


 Sign Out
Sign Out




Pharmacology: Pharmacodynamics: Mechanism of action: By combining the VZV specific antigen (gE) with an adjuvant system (AS01B), Shingrix is designed to induce antigen-specific cellular and humoral immune responses in individuals with pre-existing immunity against VZV.
Non-clinical data show that AS01B induces a local and transient activation of the innate immune system through specific molecular pathways. This facilitates the recruitment and activation of antigen presenting cells carrying gE-derived antigens in the draining lymph node, which in turn leads to the generation of gE-specific CD4+ T cells and antibodies. The adjuvant effect of AS01B is the result of interactions between MPL and QS-21 formulated in liposomes.
Efficacy of Shingrix: Efficacy against Herpes Zoster (HZ) and Post-Herpetic Neuralgia (PHN): Two phase III, placebo-controlled, observer-blind efficacy studies of Shingrix were conducted in adults ≥50 years with 2 doses administered 2 months apart.
ZOE-50 (Zoster-006): Total Vaccinated Cohort (TVC) of 15,405 adults ≥50 years who received at least one dose of either Shingrix (N=7,695) or placebo (N=7,710).
ZOE-70 (Zoster-022): TVC of 13,900 adults ≥70 years who received at least one dose of either Shingrix (N=6,950) or placebo (N=6,950).
The studies were not designed to demonstrate efficacy in subgroups of frail individuals, including those with multiple comorbidities, although these subjects were not excluded from the studies.
Two phase III, placebo-controlled, observer-blind studies evaluating Shingrix efficacy were conducted in IC adults ≥18 years with 2 doses administered 1-2 months apart.
Zoster-002: TVC of 1,846 autologous hematopoietic stem cell transplants (aHSCT) recipients who received at least one dose of either Shingrix (N=922) or placebo (N=924) 50-70 days post-transplant, 21.3% (Shingrix) and 20.5% (placebo) of the subjects received at least one immunosuppressive (IS) treatment (for a duration of at least one day) from HSCT up to 30 days after Dose 2 (TVC). The proportion of subjects by underlying disease was: 53.1% (Shingrix) and 53.4% (placebo) for multiple myeloma (MM) and 46.9% (Shingrix) and 46.6% (placebo) for other diagnosis.
Zoster-039: TVC of 562 subjects with hematologic malignancies who received at least one dose of either Shingrix (N=283) or placebo (N=279) during a cancer therapy course (37%) or after the full cancer therapy course (63%). The proportion of subjects by underlying disease was: 70.7% (Shingrix) and 71.3% (placebo) for MM and other diseases, 14.5% (Shingrix) and 14.0% (placebo) for non-Hodgkin B-cell lymphoma (NHBCL) and 14.8% (Shingrix) and 14.7% (placebo) for chronic lymphocytic leukaemia (CLL).
These studies were not designed to assess the impact of concomitant use of IS therapy on vaccine efficacy or to assess the impact of specific IS treatments on vaccine efficacy. Most vaccine recipients were not under IS therapy at the time of vaccination (see as previously mentioned). Not all types of IS therapies were used in the populations studied.
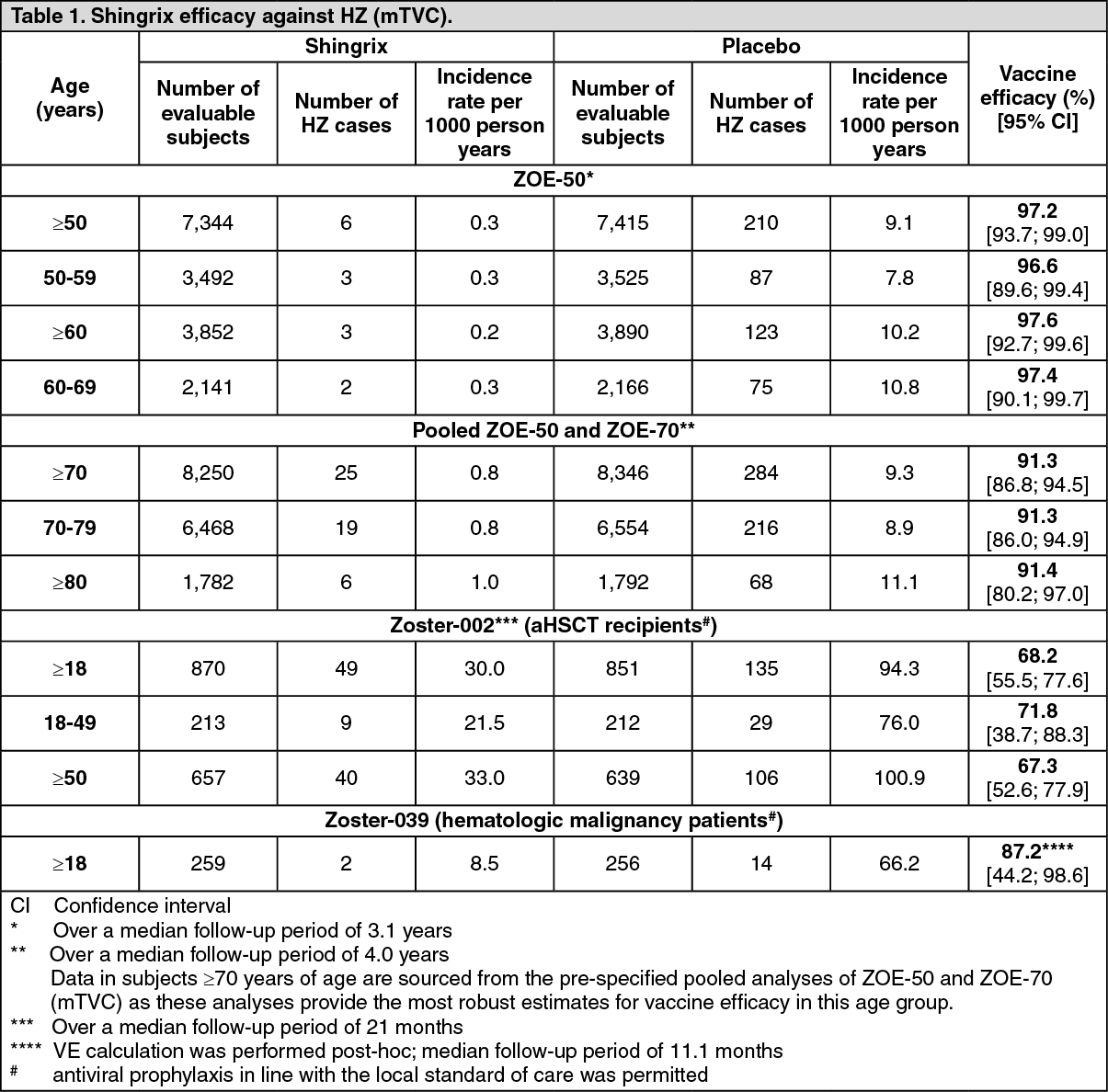
Incidence of HZ and PHN cases as well as vaccine efficacy were evaluated in the modified Total Vaccinated Cohort (mTVC), i.e. excluding adults who did not receive the second dose of vaccine or who had a confirmed diagnosis of HZ within one month after the second dose.
Shingrix significantly decreased the incidence of HZ compared with placebo in: Adults ≥50 years (ZOE-50): 6 vs. 210 cases.
Adults ≥70 years (pooled analysis of ZOE-50 and ZOE-70): 25 vs. 284 cases.
Adults ≥18 years with aHSCT (Zoster-002): 49 vs. 135 cases.
Adults ≥18 years with hematologic malignancies (Zoster-039): 2 vs. 14 cases. Vaccine efficacy was calculated post-hoc.
Vaccine efficacy results against HZ are presented in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageApproximately 13,000 subjects with underlying medical conditions, including conditions associated with a higher risk of HZ, were enrolled in ZOE-50 and ZOE-70. Post-hoc analysis of efficacy against confirmed HZ undertaken in patients with common conditions (chronic kidney disease, chronic obstructive pulmonary disease, coronary artery disease, depression or diabetes mellitus), indicates that the vaccine efficacy is aligned with the overall HZ efficacy.
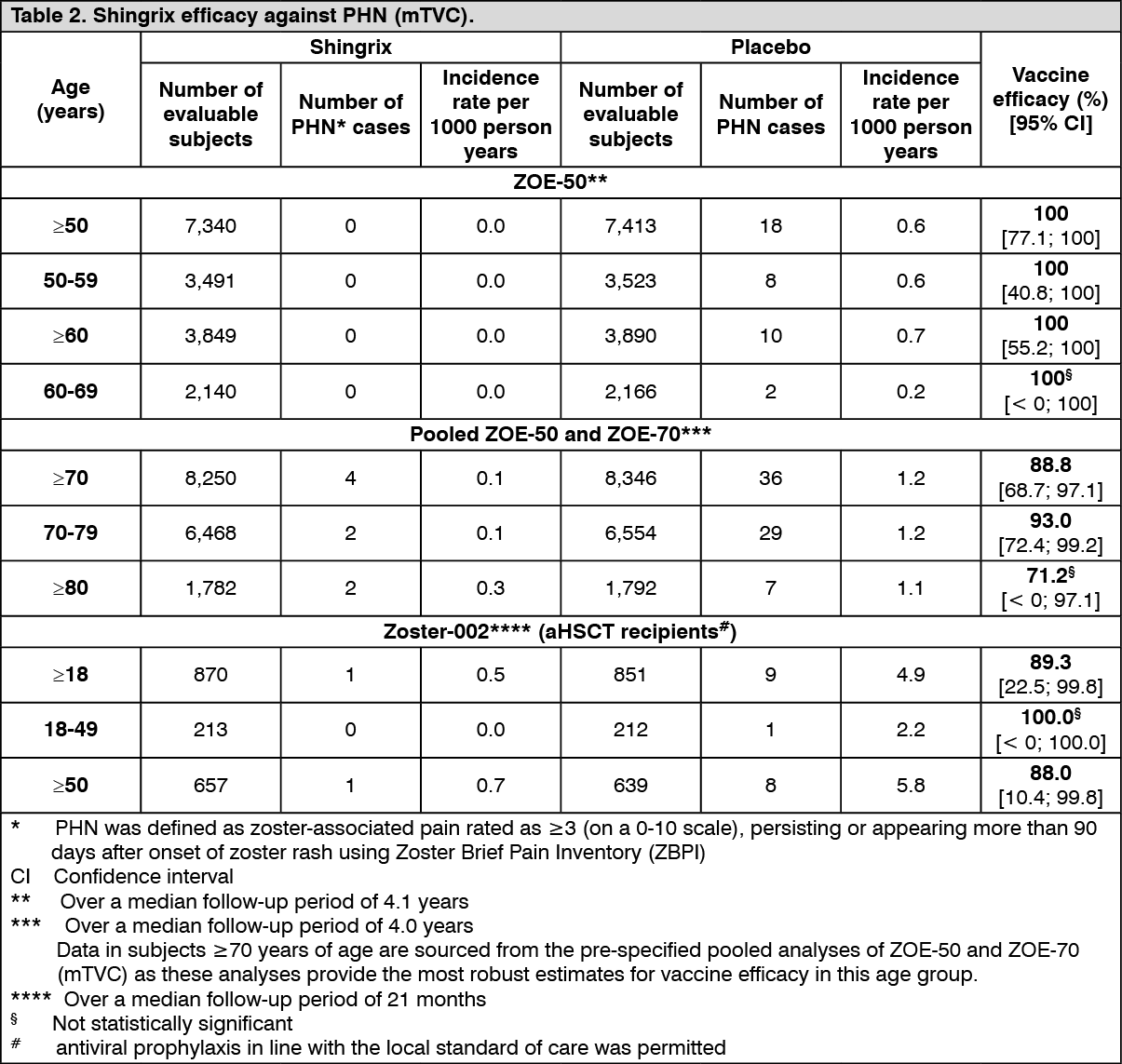
Shingrix significantly decreased the incidence of PHN compared with placebo in: Adults ≥50 years (ZOE-50): 0 vs. 18 cases.
Adults ≥70 years (pooled analysis of ZOE-50 and ZOE-70): 4 vs. 36 cases.
Adults ≥18 years with aHSCT (Zoster-002): 1 vs. 9 cases.
Vaccine efficacy results against PHN are presented in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe benefit of Shingrix in the prevention of PHN can be attributed to the effect of the vaccine on the prevention of HZ. A further reduction of PHN incidence in subjects with confirmed HZ could not be demonstrated due to the limited number of HZ cases in the vaccine group.
In the fourth year after vaccination, the efficacy against HZ was 93.1% (95% CI: 81.2; 98.2) and 87.9% (95% CI: 73.3; 95.4) in adults ≥50 years (ZOE-50) and adults ≥70 years (pooled ZOE-50 and ZOE-70), respectively.
The duration of protection beyond 4 years is currently under investigation.
In Zoster-002, during a follow-up period starting 1 month post-dose 2 (i.e. corresponding to approximately 6 months after aHSCT) until 1 year after aHSCT, when the risk for HZ is the highest, the efficacy against HZ was 76.2% (95% CI: 61.1; 86.0).
Efficacy against HZ-related complications other than PHN: The evaluated HZ-related complications (other than PHN) were: HZ vasculitis, disseminated disease, ophthalmic disease, neurologic disease including stroke, and visceral disease. In the pooled analysis of ZOE-50 and ZOE-70, Shingrix significantly reduced these HZ-related complications by 93.7% (95% CI: 59.5; 99.9) and 91.6% (95% CI: 43.3; 99.8) in adults ≥50 years (1 vs. 16 cases) and adults ≥70 years (1 vs. 12 cases), respectively. No cases of visceral disease or stroke were reported during these studies.
In Zoster-002, Shingrix significantly reduced HZ-related complications by 77.8% (95% CI: 19.0; 96.0) in aHSCT recipients ≥18 years (3 vs 13 cases).
In addition, in Zoster-002, Shingrix significantly reduced HZ-related hospitalisations by 84.7% (95% CI: 32.1; 96.6) (2 vs. 13 cases).
Effect of Shingrix on HZ-related pain: Overall in ZOE-50 and ZOE-70, there was a general trend towards less severe HZ-related pain in subjects vaccinated with Shingrix compared to placebo. As a consequence of the high vaccine efficacy against HZ, a low number of breakthrough cases were accrued, and it was therefore not possible to draw firm conclusions on these study objectives.
In subjects ≥70 years with at least one confirmed HZ episode (ZOE-50 and ZOE-70 pooled), Shingrix significantly reduced the use and the duration of HZ-related pain medication by 39.0% (95% CI: 11.9; 63.3) and 50.6% (95% CI: 8.8; 73.2), respectively. The median duration of pain medication use was 32.0 and 44.0 days in the Shingrix and placebo group, respectively.
In subjects with at least one confirmed HZ episode, Shingrix significantly reduced the maximum average pain score versus placebo over the entire HZ episode (mean = 3.9 vs. 5.5, P-value = 0.049 and mean = 4.5 vs. 5.6, P-value = 0.043, in subjects ≥50 years (ZOE-50) and ≥70 years (ZOE-50 and ZOE-70 pooled), respectively). In addition, in subjects ≥70 years (ZOE-50 and ZOE-70 pooled), Shingrix significantly reduced the maximum worst pain score versus placebo over the entire HZ episode (mean = 5.7 vs. 7.0, P-value = 0.032).
The burden-of-illness (BOI) score incorporates the incidence of HZ with the severity and duration of acute and chronic HZ-related pain over a 6-month period following rash onset. The efficacy in reducing BOI was 98.4% (95% CI: 92.2; 100) in subjects ≥50 years (ZOE-50) and 92.1% (95% CI: 90.4; 93.8) in subjects ≥70 years (ZOE-50 and ZOE-70 pooled).
In Zoster-002, Shingrix significantly reduced the duration of severe 'worst' HZ-associated pain by 38.5% (95% CI: 11.0; 57.6) in aHSCT recipients ≥18 years with at least one confirmed HZ episode. Shingrix significantly reduced the maximum average pain score versus placebo over the entire HZ episode (mean = 4.7 vs. 5.7, P-value = 0.018) and the maximum worst pain score versus placebo over the entire HZ episode (mean = 5.8 vs. 7.1, P-value = 0.011).
The percentage of subjects with at least one confirmed HZ episode in Zoster-002 using at least one pain medication was 65.3% and 69.6% in the Shingrix and placebo group, respectively. The median duration of pain medication use was 21.5 and 47.5 days in the Shingrix and placebo group, respectively. Additionally, in Zoster-002, the efficacy in reducing BOI score was 82.5% (95% CI: 73.6%, 91.4%).
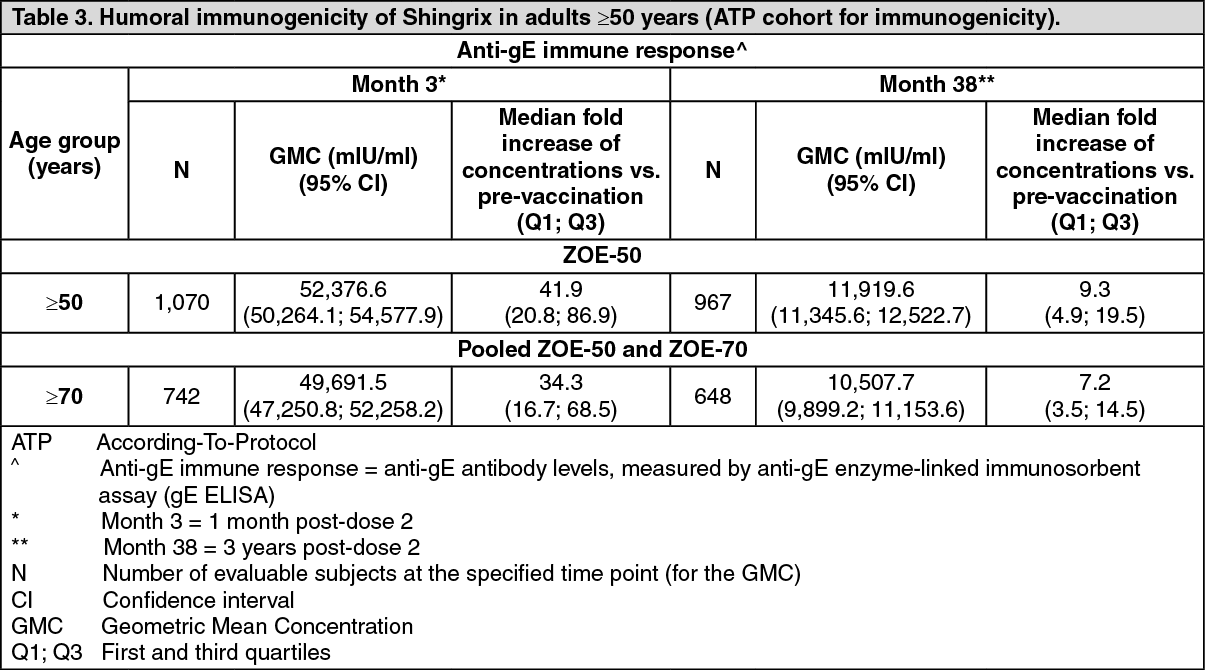
Immunogenicity of Shingrix: An immunological correlate of protection has not been established; therefore, the level of immune response that provides protection against HZ is unknown.
In adults ≥50 years, the immune responses to Shingrix, given as 2 doses 2 months apart, were evaluated in a subset of subjects from the phase III efficacy studies ZOE-50 [humoral immunity and cell-mediated immunity (CMI)] and ZOE-70 (humoral immunity). The gE-specific immune responses (humoral and CMI) elicited by Shingrix are presented in Tables 3 and 4, respectively. (See Tables 3 and 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image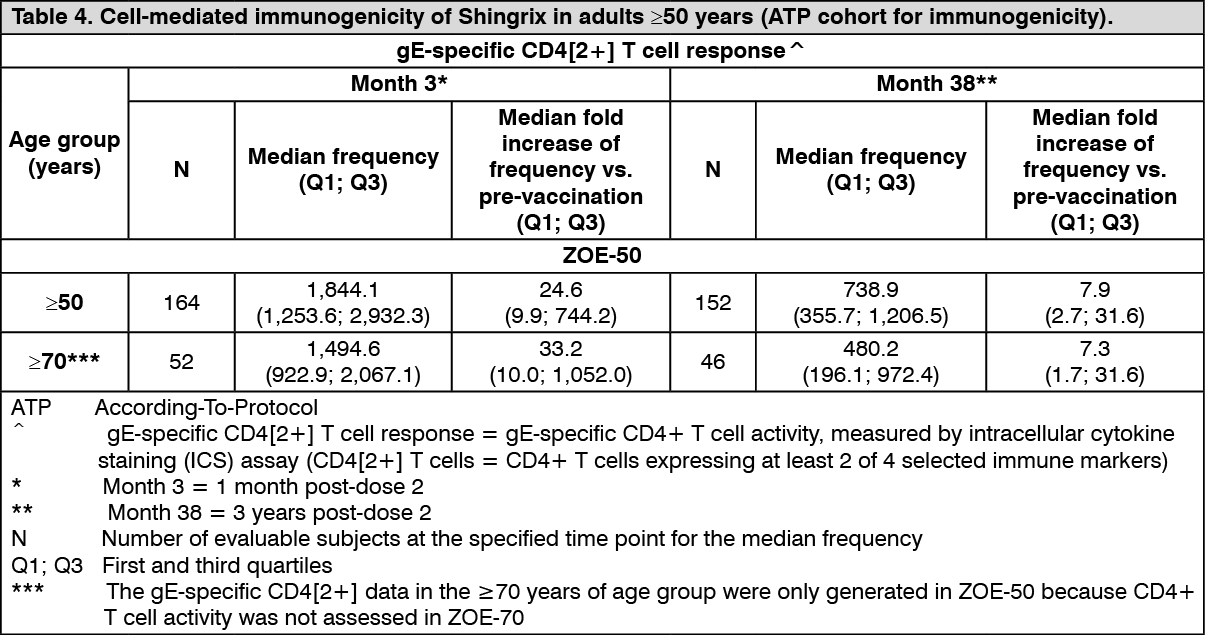 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageData from a phase II, open-label, single group, follow-up clinical study in adults ≥60 years (Zoster-024) indicate that the vaccine-induced immune response (humoral and CMI) persists up to approximately 6 years following a 0, 2-month schedule (N = 119). The median anti-gE antibody concentration was greater than 7-fold above the baseline pre-vaccination median concentration. The median frequency of gE-specific CD4[2+] T cells was greater than 3.7-fold above baseline pre-vaccination median frequency.
In IC adults ≥18 years, the humoral and CMI responses to Shingrix, given as 2 doses 1-2 months apart, were evaluated in: One phase I/II study: Zoster-015 (HIV-infected subjects, the majority (76.42%) being stable on antiretroviral therapy (for at least one year) with a CD4 T-cell count ≥200/mm3).
One phase II/III study: Zoster-028 (patients with solid tumours undergoing chemotherapy).
Three phase III studies: Zoster-002 (aHSCT recipients vaccinated post-transplant), Zoster-039 (patients with hematologic malignancies vaccinated during a cancer therapy course or after the full cancer therapy course) and Zoster-041 (renal transplant recipients on chronic immunosuppressive treatment at the time of vaccination).
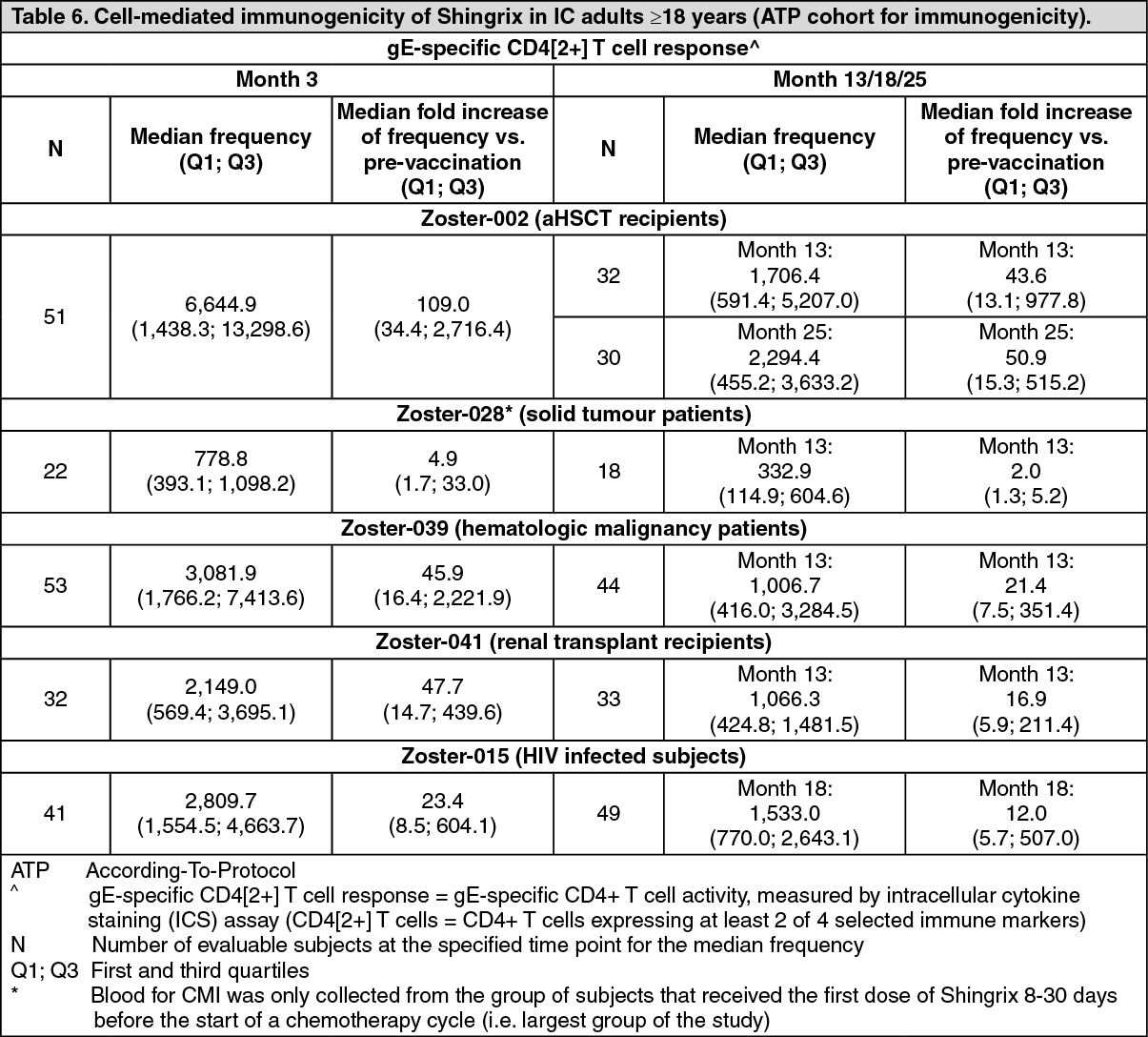
The gE-specific immune responses (humoral and CMI) elicited by Shingrix in all IC populations studied are presented in Tables 5 and 6, respectively. (See Tables 5 and 6.)
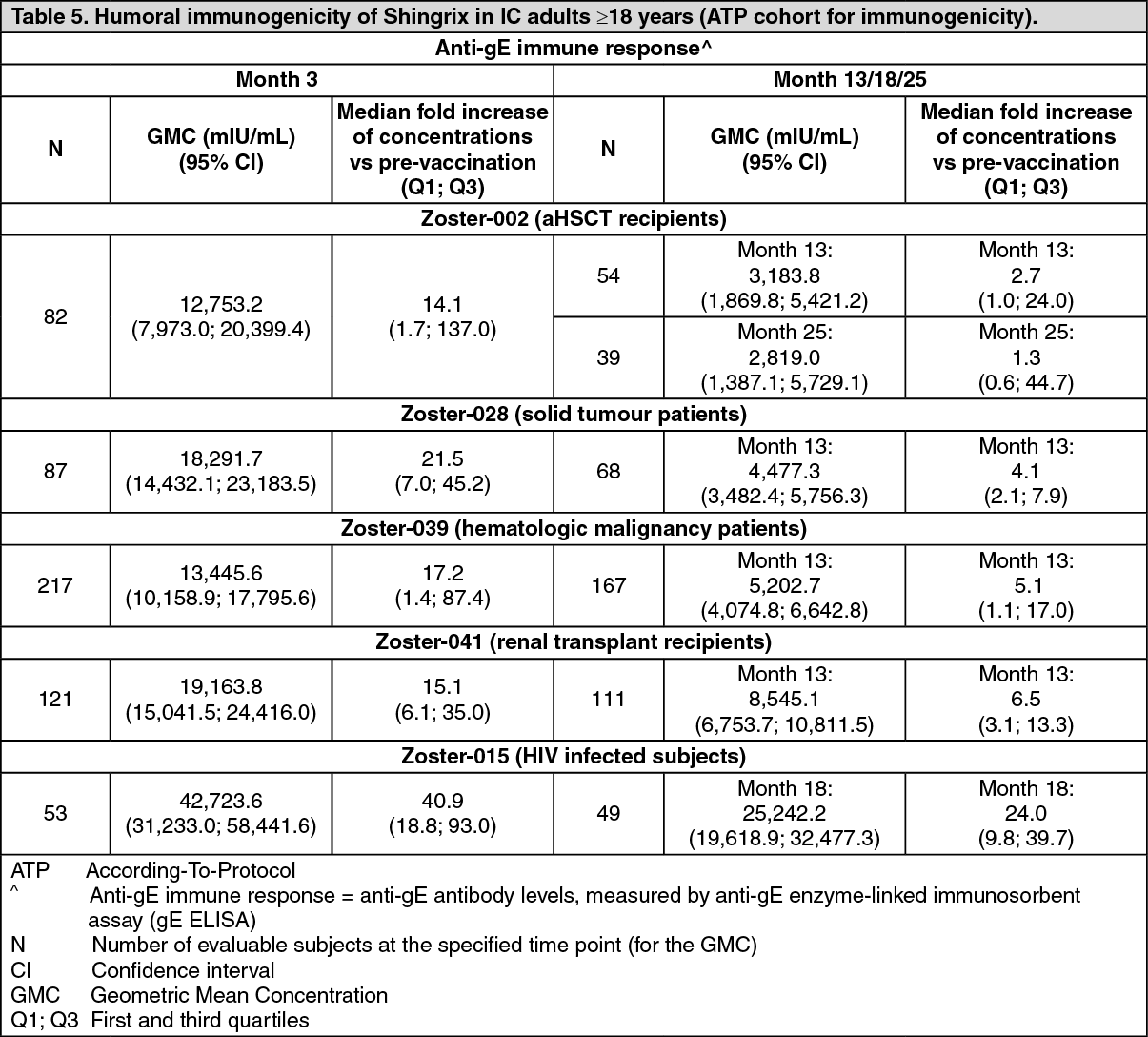 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn Zoster-028, GMC 1-month post Dose 2 were 22,974.3 (19,080.0; 27,663.5) in the group that received the first dose of Shingrix at least 10 days prior to a chemotherapy cycle (PreChemo group) and 9,328.0 (4,492.5; 19,368.2) in the group that received the first dose of Shingrix simultaneously with chemotherapy cycle (OnChemo group). In Zoster-039, GMC 1-month post Dose 2 were 19,934.7 (14,674.1; 27,081.2) in the group that received the first dose of Shingrix after the full cancer therapy course and 5,777.4 (3,342.5; 9,985.9) in the group that received the first dose of Shingrix during a cancer therapy course. The clinical relevance in terms of impact on efficacy, on the short- and long-term, is unknown.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageImmunogenicity in subjects receiving 2 doses of Shingrix 6 months apart: Efficacy has not been assessed for the 0, 6-month schedule. In a phase III, open-label clinical study (Zoster-026) where 238 adults ≥50 years of age were equally randomised to receive 2 doses of Shingrix 2 or 6 months apart, the humoral immune response following the 0, 6-month schedule was demonstrated to be non-inferior to the response with the 0, 2-month schedule. The anti-gE GMC at 1 month after the last vaccine dose was 38,153.7 mIU/ml (95% CI: 34,205.8; 42,557.3) and 44,376.3 mIU/ml (95% CI: 39,697.0; 49,607.2) following the 0, 6-month schedule and the 0, 2-month schedule, respectively.
Subjects with a history of HZ prior to vaccination: Subjects with a history of HZ were excluded from ZOE-50 and ZOE-70. In a phase III, uncontrolled, open-label clinical study (Zoster-033), 96 adults ≥50 years of age with a physician-documented history of HZ received 2 doses of Shingrix 2 months apart. Laboratory confirmation of HZ cases was not part of the study procedures. The anti-gE GMC at 1 month after the last vaccine dose was 47,758.7 mIU/ml (95% CI: 42,258.8; 53,974.4). There were 9 reports of suspected HZ in 6 subjects over a one-year follow-up period. This is a higher recurrence rate than generally reported in observational studies in unvaccinated individuals with a history of HZ. (See Precautions.)
Immunogenicity in individuals previously vaccinated with live attenuated herpes zoster (HZ) vaccine: In a phase III, open-label, multicentre clinical study (Zoster-048), a 2-dose schedule of Shingrix 2 months apart was assessed in 215 adults ≥65 years of age with a previous history of vaccination with live attenuated HZ vaccine ≥5 years earlier compared to 215 matched subjects who had never received live attenuated HZ vaccine. The immune response to Shingrix was unaffected by prior vaccination with live attenuated HZ vaccine.
Paediatric population: The European Medicines Agency has deferred the obligation to submit the results of studies with Shingrix in one or more subsets of the paediatric population in prevention of Varicella Zoster Virus reactivation (see Dosage & Administration for information on paediatric use).
Pharmacokinetics: Not applicable.
Toxicology: Preclinical safety data: Non-clinical data reveal no special hazard for humans based on conventional studies of acute and repeated dose toxicity, local tolerance, cardiovascular/respiratory safety pharmacology and toxicity to reproduction and development.