


 Sign Out
Sign Out

Many of the adverse reactions listed in the following table occur commonly (nausea, vomiting, diarrhoea, fever, lethargy, rash) in patients with abacavir hypersensitivity. Therefore, patients with any of these symptoms should be carefully evaluated for the presence of this hypersensitivity (see Precautions). Very rarely cases of erythema multiforme, Stevens-Johnson syndrome or toxic epidermal necrolysis have been reported where abacavir hypersensitivity could not be ruled out. In such cases medicinal products containing abacavir should be permanently discontinued.
The most severe adverse event possibly related to the treatment with dolutegravir and abacavir/lamivudine, seen in individual patients, was a hypersensitivity reaction that included rash and severe liver effects (see Description of selected adverse reactions as follows and Warnings).
Tabulated list of adverse reactions: The adverse reactions considered at least possibly related to treatment with the components of Triumeq from clinical study and post-marketing experience are listed in Table 6 by body system, organ class and absolute frequency. Frequencies are defined as very common (≥ 1/10), common (≥ 1/100 to < 1/10), uncommon (≥ 1/1000 to < 1/100), rare (≥ 1/10,000 to < 1/1000), very rare (< 1/10,000). (See Table 6.)
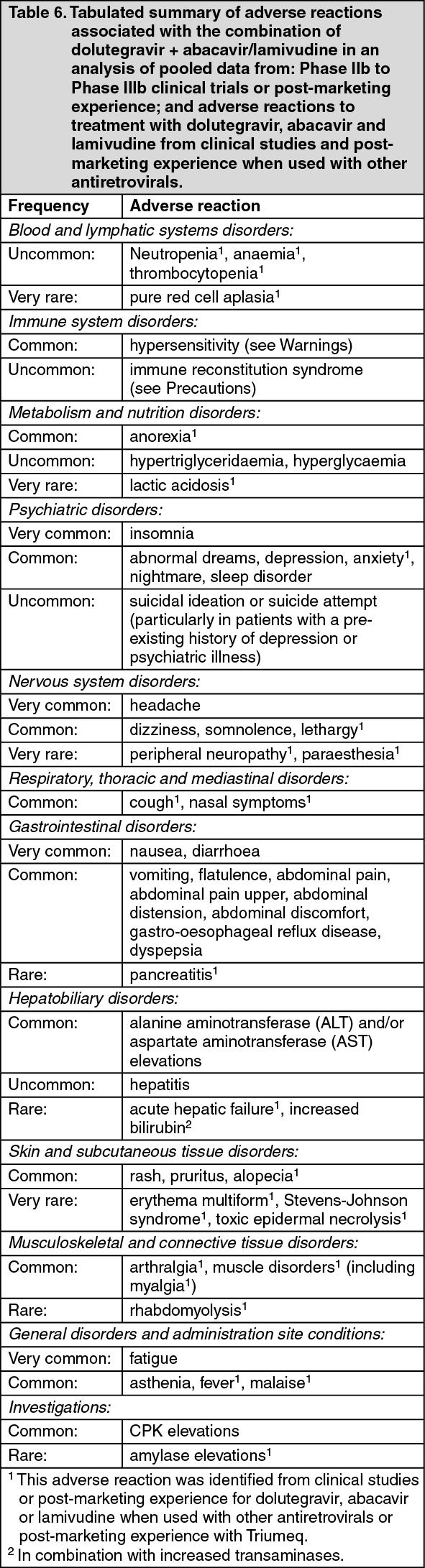 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDescription of selected adverse reactions: Hypersensitivity reactions: Both abacavir and dolutegravir are associated with a risk for hypersensitivity reactions (HSR), which were observed more commonly with abacavir. Hypersensitivity reaction observed for each of these medicinal products (described as follows) share some common features such as fever and/or rash with other symptoms indicating multi-organ involvement. Time to onset was typically 10-14 days for both abacavir and dolutegravir-associated reactions, although reactions to abacavir may occur at any time during therapy. Treatment with Triumeq must be stopped without delay if HSR cannot be ruled out on clinical grounds, and therapy with Triumeq or other abacavir or dolutegravir containing products must never be re-initiated. Please refer to Warnings for further details on patient management in the event of a suspected HSR to Triumeq.
Dolutegravir hypersensitivity: Symptoms have included rash, constitutional findings, and sometimes, organ dysfunction, including severe liver reactions.
Abacavir hypersensitivity: The signs and symptoms of this HSR are listed as follows. These have been identified either from clinical studies or post marketing surveillance. Those reported in at least 10% of patients with a hypersensitivity reaction are in bold text.
Almost all patients developing hypersensitivity reactions will have fever and/or rash (usually maculopapular or urticarial) as part of the syndrome, however reactions have occurred without rash or fever. Other key symptoms include gastrointestinal, respiratory or constitutional symptoms such as lethargy and malaise.
Skin: Rash (usually maculopapular or urticarial).
Gastrointestinal tract: Nausea, vomiting, diarrhoea, abdominal pain, mouth ulceration.
Respiratory tract: Dyspnoea, cough, sore throat, adult respiratory distress syndrome, respiratory failure.
Miscellaneous: Fever, lethargy, malaise, oedema, lymphadenopathy, hypotension, conjunctivitis, anaphylaxis.
Neurological/Psychiatry: Headache, paraesthesia.
Haematological: Lymphopenia.
Liver/pancreas: Elevated liver function tests, hepatitis, hepatic failure.
Musculoskeletal: Myalgia, rarely myolysis, arthralgia, elevated creatine phosphokinase.
Urology: Elevated creatinine, renal failure.
Symptoms related to this HSR worsen with continued therapy and can be life-threatening and in rare instance, have been fatal.
Restarting abacavir following an abacavir HSR results in a prompt return of symptoms within hours. This recurrence of the HSR is usually more severe than on initial presentation, and may include life-threatening hypotension and death. Similar reactions have also occurred infrequently after restarting abacavir in patients who had only one of the key symptoms of hypersensitivity (see as previously mentioned) prior to stopping abacavir; and on very rare occasions have also been seen in patients who have restarted therapy with no preceding symptoms of a HSR (i.e., patients previously considered to be abacavir tolerant).
Metabolic parameters: Weight and levels of blood lipids and glucose may increase during antiretroviral therapy (see Precautions).
Osteonecrosis: Cases of osteonecrosis have been reported, particularly in patients with generally acknowledged risk factors, advanced HIV disease or long-term exposure to CART. The frequency of this is unknown (see Precautions).
Immune reactivation syndrome: In HIV-infected patients with severe immune deficiency at the time of initiation of CART, an inflammatory reaction to asymptomatic or residual opportunistic infections may arise. Autoimmune disorders (such as Graves' disease and autoimmune hepatitis) have also been reported; however, the reported time to onset is more variable and these events can occur many months after initiation of treatment (see Precautions).
Changes in laboratory chemistries: Increases in serum creatinine occurred within the first week of treatment with dolutegravir and remained stable through 96 weeks. In the SINGLE study a mean change from baseline of 12.6 μmol/L was observed after 96 weeks of treatment. These changes are not considered to be clinically relevant since they do not reflect a change in glomerular filtration rate.
Asymptomatic creatine phosphokinase (CPK) elevations mainly in association with exercise have also been reported with dolutegravir therapy.
Co-infection with Hepatitis B or C: In dolutegravir Phase III studies patients with hepatitis B and/or C co-infection were permitted to enrol provided that baseline liver chemistry tests did not exceed 5 times the upper limit of normal (ULN). Overall, the safety profile in patients co-infected with hepatitis B and/or C was similar to that observed in patients without hepatitis B or C co-infection, although the rates of AST and ALT abnormalities were higher in the subgroup with hepatitis B and/or C co-infection for all treatment groups.
Paediatric population: There are no clinical study data on the effects of Triumeq in the paediatric population. Individual components have been investigated in adolescents (12 to 17 years).
Based on limited available data with the dolutegravir single entity used in combination with other antiretroviral agents to treat adolescents (12 to 17 years), there were no additional types of adverse reactions beyond those observed in the adult population.
The individual preparations of abacavir and lamivudine have been investigated separately, and as a dual nucleoside backbone, in combination antiretroviral therapy to treat ART-naive and ART-experienced HIV-infected paediatric patients (data available on the use of abacavir and lamivudine in infants less than three months are limited). No additional types of adverse reactions have been observed beyond those characterised for the adult population.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product.
View ADR Monitoring Form