


 Sign Out
Sign Out
In the placebo-controlled atopic dermatitis clinical trials, the most commonly reported adverse reactions (≥2% of patients) with upadacitinib 15 mg or 30 mg were upper respiratory tract infection (25.4%), acne (15.1%), herpes simplex (8.4%), headache (6.3%), blood CPK increased (5.5%), cough (3.2%), folliculitis (3.2%), abdominal pain (2.9%), nausea (2.7%), neutropaenia (2.3%), pyrexia (2.1%), and influenza (2.1%).
In the placebo-controlled ulcerative colitis and Crohn's disease induction and maintenance clinical trials, the most commonly reported adverse reactions (≥3% of patients) with upadacitinib 45 mg, 30 mg or 15 mg were upper respiratory tract infection (19.9%), pyrexia (8.7%), blood CPK increased (7.6%), anemia (7.4%), headache (6.6%), acne (6.3%), herpes zoster (6.1%), neutropaenia (6.0%), rash (5.2%), pneumonia (4.1%), hypercholesterolemia (4.0%), bronchitis (3.9%), aspartate transaminase increased (3.9%), fatigue (3.9%), folliculitis (3.6%), alanine transaminase increased (3.5%), herpes simplex (3.2%), and influenza (3.2%).
The most common serious adverse reactions were serious infections (see Precautions).
The safety profile of upadacitinib with long-term treatment was generally similar to the safety profile during the placebo-controlled period across indications.
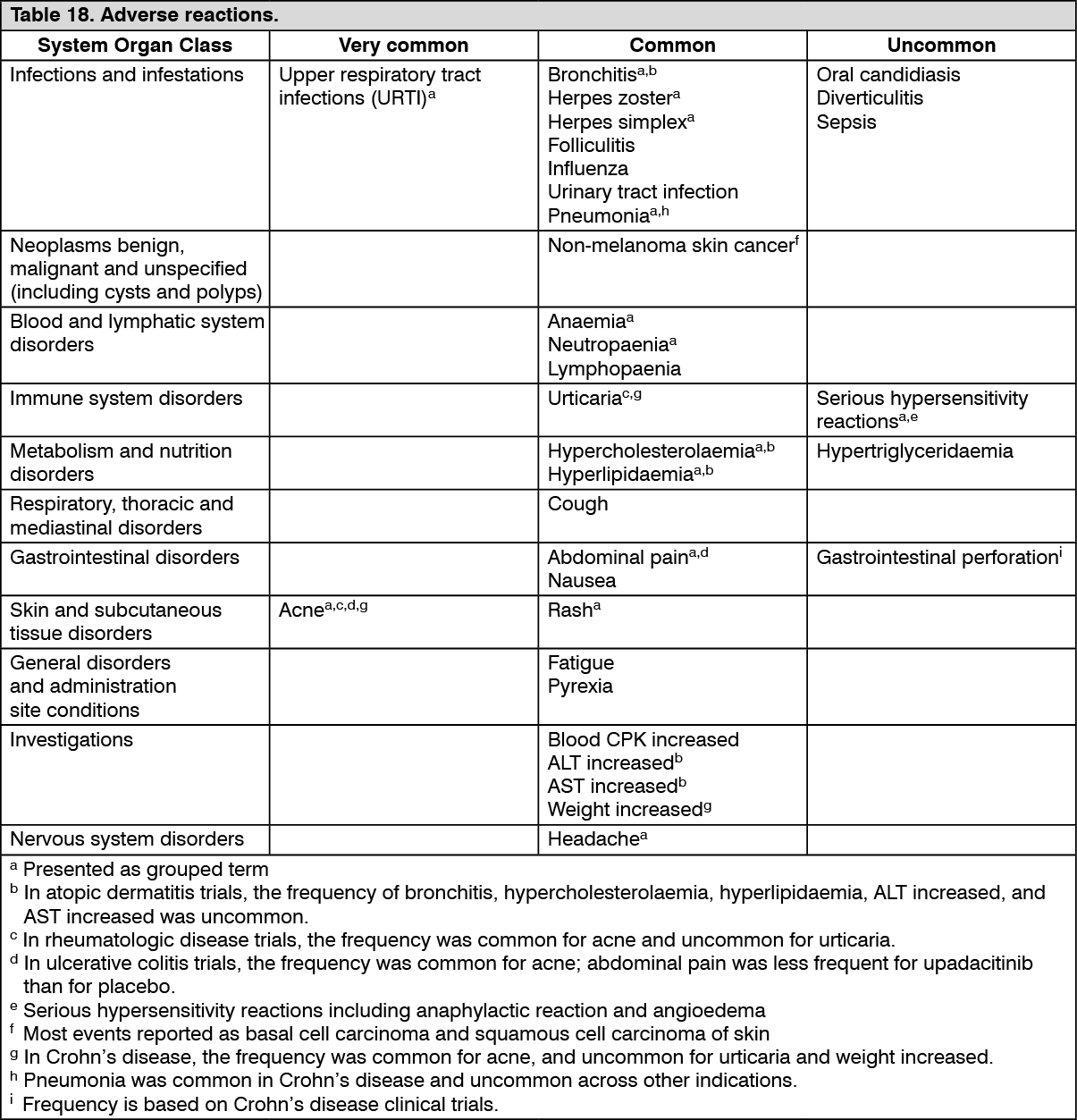
Tabulated list of adverse reactions: The following list of adverse reactions is based on experience from clinical studies.
The frequency of adverse reactions listed as follows is defined using the following convention: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1 000 to <1/100). The frequencies in Table 18 are based on the higher of the rates for adverse reactions reported with RINVOQ in clinical trials of rheumatologic disease (15 mg), atopic dermatitis (15 mg and 30 mg), ulcerative colitis (15 mg, 30 mg and 45 mg), or Crohn's disease (15 mg, 30 mg, and 45 mg). When notable differences in frequency were observed between indications, these are presented in the footnotes following the table. (See Table 18.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Rheumatoid arthritis: Infections: In placebo-controlled clinical studies with background DMARDs, the frequency of infection over 12/14 weeks in the upadacitinib 15 mg group was 27.4% compared to 20.9% in the placebo group. In methotrexate (MTX)-controlled studies, the frequency of infection over 12/14 weeks in the upadacitinib 15 mg monotherapy group was 19.5% compared to 24.0% in the MTX group. The overall long-term rate of infections for the upadacitinib 15 mg group across all five Phase 3 clinical studies (2 630 patients) was 93.7 events per 100 patient-years.
In placebo-controlled clinical studies with background DMARDs, the frequency of serious infection over 12/14 weeks in the upadacitinib 15 mg group was 1.2% compared to 0.6% in the placebo group. In MTX-controlled studies, the frequency of serious infection over 12/14 weeks in the upadacitinib 15 mg monotherapy group was 0.6% compared to 0.4% in the MTX group. The overall long-term rate of serious infections for the upadacitinib 15 mg group across all five Phase 3 clinical studies was 3.8 events per 100 patient-years. The most common serious infection was pneumonia. The rate of serious infections remained stable with long-term exposure.
Opportunistic infections (excluding tuberculosis): In placebo-controlled clinical studies with background DMARDs, the frequency of opportunistic infections over 12/14 weeks in the upadacitinib 15 mg group was 0.5% compared to 0.3% in the placebo group. In MTX-controlled studies, there were no cases of opportunistic infection over 12/14 weeks in the upadacitinib 15 mg monotherapy group and 0.2% in the MTX group. The overall long-term rate of opportunistic infections for the upadacitinib 15 mg group across all five Phase 3 clinical studies was 0.6 events per 100 patient-years.
The long-term rate of herpes zoster for the upadacitinib 15 mg group across all five Phase 3 clinical studies was 3.7 events per 100 patient-years. Most of the herpes zoster events involved a single dermatome and were non-serious.
Hepatic transaminase elevations: In placebo-controlled studies with background DMARDs, for up to 12/14 weeks, alanine transaminase (ALT) and aspartate transaminase (AST) elevations ≥3 x upper limit of normal (ULN) in at least one measurement were observed in 2.1% and 1.5% of patients treated with upadacitinib 15 mg, compared to 1.5% and 0.7%, respectively, of patients treated with placebo. Most cases of hepatic transaminase elevations were asymptomatic and transient.
In MTX-controlled studies, for up to 12/14 weeks, ALT and AST elevations ≥3 x ULN in at least one measurement were observed in 0.8% and 0.4% of patients treated with upadacitinib 15 mg, compared to 1.9% and 0.9%, respectively, of patients treated with MTX.
The pattern and incidence of elevation in ALT/AST remained stable over time including in long-term extension studies.
Lipid elevations: Upadacitinib 15 mg treatment was associated with increases in lipid parameters including total cholesterol, triglycerides, LDL cholesterol and HDL cholesterol. There was no change in the LDL/HDL ratio. Elevations were observed at 2 to 4 weeks of treatment and remained stable with longer-term treatment. Among patients in the controlled studies with baseline values below the specified limits, the following frequencies of patients were observed to shift to above the specified limits on at least one occasion during 12/14 weeks (including patients who had an isolated elevated value): Total cholesterol ≥5.17 mmol/L (200 mg/dL): 62% vs. 31%, in the upadacitinib 15 mg and placebo groups, respectively.
LDL cholesterol ≥3.36 mmol/L (130 mg/dL): 42% vs. 19%, in the upadacitinib 15 mg and placebo groups, respectively.
HDL cholesterol ≥1.03 mmol/L (40 mg/dL): 89% vs. 61%, in the upadacitinib 15 mg and placebo groups, respectively.
Triglycerides ≥2.26 mmol/L (200 mg/dL): 25% vs. 15%, in the upadacitinib 15 mg and placebo groups, respectively.
Creatine phosphokinase: In placebo-controlled studies with background DMARDs, for up to 12/14 weeks, increases in CPK values were observed. CPK elevations >5 x upper limit of normal (ULN) were reported in 1.0% and 0.3% of patients over 12/14 weeks in the upadacitinib 15 mg and placebo groups, respectively. Most elevations >5 x ULN were transient and did not require treatment discontinuation. Mean CPK values increased by 4 weeks with a mean increase of 60 U/L at 12 weeks and then remained stable at an increased value thereafter including with extended therapy.
Neutropaenia: In placebo-controlled studies with background DMARDs, for up to 12/14 weeks, decreases in neutrophil counts below 1 x 109 cells/L in at least one measurement occurred in 1.1% and <0.1% of patients in the upadacitinib 15 mg and placebo groups, respectively. In clinical studies, treatment was interrupted in response to ANC <1 x 109 cells/L (see Dosage & Administration). Mean neutrophil counts decreased over 4 to 8 weeks. The decreases in neutrophil counts remained stable at a lower value than baseline over time including with extended therapy.
Psoriatic arthritis: Overall, the safety profile observed in patients with active psoriatic arthritis treated with upadacitinib 15 mg was consistent with the safety profile observed in patients with rheumatoid arthritis. A higher rate of serious infections (2.6 events per 100 patient-years and 1.3 events per 100 patient-years, respectively) and hepatic transaminase elevations (ALT elevations Grade 3 and higher rates 1.4% and 0.4%, respectively) was observed in patients treated with upadacitinib in combination with MTX therapy compared to patients treated with monotherapy.
Axial spondyloarthritis: Overall, the safety profile observed in patients with active axial spondyloarthritis treated with upadacitinib 15 mg was consistent with the safety profile observed in patients with rheumatoid arthritis. No new safety findings were identified.
Atopic dermatitis: Infections: In the placebo-controlled period of the clinical studies, the frequency of infection over 16 weeks in the upadacitinib 15 mg and 30 mg groups was 39% and 43% compared to 30% in the placebo group, respectively. The long-term rate of infections for the upadacitinib 15 mg and 30 mg groups was 98.5 and 109.6 events per 100 patient-years, respectively.
In placebo-controlled clinical studies, the frequency of serious infection over 16 weeks in the upadacitinib 15 mg and 30 mg groups was 0.8% and 0.4% compared to 0.6% in the placebo group, respectively. The long-term rate of serious infections for the upadacitinib 15 mg and 30 mg groups was 2.3 and 2.8 events per 100 patient-years, respectively.
Opportunistic infections (excluding tuberculosis): In the placebo-controlled period of the clinical studies, all opportunistic infections (excluding TB and herpes zoster) reported were eczema herpeticum. The frequency of eczema herpeticum over 16 weeks in the upadacitinib 15 mg and 30 mg groups was 0.7% and 0.8% compared to 0.4% in the placebo group, respectively. The long-term rate of eczema herpeticum for the upadacitinib 15 mg and 30 mg groups was 1.6 and 1.8 events per 100 patient-years, respectively. One case of esophageal candidiasis was reported with upadacitinib 30 mg.
The long-term rate of herpes zoster for the upadacitinib 15 mg and 30 mg groups was 3.5 and 5.2 events per 100 patient-years, respectively. Most of the herpes zoster events involved a single dermatome and were non-serious.
Laboratory abnormalities: Dose-dependent changes in ALT increased and/or AST increased (≥3 x ULN), lipid parameters, CPK values (>5 x ULN), and neutropaenia (ANC <1 x 109 cells/L) associated with upadacitinib treatment were similar to what was observed in the rheumatologic disease clinical studies.
Small increases in LDL cholesterol were observed after week 16 in atopic dermatitis studies.
Ulcerative colitis: The overall safety profile observed in patients with ulcerative colitis was generally consistent with that observed in patients with rheumatoid arthritis.
A higher rate of herpes zoster was observed with an induction treatment period of 16 weeks vs 8 weeks.
Infections: In the placebo-controlled induction studies, the frequency of infection over 8 weeks in the upadacitinib 45 mg group compared to the placebo group was 20.7% and 17.5%, respectively. In the placebo-controlled maintenance study, the frequency of infection over 52 weeks in the upadacitinib 15 mg and 30 mg groups was 38.4% and 40.6%, respectively, compared to 37.6% in the placebo group. The long-term rate of infections for upadacitinib 15 mg and 30 mg was 73.8 and 82.6 events per 100 patient-years, respectively.
In the placebo-controlled induction studies, the frequency of serious infection over 8 weeks in both the upadacitinib 45 mg group and the placebo group was 1.3%. No additional serious infections were observed over 8-week extended treatment with upadacitinib 45 mg. In the placebo-controlled maintenance study, the frequency of serious infection over 52 weeks in the upadacitinib 15 mg and 30 mg groups was 3.2% and 2.4%, respectively, compared to 3.3% in the placebo group. The long term rate of serious infections for the upadacitinib 15 mg and 30 mg groups was 4.1 and 3.9 events per 100 patient-years, respectively. The most frequently reported serious infection in the induction and maintenance phases was COVID-19 pneumonia.
Opportunistic infections (excluding tuberculosis): In the placebo-controlled induction studies over 8 weeks, the frequency of opportunistic infection (excluding tuberculosis and herpes zoster) in the upadacitinib 45 mg group was 0.4% and 0.3% in the placebo group. No additional opportunistic infections (excluding tuberculosis and herpes zoster) were observed over 8-week extended treatment with upadacitinib 45 mg. In the placebo-controlled maintenance study over 52 weeks, the frequency of opportunistic infection (excluding tuberculosis and herpes zoster) in the upadacitinib 15 mg and 30 mg groups was 0.8% and 0.4%, respectively, compared to 0.8% in the placebo group. The long-term rate of opportunistic infections (excluding tuberculosis and herpes zoster) for the upadacitinib 15 mg and 30 mg groups was 0.6 and 0.3 events per 100 patient-years, respectively.
In the placebo-controlled induction studies over 8 weeks, the frequency of herpes zoster in the upadacitinib 45 mg group was 0.6% and 0% in the placebo group. The frequency of herpes zoster was 3.9% over 16-week treatment with upadacitinib 45 mg. In the placebo-controlled maintenance study over 52 weeks, the frequency of herpes zoster in the upadacitinib 15 mg and 30 mg groups was 4.4% and 4.0%, respectively, compared to 0% in the placebo group. The long-term rate of herpes zoster for the upadacitinib 15 mg and 30 mg groups was 5.7 and 6.3 events per 100 patient-years, respectively.
Laboratory abnormalities: In the induction and maintenance clinical studies, the laboratory changes in ALT increased and/or AST increased (≥3 x ULN), CPK values (>5 x ULN), and neutropaenia (ANC <1 x 109 cells/L) associated with upadacitinib treatment were generally similar to what was observed in the rheumatologic disease and atopic dermatitis clinical studies. Dose-dependent changes for these laboratory parameters associated with 15 mg and 30 mg upadacitinib treatment were observed.
In the placebo-controlled induction studies for up to 8 weeks, decreases in lymphocyte counts below 0.5 x 109 cells/L in at least one measurement occurred in 2.0% and 0.8% of patients in the upadacitinib 45 mg and placebo groups, respectively. In the placebo-controlled maintenance study, for up to 52 weeks, decreases in lymphocyte counts below 0.5 x 109 cells/L in at least one measurement occurred in 1.6%, 0.8% and 0.8% of patients in the upadacitinib 15 mg, 30 mg and placebo groups, respectively. In clinical studies, treatment was interrupted in response to ALC <0.5 x 109 cells/L (see Dosage & Administration). No notable mean changes of lymphocyte counts were observed during upadacitinib treatment over time.
Elevations in lipid parameters were observed at 8 weeks of treatment with upadacitinib 45 mg and remained generally stable with longer-term treatment with upadacitinib 15 mg and 30 mg. Among patients in the placebo-controlled induction studies with baseline values below the specified limits, the following frequencies of patients were observed to shift to above the specified limits on at least one occasion during 8 weeks (including patients who had an isolated elevated value): Total cholesterol ≥5.17 mmol/L (200 mg/dL): 49% vs. 11%, in the upadacitinib 45 mg and placebo groups, respectively.
LDL cholesterol ≥3.36 mmol/L (130 mg/dL): 27% vs. 9%, in the upadacitinib 45 mg and placebo groups, respectively.
HDL cholesterol ≥1.03 mmol/L (40 mg/dL): 79% vs. 36%, in the upadacitinib 45 mg and placebo groups, respectively.
Triglycerides ≥2.26 mmol/L (200 mg/dL): 6% vs 4% in the upadacitinib 45 mg and placebo groups, respectively.
Crohn's disease: Overall, the safety profile observed in patients with Crohn's disease treated with upadacitinib was consistent with the known safety profile for upadacitinib.
Serious infections: In the placebo-controlled induction studies, the frequency of serious infection over 12 weeks in the upadacitinib 45 mg group and the placebo group was 1.9% and 1.7%, respectively. In the placebo-controlled maintenance study, the frequency of serious infection over 52 weeks in the upadacitinib 15 mg and 30 mg groups was 3.2% and 5.7%, respectively, compared to 4.5% in the placebo group. The long-term rate of serious infections for the upadacitinib 15 mg and 30 mg groups in patients who responded to upadacitinib 45 mg as induction treatment was 5.1 and 7.3 events per 100 patient-years, respectively. The most frequently reported serious infection in the induction and maintenance studies was gastrointestinal infections.
Gastrointestinal Perforations: During the placebo-controlled period in the Phase 3 induction clinical studies, gastrointestinal perforation was reported in 1 patient (0.1%) treated with upadacitinib 45 mg and no patients on placebo through 12 weeks. In all patients treated with upadacitinib 45 mg (n=938) during the induction studies, gastrointestinal perforation was reported in 4 patients (0.4%).
In the long-term placebo-controlled period, gastrointestinal perforation was reported in 1 patient each treated with placebo (0.7 per 100 patient-years), upadacitinib 15 mg (0.4 per 100 patient-years), and upadacitinib 30 mg (0.4 per 100 patient-years). In all patients treated with rescue upadacitinib 30 mg (n=336), gastrointestinal perforation was reported in 3 patients (0.8 per 100 patient-years) through long-term treatment.
Laboratory abnormalities: In the induction and maintenance clinical studies, the laboratory changes in ALT increased and/or AST increased (≥3 x ULN), CPK values (>5 x ULN), neutropaenia (ANC <1 x 109 cells/L), and lipid parameters associated with upadacitinib treatment were generally similar to what was observed in the rheumatologic disease, atopic dermatitis and ulcerative colitis clinical studies. Dose-dependent changes for these laboratory parameters associated with 15 mg and 30 mg upadacitinib treatment were observed.
In the placebo-controlled induction studies for up to 12 weeks, decreases in lymphocyte counts below 0.5 x 109 cells/L in at least one measurement occurred in 2.2% and 2.0% of patients in the upadacitinib 45 mg and placebo groups, respectively. In the placebo-controlled maintenance study, for up to 52 weeks, decreases in lymphocyte counts below 0.5 x 109 cells/L in at least one measurement occurred in 4.6%, 5.2% and 1.8% of patients in the upadacitinib 15 mg, 30 mg and placebo groups, respectively. In clinical studies, treatment was interrupted in response to ALC <0.5 x 109 cells/L (see Dosage & Administration). No notable mean changes of lymphocyte counts were observed during upadacitinib treatment over time.
In the placebo-controlled induction studies for up to 12 weeks, decreases in haemoglobin concentration to below 8 g/dL in at least one measurement occurred in 2.7% and 1.4% of patients in the upadacitinib 45 mg and placebo groups, respectively. In the placebo-controlled maintenance study, for up to 52 weeks, decreases in haemoglobin concentration below 8 g/dL in at least one measurement occurred in 1.4%, 4.4% and 2.8% of patients in the upadacitinib 15 mg, 30 mg and placebo groups, respectively. In clinical studies, treatment was interrupted in response to Hb <8 g/dL (see Dosage & Administration). No notable mean changes of haemoglobin concentration were observed during upadacitinib treatment over time.
Elderly: Based on limited data in atopic dermatitis patients 65 years of age and older, there was a higher rate of overall adverse reactions with the upadacitinib 30 mg dose compared to the 15 mg dose.
Based on the limited data in ulcerative colitis and Crohn's disease patients 65 years of age and older, there was a higher rate of overall adverse reactions with the upadacitinib 30 mg dose compared to the 15 mg dose with maintenance treatment (see Precautions).
Paediatric population: A total of 343 adolescents aged 12 to 17 years with atopic dermatitis were treated in the Phase 3 studies, of whom 167 were exposed to 15 mg. The safety profile for upadacitinib 15 mg in adolescents was similar to that in adults. The safety and efficacy of the 30 mg dose in adolescents are still being investigated.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions according to the local requirements.
View ADR Monitoring Form