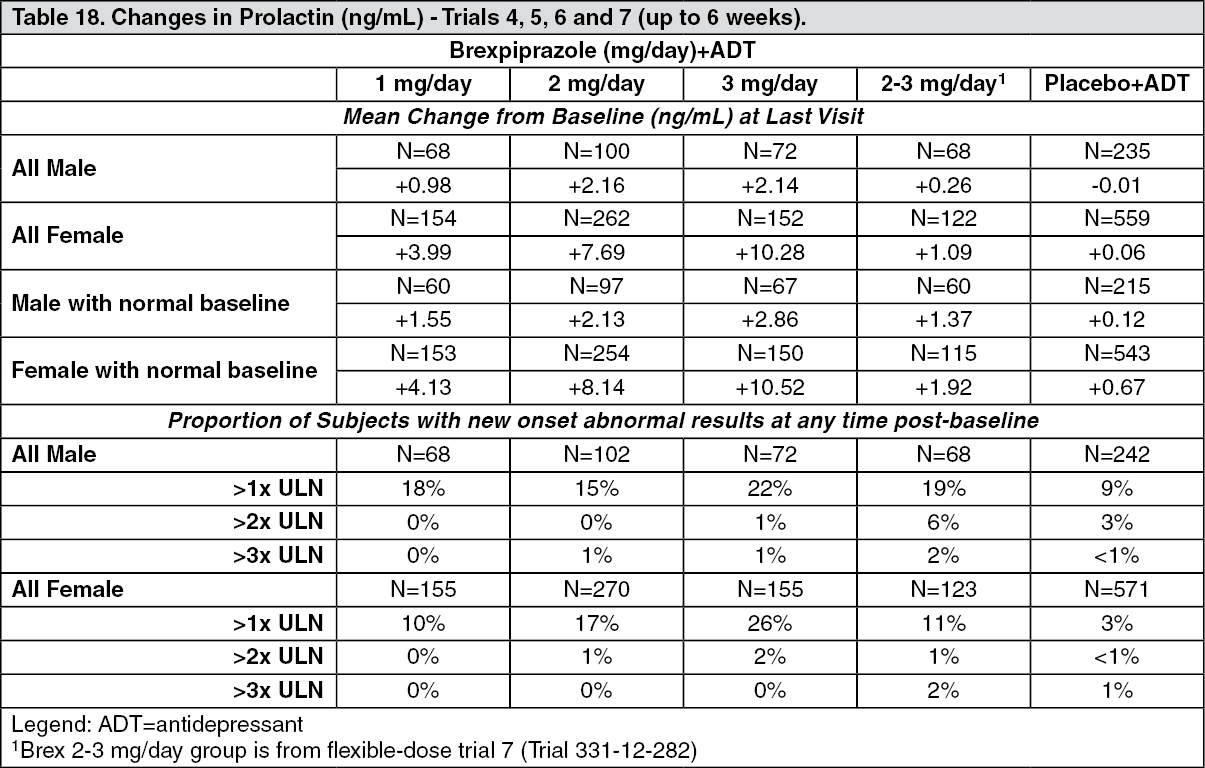
Adjunctive Treatment in Major Depressive Disorder (MDD): Table 18 shows the mean change from baseline in prolactin and the proportion of subjects with prolactin elevations in Trials 4, 5, 6 and 7. (See Table 18.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the long-term open-label MDD trials, the mean change from baseline at last visit in prolactin in females was 1.86 ng/mL in REXULTI + ADT group and 0.50 ng/mL in males. The proportion of subjects with prolactin elevations >1X ULN was 15.4% in females and 13.5% in males in the REXULTI + ADT group, and prolactin elevations >3X ULN was 0.5% in females and 0.9% in males.
Post-Market Adverse Drug Reactions: Immune system disorders: hypersensitivity reactions (including anaphylaxis, angioedema, facial swelling, rash and urticaria).
Neurological: seizure, neuroleptic malignant syndrome.
Psychiatric disorders: suicidality (including completed suicide, attempted suicide, suicidal behavior and suicidal ideation).
Atypical antipsychotic drugs, such as REXULTI, have been associated with cases of sleep apnea, with or without concomitant weight gain. In patients who have a history of or are at risk for sleep apnea, REXULTI should be prescribed with caution.
Complex sleep-related behaviors such as somnambulism and sleep-related eating disorder have been associated with the use of atypical antipsychotic drugs.
View ADR Monitoring Form