


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Dolutegravir inhibits HIV integrase by binding to the integrase active site and blocking the strand transfer step of retroviral Deoxyribonucleic acid (DNA) integration which is essential for the HIV replication cycle.
Abacavir and lamivudine are potent selective inhibitors of HIV-1 and HIV-2. Both abacavir and lamivudine are metabolised sequentially by intracellular kinases to the respective 5'-triphosphates (TP) which are the active moieties with extended intracellular half-lives supporting once daily dosing (see Pharmacokinetics as follows). Lamivudine-TP (an analogue for cytidine) and carbovir-TP (the active triphosphate form of abacavir, an analogue for guanosine) are substrates for and competitive inhibitors of HIV reverse transcriptase (RT). However, their main antiviral activity is through incorporation of the monophosphate form into the viral DNA chain, resulting in chain termination. Abacavir and lamivudine triphosphates show significantly less affinity for host cell DNA polymerases.
Pharmacodynamic effects: Antiviral activity in vitro: Dolutegravir, abacavir and lamivudine have been shown to inhibit replication of lab-strains and clinical isolates of HIV in a number of cell types, including transformed T cell lines, monocyte/macrophage derived lines and primary cultures of activated peripheral blood mononuclear cells (PMBCs) and monocyte/macrophages. The concentration of active substance necessary to effect viral replication by 50% (IC50 - half maximal inhibitory concentration) varied according to virus and host cell type.
The IC50 for dolutegravir in various lab-strains using PBMC was 0.5 nM, and when using MT-4 cells it ranged from 0.7-2 nM. Similar IC50s were seen for clinical isolates without any major difference between subtypes; in a panel of 24 HIV-1 isolates of clades A, B, C, D, E, F and G and group O the mean IC50 value was 0.2 nM (range 0.02-2.14). The mean IC50 for 3 HIV-2 isolates was 0.18 nM (range 0.09-0.61).
The mean IC50 for abacavir against lab-strains of HIV-1IIIB and HIV-1HXB2 ranged from 1.4 to 5.8 μM. The median or mean IC50 values for lamivudine against lab-strains of HIV-1 ranged from 0.007 to 2.3 μM. The mean IC50 against lab-strains of HIV-2 (LAV2 and EHO) ranged from 1.57 to 7.5 μM for abacavir and from 0.16 to 0.51 μM for lamivudine.
The IC50 values of abacavir against HIV-1 Group M subtypes (A-G) ranged from 0.002 to 1.179 μM, against Group O from 0.022 to 1.21 μM, and against HIV-2 isolates, from 0.024 to 0.49 μM. For lamivudine, the IC50 values against HIV-1 subtypes (A-G) ranged from 0.001 to 0.170 μM, against Group O from 0.030 to 0.160 μM and against HIV-2 isolates from 0.002 to 0.120 μM in peripheral blood mononuclear cells.
HIV-1 isolates (CRF01_AE, n=12; CRF02_AG, n=12; and Subtype C or CRF_AC, n=13) from 37 untreated patients in Africa and Asia were susceptible to abacavir (IC50 fold changes < 2.5), and lamivudine (IC50 fold changes < 3.0), except for two CRF02_AG isolates with fold changes of 2.9 and 3.4 for abacavir. Group O isolates from antiviral naïve patients tested for lamivudine activity were highly sensitive.
The combination of abacavir and lamivudine has demonstrated antiviral activity in cell culture against non-subtype B isolates and HIV-2 isolates with equivalent antiviral activity as for subtype B isolates.
Antiviral activity in combination with other antiviral agents: No antagonistic effects in vitro were seen with dolutegravir and other antiretrovirals (tested agents: stavudine, abacavir, efavirenz, nevirapine, lopinavir, amprenavir, enfuvirtide, maraviroc, adefovir and raltegravir). In addition, ribavirin had no apparent effect on dolutegravir activity.
The antiviral activity of abacavir in cell culture was not antagonized when combined with the nucleoside reverse transcriptase inhibitors (NRTIs) didanosine, emtricitabine, lamivudine, stavudine, tenofovir, zalcitabine or zidovudine, the non-nucleoside reverse transcriptase inhibitor (NNRTI) nevirapine, or the protease inhibitor (PI) amprenavir.
No antagonistic effects in vitro were seen with lamivudine and other antiretrovirals (tested agents: abacavir, didanosine, nevirapine, zalcitabine, and zidovudine).
Effect of human serum: In 100% human serum, the mean fold shift for dolutegravir activity was 75-fold, resulting in protein adjusted IC90 of 0.064 ug/mL. Plasma protein binding studies in vitro indicate that abacavir binds only low to moderately (~49%) to human plasma proteins at therapeutic concentrations. Lamivudine exhibits linear pharmacokinetics over the therapeutic dose range and displays low plasma protein binding (less than 36%).
Resistance: Resistance in vitro: (dolutegravir): Serial passage is used to study resistance evolution in vitro. When using the lab-strain HIVIII during passage over 112 days, mutations selected appeared slowly, with substitutions at positions S153Y and F. These mutations were not selected in patients treated with dolutegravir in the clinical studies. Using strain NL432 mutations E92Q (fold change 3) and G193E (fold change 3) were selected. These mutations have been selected in patients with pre-existing raltegravir resistance and who were then treated with dolutegravir (listed as secondary mutations for dolutegravir).
In further selection experiments using clinical isolates of subtype B, mutation R263K was seen in all five isolates (after 20 weeks and onwards). In subtype C (n=2) and A/G (n=2) isolates the integrase substitution R263K was selected in one isolate, and G118R in two isolates. R263K was reported from two individual patients with subtype B and subtype C in the clinical program for ART experienced, INI naive subjects, but without effects on dolutegravir susceptibility in vitro. G118R lowers the susceptibility to dolutegravir in site directed mutants (fold change 10), but was not detected in patients receiving dolutegravir in the Phase III program.
Primary mutations for raltegravir/elvitegravir (Q148H/R/K, N155H, Y143R/H/C, E92Q, T66I) do not affect the in vitro susceptibility of dolutegravir as single mutations. When mutations listed as secondary integrase inhibitor associated mutations (for raltegravir/elvitegravir) are added to primary mutations (excluding at Q148) in experiments with site directed mutants, dolutegravir susceptibility remains at or near wildtype level. In the case of the Q148-mutation viruses, increasing dolutegravir fold change is seen as the number of secondary mutations increase. The effect of the Q148-based mutations (H/R/K) was also consistent with in vitro passage experiments with site directed mutants. In serial passage with strain NL432-based site directed mutants at N155H or E92Q, no further selection of resistance was seen (fold change unchanged around 1). In contrast, starting passage with mutants with mutation Q148H (fold change 1), a variety of raltegravir associated secondary mutations accumulated with a consequent increase of fold change to values >10.
A clinically relevant phenotypic cut-off value (fold change vs wild type virus) has not been determined; genotypic resistance was a better predictor for outcome.
Seven hundred and five raltegravir resistant isolates from raltegravir experienced patients were analyzed for susceptibility to dolutegravir. Dolutegravir has a <10-fold change against 94% of the 705 clinical isolates.
Resistance in vivo: (dolutegravir): In previously untreated patients receiving dolutegravir + 2 NRTIs in Phase IIb and Phase III, no development of resistance to the integrase class, or to the NRTI class was seen (n=876, follow-up of 48-96 weeks).
In patients with prior failed therapies, but naïve to the integrase class (SAILING study), integrase inhibitor substitutions were observed in 4/354 patients (follow-up 48 weeks) treated with dolutegravir, which was given in combination with an investigator selected background regimen (BR). Of these four, two subjects had a unique R263K integrase substitution, with a maximum fold change of 1.93, one subject had a polymorphic V151V/I integrase substitution, with maximum fold change of 0.92, and one subject had pre-existing integrase mutations and is assumed to have been integrase experienced or infected with integrase resistant virus by transmission. The R263K mutation was also selected in vitro (see as previously mentioned).
Resistance in vitro and in vivo: (abacavir and lamivudine): Abacavir-resistant isolates of HIV-1 have been selected in vitro and in vivo and are associated with specific genotypic changes in the RT codon region (codons M184V, K65R, L74V and Y115F). During in vitro abacavir selection the M184V mutation occurred first and resulted in about a 2-fold increase in IC50, below the abacavir clinical cut-off of 4.5-fold change. Continued passage in increasing concentrations of drug resulted in selection for double RT mutants 65R/184V and 74V/184V or triple RT mutant 74V/115Y/184V. Two mutations conferred a 7 to 8-fold change in abacavir susceptibility and combinations of three mutations were required to confer more than an 8-fold change in susceptibility.
HIV-1 resistance to lamivudine involves the development of a M184I or M184V amino acid change close to the active site of the viral RT. This variant arises both in vitro and in HIV-1 infected patients treated with lamivudine-containing antiretroviral therapy. M184V mutants display greatly reduced susceptibility to lamivudine and show diminished viral replicative capacity in vitro. M184V is associated with about a 2-fold increase in abacavir resistance but does not confer clinical resistance for abacavir.
Isolates resistant to abacavir may also show reduced sensitivity to lamivudine. The combination of abacavir/lamivudine has demonstrated decreased susceptibility to viruses with the substitutions K65R with or without the M184V/I substitution, and to viruses with L74V plus the M184V/I substitution.
Cross-resistance between dolutegravir or abacavir or lamivudine and antiretrovirals from other classes e.g. PIs or NNRTIs is unlikely.
Effects on electrocardiogram: No relevant effects were seen on the QTc interval, with doses of dolutegravir exceeding the clinical dose by approximately 3-fold. Similar studies were not conducted with either abacavir or lamivudine.
Clinical efficacy and safety: The efficacy of Triumeq in HIV-infected, therapy naive subjects is based on the analyses of data from a number of trials. The analyses included two randomized, international, double-blind, active-controlled trials, SINGLE (ING114467) and SPRING-2 (ING113086), the international, open-label, active-controlled trial FLAMINGO (ING114915), and the randomized, open-label, active-controlled, multicentre, non-inferiority study ARIA (ING117172).
The STRIIVING study (201147), was a randomized, open-label, active-controlled, multicentre, non-inferiority switch study in virologically suppressed subjects with no documented history of resistance to any class.
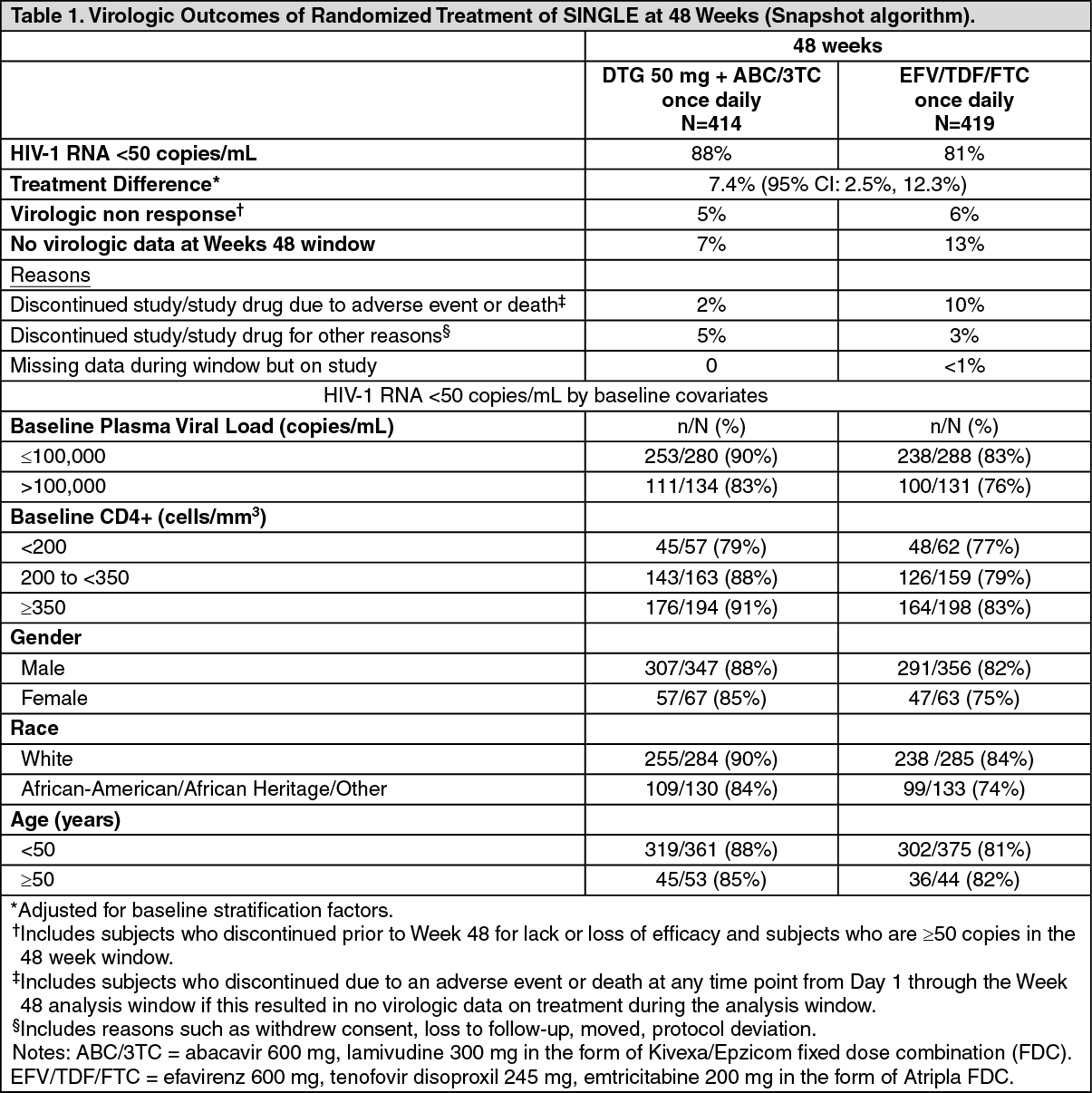
In SINGLE, 833 patients were treated with dolutegravir 50 mg once daily plus fixed-dose abacavir-lamivudine (DTG + ABC/3TC) or fixed-dose efavirenz-tenofovir-emtricitabine (EFV/TDF/FTC). At baseline, median patient age was 35 years, 16% were female, 32% non-white, 7% had hepatitis C co-infection and 4% were CDC Class C, these characteristics were similar between treatment groups. Week 48 outcomes (including outcomes by key baseline covariates) are shown in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn the primary 48 weeks analysis, the proportion of patients with virologic suppression in the dolutegravir + ABC/3TC arm, was superior to the EFV/TDF/FTC arm, p=0.003, the same treatment difference was observed in subjects defined by baseline HIV RNA level (< or > 100,000 copies/mL). The median time to viral suppression was shorter with ABC/3TC + DTG (28 vs 84 days, p<0.0001). The adjusted mean change in CD4+ T cell count from baseline were 267 cells versus 208 cells/mm3, respectively (p<0.001). Both the time to viral suppression and change from baseline analyses were pre-specified and adjusted for multiplicity. At 96 weeks, the response was 80% vs 72%, respectively. The difference in the endpoint remained statistically significant (p=0.006). The statistically higher responses on DTG+ABC/3TC were driven by a higher rate of withdrawals due to AEs in the EFV/TDF/FTC arm, irrespective of viral load strata. Overall treatment differences at Week 96 are applicable to patients with high and low Baseline viral loads. At 144 weeks in the open-label phase of SINGLE, virologic suppression was maintained, the DTG +ABC/3TC arm (71%) was superior to the EFV/TDF/FTC arm (63%), treatment difference was 8.3% (2.0, 14.6).
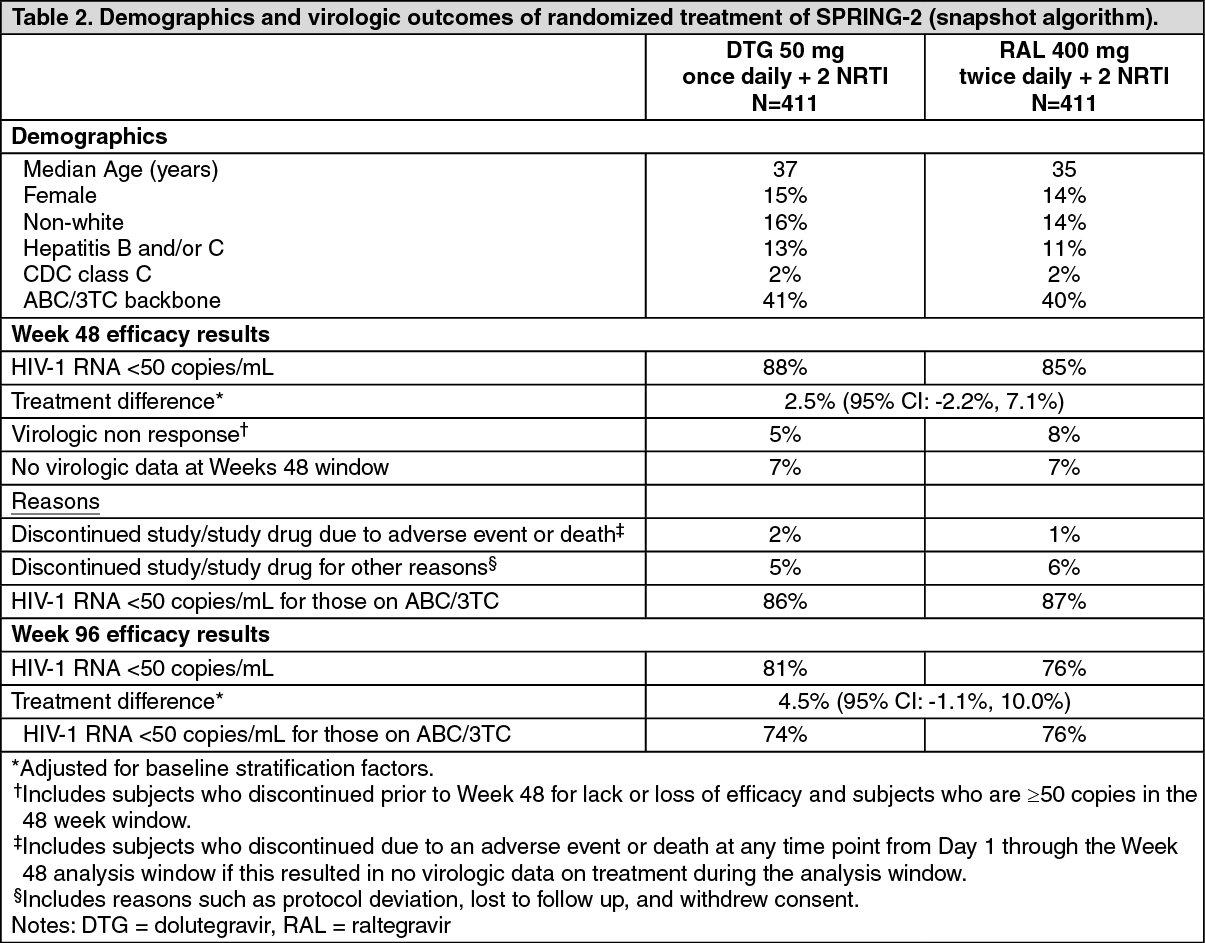
In SPRING-2, 822 patients were treated with either dolutegravir 50 mg once daily or raltegravir 400 mg twice daily (blinded), both with fixed-dose ABC/3TC (around 40%) or TDF/FTC (around 60%), given open label. Baseline demographics and outcomes are summarised in Table 2. Dolutegravir was non-inferior to raltegravir, including within the subset of patients with the abacavir/lamivudine background regimen. (See Table 2.)
 Click on icon to see table/diagram/image
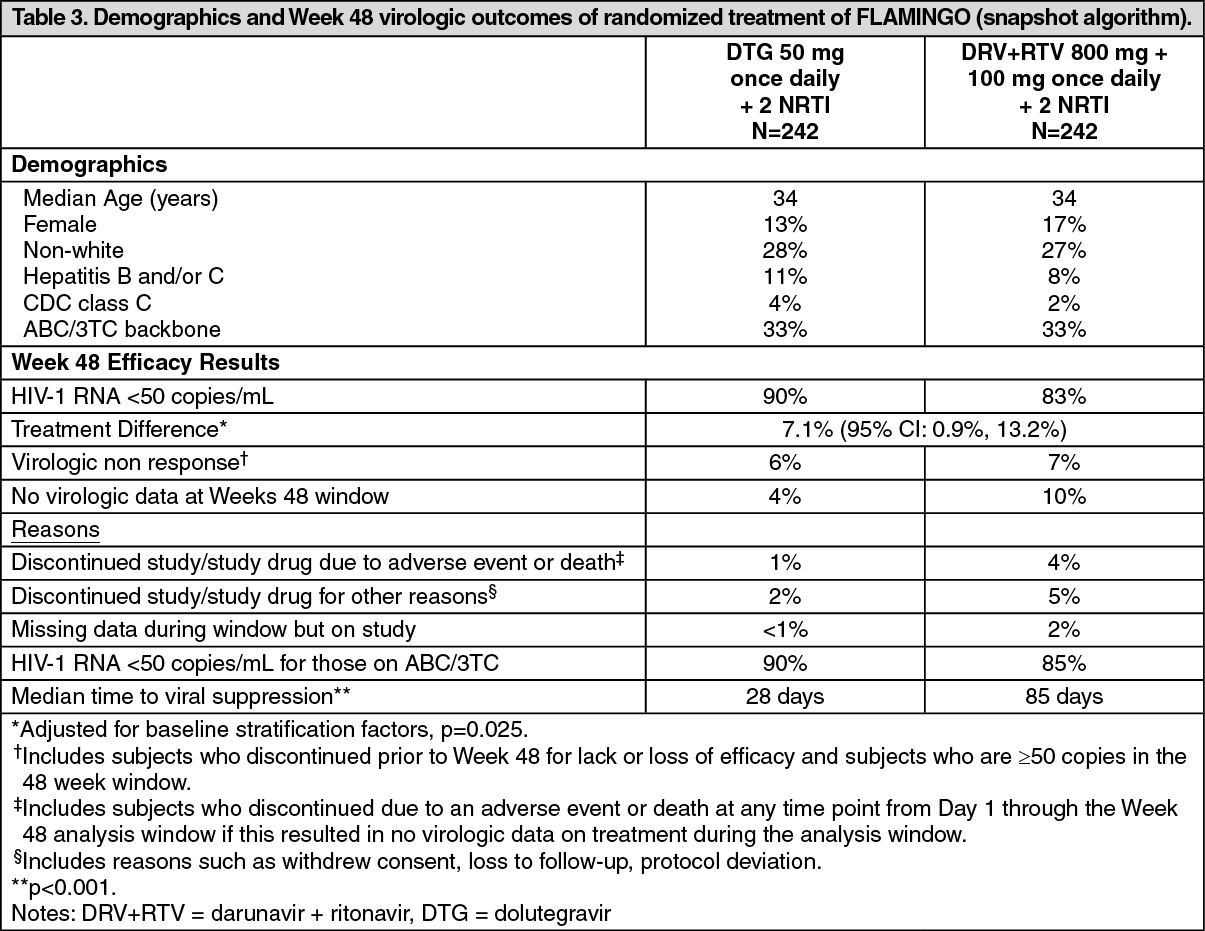
Click on icon to see table/diagram/imageIn FLAMINGO, 485 patients were treated with dolutegravir 50 mg once daily or darunavir/ritonavir (DRV/r) 800 mg/100 mg once daily, both with ABC/3TC (around 33%) or TDF/FTC (around 67%). All treatments were given open-label. Main demographics and outcomes are summarised in Table 3. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAt 96 weeks, virologic suppression in the dolutegravir group (80%) was superior to the DRV/r group (68%), (adjusted treatment difference [DTG-(DRV+RTV)]: 12.4%; 95% CI: [4.7, 20.2]). Response rates at 96 weeks were 82% for DTG+ABC/3TC and 75% for DRV/r+ABC/3TC.
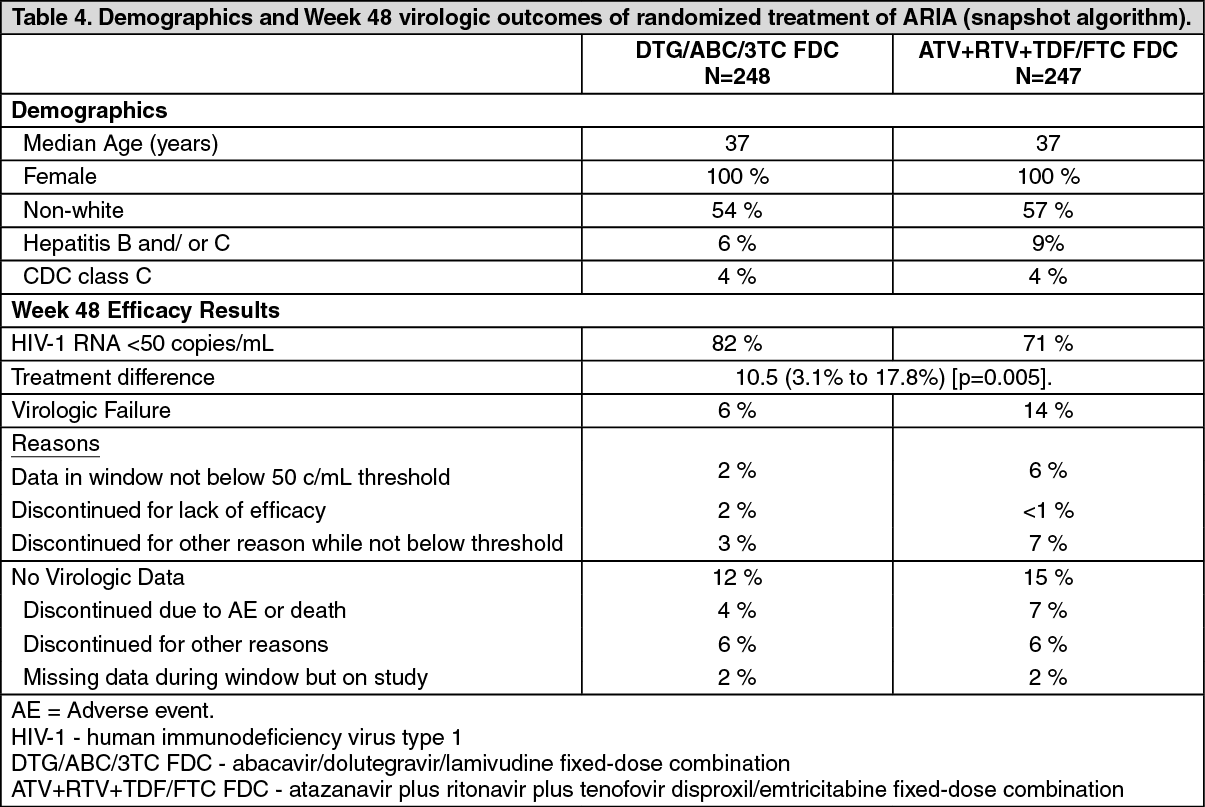
In ARIA (ING117172), a randomized, open-label, active-controlled, multicenter, parallel group, non-inferiority study; 499 HIV-1 infected ART naïve adult women were randomized 1:1 to receive either; DTG/ABC/3TC FDC 50 mg/600 mg/300 mg; or atazanavir 300 mg plus ritonavir 100 mg plus tenofovir disproxil / emtricitabine 245 mg/200 mg (ATV+RTV+TDF/FTC FDC), all administered once daily. (See Table 4.)
 Click on icon to see table/diagram/image
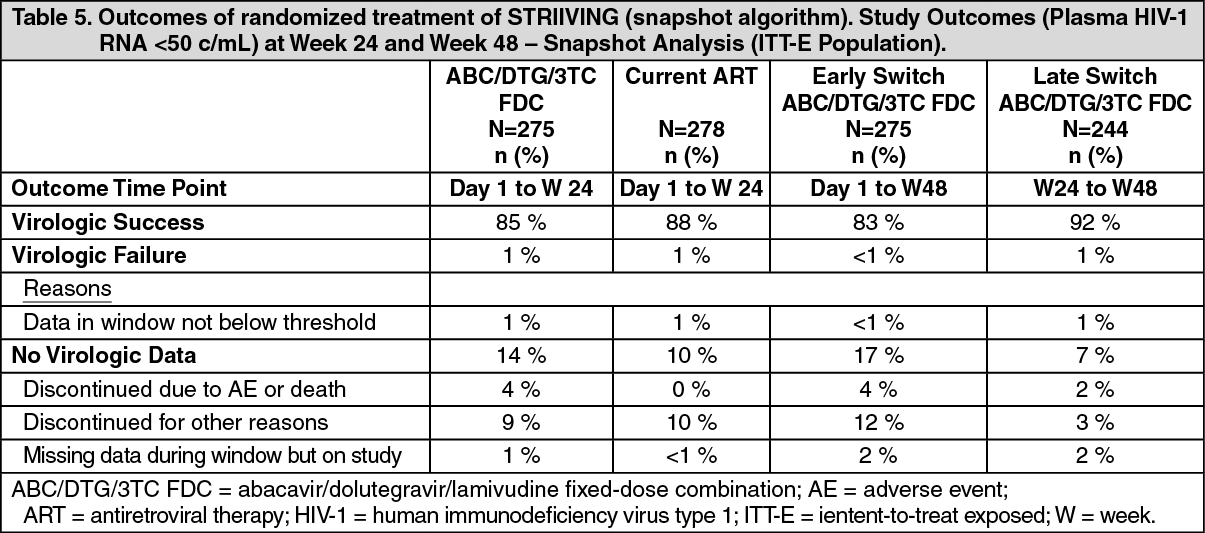
Click on icon to see table/diagram/imageSTRIIVING (201147) is a 48-week, randomized, open-label, active controlled, multicenter, non-inferiority study in patients without any prior treatment failure, and without any documented resistance to any class. Virologically suppressed (HIV-1 RNA <50 c/mL) subjects were randomly assigned (1:1) to continue their current ART regimen (2 NRTIs plus either a PI, NNRTI, or INI), or switch to ABC/DTG/3TC FDC once daily (Early Switch). Hepatitis B co-infection was one of main exclusion criteria.
Patients were mainly white (66%) or black (28%) of male sex (87%). Main prior transmission routes were homosexual (73%) or heterosexual (29%) contact. The proportion with a positive HCV serology was 7%. The median time from first starting ART was around 4.5 years. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageVirologic suppression (HIV-1 RNA <50 copies/mL) in the ABC/DTG/3TC FDC group (85%) was statistically non-inferior to the current ART groups (88%) at 24 weeks. The adjusted difference in proportion and 95% CI [ABC/DTG/3TC vs current ART] were 3.4%; 95% CI: [-9.1, 2.4]. After 24 weeks all remaining subjects switched to ABC/DTG/3TC FDC (Late Switch). Similar levels of virologic suppression were maintained in both the Early and Late Switch groups at 48 weeks.
De novo resistance in patients failing therapy in SINGLE, SPRING-2 and FLAMINGO: De novo resistance was not detected to the integrase class or the NRTI class in any patients who were treated with dolutegravir + abacavir/lamivudine in the three studies mentioned.
For the comparators typical resistance was detected with TDF/FTC/EFV (SINGLE; six with NNRTI associated resistance and one with major NRTI resistance) and with 2 NRTIs + raltegravir (SPRING-2; four with major NRTI resistance and one with raltegravir resistance), while no de novo resistance was detected in patients treated with 2 NRTIs + DRV/RTV (FLAMINGO).
Paediatric population: In a Phase I/II 48 week multicentre, open-label study (P1093/ING112578), the pharmacokinetic parameters, safety, tolerability and efficacy of dolutegravir was evaluated in combination regimens in HIV-1 infected infants, children and adolescents.
At 24 weeks, 16 of 23 (69%) adolescents (12 to 17 years of age) treated with dolutegravir once daily (35 mg n=4; 50 mg n=19) plus OBR achieved viral load less than 50 copies/mL.
Twenty out of 23 children and adolescents (87%) had >1 log10 c/mL decrease from Baseline in HIV-1 RNA or HIV-1 RNA <400 c/mL at Week 24. Four subjects had virologic failure none of which had INI resistance at the time of virologic failure.
Pharmacokinetics: The Triumeq tablet has been shown to be bioequivalent to dolutegravir single entity tablet and abacavir/lamivudine fixed-dose combination tablet (ABC/3TC FDC) administered separately. This was demonstrated in a single dose, 2-way crossover bioequivalence study of Triumeq (fasted) versus 1 x 50 mg dolutegravir tablet, plus 1 x 600mg abacavir/300 mg lamivudine tablet (fasted) in healthy subjects (n=66). The effect of a high fat meal on the Triumeq tablet was evaluated in a subgroup of subjects in this study (n=12). Plasma Cmax and AUC of dolutegravir following administration of Triumeq with a high fat meal were 37% and 48% higher, respectively, than those following administration of Triumeq in the fasted state. This is not considered clinically significant (see Absorption as follows). The effect of food on plasma exposures of abacavir and lamivudine following administration of Triumeq with a high fat meal were very similar to prior food effects observed with ABC/3TC FDC. These results indicate that Triumeq can be taken with or without food.
The pharmacokinetic properties of dolutegravir, lamivudine and abacavir are described as follows.
Absorption: Dolutegravir, abacavir and lamivudine are rapidly absorbed following oral administration. The absolute bioavailability of dolutegravir has not been established. The absolute bioavailability of oral abacavir and lamivudine in adults is about 83% and 80-85% respectively. The mean time to maximal serum concentrations (tmax) is about 2 to 3 hours (post dose for tablet formulation), 1.5 hours and 1.0 hour for dolutegravir, abacavir and lamivudine, respectively.
Exposure to dolutegravir was generally similar between healthy subjects and HIV-1-infected subjects. In HIV-1-infected adult subjects following dolutegravir 50 mg once daily, the steady-state pharmacokinetic parameters (geometric mean [%CV]) based on population pharmacokinetic analyses were AUC(0-24) = 53.6 (27) μg.h/mL, Cmax = 3.67 (20) μg/mL, and Cmin = 1.11 (46) μg/mL. Following a single dose of 600 mg of abacavir, the mean (CV) Cmax is 4.26 μg/ml (28%) and the mean (CV) AUC∞ is 11.95 μg.h/ml (21%). Following multiple-dose oral administration of lamivudine 300 mg once daily for seven days, the mean (CV) steady-state Cmax is 2.04 μg/ml (26%) and the mean (CV) AUC24 is 8.87 μg.h/ml (21%).
Plasma Cmax and AUC of dolutegravir following administration of Triumeq with a high fat meal were 37% and 48% higher, respectively, than those following administration of Triumeq in the fasted state. For abacavir there was a decrease in Cmax with 23% and AUC was unchanged. The exposure of lamivudine was similar with and without food. These results indicate that Triumeq can be taken with or without food.
Distribution: The apparent volume of distribution of dolutegravir (following oral administration of suspension formulation, Vd/F) is estimated at 12.5 L. Intravenous studies with abacavir and lamivudine showed that the mean apparent volume of distribution is 0.8 and 1.3 l/kg respectively.
Dolutegravir is highly bound (> 99%) to human plasma proteins based on in vitro data. Binding of dolutegravir to plasma proteins is independent of dolutegravir concentration. Total blood and plasma drug-related radioactivity concentration ratios averaged between 0.441 to 0.535, indicating minimal association of radioactivity with blood cellular components. The unbound fraction of dolutegravir in plasma is increased at low levels of serum albumin (<35 g/L) as seen in subjects with moderate hepatic impairment. Plasma protein binding studies in vitro indicate that abacavir binds only low to moderately (~49%) to human plasma proteins at therapeutic concentrations. Lamivudine exhibits linear pharmacokinetics over the therapeutic dose range and displays limited plasma protein binding in vitro (< 36%).
Dolutegravir, abacavir and lamivudine are present in cerebrospinal fluid (CSF).
In 13 treatment-naïve subjects on a stable dolutegravir plus abacavir/lamivudine regimen, dolutegravir concentration in CSF averaged 18 ng/mL (comparable to unbound plasma concentration, and above the IC50). Studies with abacavir demonstrate a CSF to plasma AUC ratio of between 30 to 44%. The observed values of the peak concentrations are 9-fold greater than the IC50 of abacavir of 0.08 μg/ml or 0.26 μM when abacavir is given at 600 mg twice daily. The mean ratio of CSF/serum lamivudine concentrations 2-4 hours after oral administration was approximately 12%. The true extent of CNS penetration of lamivudine and its relationship with any clinical efficacy is unknown.
Dolutegravir is present in the female and male genital tract. AUC in cervicovaginal fluid, cervical tissue and vaginal tissue were 6-10% of those in corresponding plasma at steady state. AUC in semen was 7% and 17% in rectal tissue of those in corresponding plasma at steady state.
Biotransformation: Dolutegravir is primarily metabolized via UGT1A1 with a minor CYP3A component (9.7% of total dose administered in a human mass balance study). Dolutegravir is the predominant circulating compound in plasma; renal elimination of unchanged active substance is low (< 1% of the dose). Fifty-three percent of total oral dose is excreted unchanged in the faeces. It is unknown if all or part of this is due to unabsorbed active substance or biliary excretion of the glucuronidate conjugate, which can be further degraded to form the parent compound in the gut lumen. Thirty-two percent of the total oral dose is excreted in the urine, represented by ether glucuronide of dolutegravir (18.9% of total dose), N-dealkylation metabolite (3.6% of total dose), and a metabolite formed by oxidation at the benzylic carbon (3.0% of total dose).
Abacavir is primarily metabolised by the liver with approximately 2% of the administered dose being renally excreted, as unchanged compound. The primary pathways of metabolism in man are by alcohol dehydrogenase and by glucuronidation to produce the 5'-carboxylic acid and 5'-glucuronide which account for about 66% of the administered dose. These metabolites are excreted in the urine.
Metabolism of lamivudine is a minor route of elimination. Lamivudine is predominately cleared by renal excretion of unchanged lamivudine. The likelihood of metabolic drug interactions with lamivudine is low due to the small extent of hepatic metabolism (5-10%).
Drug interactions: In vitro, dolutegravir demonstrated no direct, or weak inhibition (IC50>50 μM) of the enzymes cytochrome P450 (CYP)1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP3A, UGT1A1 or UGT2B7, or the transporters Pgp, BCRP, BSEP, organic anion transporting polypeptide 1B1 (OATP1B1), OATP1B3, OCT1, MATE2-K, multidrug resistance-associated protein 2 (MRP2) or MRP4. In vitro, dolutegravir did not induce CYP1A2, CYP2B6 or CYP3A4. Based on this data, dolutegravir is not expected to affect the pharmacokinetics of medicinal products that are substrates of major enzymes or transporters (see Interactions).
In vitro, dolutegravir was not a substrate of human OATP 1B1, OATP 1B3 or OCT 1.
In vitro, abacavir did not inhibit or induce CYP enzymes (other than CY1A1 and CYP3A4 [limited potential], see Interactions) and demonstrates no or weak inhibition of OATP1B1, OAT1B3, OCT1, OCT2, BCRP and P-gp or MATE2-K. Abacavir is therefore not expected to affect the plasma concentrations of drugs that are substrates of these enzymes or transporters.
Abacavir was not significantly metabolised by CYP enzymes. In vitro, abacavir was not a substrate of OATP1B1, OATP1B3, OCT1, OCT2, OAT1, MATE1, MATE2-K, MRP2 or MRP4 therefore drugs that modulate these transporters are not expected to affect abacavir plasma concentrations.
In vitro, lamivudine did not inhibit or induce CYP enzymes (such as CYP3A4, CYP2C9 or CYP2D6) and demonstrated no or weak inhibition of OATP1B1, OAT1B3, OCT3, BCRP, P-gp, MATE1 or MATE2-K. Lamivudine is therefore not expected to affect the plasma concentrations of drugs that are substrates of these enzymes or transporters.
Lamivudine was not significantly metabolised by CYP enzymes.
Elimination: Dolutegravir has a terminal half-life of ~14 hours. The apparent oral clearance (CL/F) is approximately 1 L/hr in HIV-infected patients based on a population pharmacokinetic analysis.
The mean half-life of abacavir is about 1.5 hours. The geometric mean terminal half-life of intracellular active moiety carbovir triphosphate (TP) at steady-state is 20.6 hours. Following multiple oral doses of abacavir 300 mg twice a day there is no significant accumulation of abacavir. Elimination of abacavir is via hepatic metabolism with subsequent excretion of metabolites primarily in the urine. The metabolites and unchanged abacavir account for about 83% of the administered abacavir dose in the urine. The remainder is eliminated in the faeces.
The observed lamivudine half-life of elimination is 5 to 7 hours. For patients receiving lamivudine 300 mg once daily, the terminal intracellular half-life of lamivudine-TP was 16 to 19 hours. The mean systemic clearance of lamivudine is approximately 0.32 l/h/kg, predominantly by renal clearance (> 70%) via the organic cationic transport system. Studies in patients with renal impairment show lamivudine elimination is affected by renal dysfunction. Dose reduction is required for patients with creatinine clearance < 50 ml/min (see Dosage & Administration).
Pharmacokinetic/pharmacodynamic relationship(s): In a randomized, dose-ranging trial, HIV-1-infected subjects treated with dolutegravir monotherapy (ING111521) demonstrated rapid and dose-dependent antiviral activity with mean decline in HIV-1 RNA of 2.5 log10 at day 11 for 50 mg dose. This antiviral response was maintained for 3 to 4 days after the last dose in the 50 mg group.
Intracellular pharmacokinetics: The geometric mean terminal carbovir-TP intracellular half-life at steady-state was 20.6 hours, compared to the geometric mean abacavir plasma half-life of 2.6 hours. The terminal intracellular half-life of lamivudine-TP was prolonged to 16-19 hours, compared to the plasma lamivudine half-life of 5-7 hours, supporting once daily dosing of ABC and 3TC.
Special patient populations: Hepatic impairment: Pharmacokinetic data has been obtained for dolutegravir, abacavir and lamivudine separately.
Dolutegravir is primarily metabolized and eliminated by the liver. A single dose of 50 mg of dolutegravir was administered to 8 subjects with moderate hepatic impairment (Child-Pugh class B) and to 8 matched healthy adult controls. While the total dolutegravir concentration in plasma was similar, a 1.5 to 2-fold increase in unbound exposure to dolutegravir was observed in subjects with moderate hepatic impairment compared to healthy controls. No dosage adjustment is considered necessary for patients with mild to moderate hepatic impairment. The effect of severe hepatic impairment on the pharmacokinetics of dolutegravir has not been studied.
Abacavir is metabolised primarily by the liver. The pharmacokinetics of abacavir have been studied in patients with mild hepatic impairment (Child-Pugh score 5-6) receiving a single 600 mg dose. The results showed that there was a mean increase of 1.89-fold [1.32; 2.70] in the abacavir AUC, and 1.58 [1.22; 2.04] fold in the elimination half-life. No recommendation on dose reduction is possible in patients with mild hepatic impairment due to substantial variability of abacavir exposure.
Data obtained in patients with moderate to severe hepatic impairment show that lamivudine pharmacokinetics are not significantly affected by hepatic dysfunction.
Based on data obtained for abacavir, Triumeq is not recommended in patients with moderate and severe hepatic impairment.
Renal impairment: Pharmacokinetic data have been obtained for dolutegravir, lamivudine and abacavir separately.
Renal clearance of unchanged active substance is a minor pathway of elimination for dolutegravir. A study of the pharmacokinetics of dolutegravir was performed in subjects with severe renal impairment (CLcr <30 mL/min). No clinically important pharmacokinetic differences between subjects with severe renal impairment (CLcr <30 mL/min) and matching healthy subjects were observed. Dolutegravir has not been studied in patients on dialysis, though differences in exposure are not expected.
Abacavir is primarily metabolised by the liver with approximately 2% of abacavir excreted unchanged in the urine. The pharmacokinetics of abacavir in patients with end-stage renal disease is similar to patients with normal renal function.
Studies with lamivudine show that plasma concentrations (AUC) are increased in patients with renal dysfunction due to decreased clearance.
Based on the lamivudine data, Triumeq is not recommended for patients with creatinine clearance of < 50 ml/min.
Elderly: Population pharmacokinetic analysis of dolutegravir using data in HIV-1 infected adults showed that there was no clinically relevant effect of age on dolutegravir exposure.
Pharmacokinetic data for dolutegravir, abacavir and lamivudine in subjects >65 years of age are limited.
Paediatric population: The pharmacokinetics of dolutegravir in 10 antiretroviral treatment-experienced HIV-1 infected adolescents (12 to 17 years) showed that dolutegravir 50 mg once daily dosage resulted in dolutegravir exposure comparable to that observed in adults who received dolutegravir 50 mg once daily.
Limited data are available in adolescents receiving a daily dose of 600 mg of abacavir and 300 mg of lamivudine. Pharmacokinetic parameters are comparable to those reported in adults.
Polymorphisms in drug metabolising enzymes: There is no evidence that common polymorphisms in drug metabolising enzymes alter dolutegravir pharmacokinetics to a clinically meaningful extent. In a meta-analysis using pharmacogenomics samples collected in clinical studies in healthy subjects, subjects with UGT1A1 (n=7) genotypes conferring poor dolutegravir metabolism had a 32% lower clearance of dolutegravir and 46% higher AUC compared with subjects with genotypes associated with normal metabolism via UGT1A1 (n=41).
Gender: Population PK analyses using pooled pharmacokinetic data from Phase IIb and Phase III adult trials revealed no clinically relevant effect of gender on the exposure of dolutegravir. There is no evidence that a dose adjustment of dolutegravir, abacavir or lamivudine would be required based on the effects of gender on PK parameters.
Race: Population PK analyses using pooled pharmacokinetic data from Phase IIb and Phase III adult trials revealed no clinically relevant effect of race on the exposure of dolutegravir. The pharmacokinetics of dolutegravir following single dose oral administration to Japanese subjects appear similar to observed parameters in Western (US) subjects. There is no evidence that a dose adjustment of dolutegravir, abacavir or lamivudine would be required based on the effects of race on PK parameters.
Co-infection with Hepatitis B or C: Population pharmacokinetic analysis indicated that hepatitis C virus co-infection had no clinically relevant effect on the exposure to dolutegravir. There are limited pharmacokinetic data on subjects with hepatitis B co-infection (see Precautions).
Toxicology: Preclinical safety data: There are no data available on the effects of the combination of dolutegravir, abacavir and lamivudine in animals, except a negative in vivo rat micronucleus test which tested the effects of the combination of abacavir and lamivudine.
Mutagenicity and carcinogenicity: Dolutegravir was not mutagenic or clastogenic using in vitro tests in bacteria and cultured mammalian cells, and an in vivo rodent micronucleus assay.
Neither abacavir nor lamivudine were mutagenic in bacterial tests, but consistent with other nucleoside analogues, inhibit cellular DNA replication in in vitro mammalian tests such as the mouse lymphoma assay. The results of an in vivo rat micronucleus test with abacavir and lamivudine in combination were negative.
Lamivudine has not shown any genotoxic activity in the in vivo studies. Abacavir has a weak potential to cause chromosomal damage both in vitro and in vivo at high tested concentrations.
The carcinogenic potential of a combination of dolutegravir, abacavir and lamivudine has not been tested. Dolutegravir was not carcinogenic in long term studies in the mouse and rat. In long-term oral carcinogenicity studies in rats and mice, lamivudine did not show any carcinogenic potential.
Carcinogenicity studies with orally administered abacavir in mice and rats showed an increase in the incidence of malignant and non-malignant tumours. Malignant tumours occurred in the preputial gland of males and the clitoral gland of females of both species, and in rats in the thyroid gland of males and in the liver, urinary bladder, lymph nodes and the subcutis of females.
The majority of these tumours occurred at the highest abacavir dose of 330 mg/kg/day in mice and 600 mg/kg/day in rats. The exception was the preputial gland tumour which occurred at a dose of 110 mg/kg in mice. The systemic exposure at the no effect level in mice and rats was equivalent to 3 and 7 times the human systemic exposure during therapy. While the clinical relevance of these findings is unknown, these data suggest that a potential carcinogenic risk to humans is outweighed by the clinical benefit.
Repeat-dose toxicity: The effect of prolonged daily treatment with high doses of dolutegravir has been evaluated in repeat oral dose toxicity studies in rats (up to 26 weeks) and in monkeys (up to 38 weeks). The primary effect of dolutegravir was gastrointestinal intolerance or irritation in rats and monkeys at doses that produce systemic exposures approximately 38 and 1.5 times the 50 mg human clinical exposure based on AUC, respectively. Because gastrointestinal (GI) intolerance is considered to be due to local active substance administration, mg/kg or mg/m2 metrics are appropriate determinates of safety cover for this toxicity. GI intolerance in monkeys occurred at 30 times the human mg/kg equivalent dose (based on 50 kg human), and 11 times the human mg/m2 equivalent dose for a total daily clinical dose of 50 mg.
In toxicology studies abacavir was shown to increase liver weights in rats and monkeys. The clinical relevance of this is unknown. There is no evidence from clinical studies that abacavir is hepatotoxic. Additionally, autoinduction of abacavir metabolism or induction of the metabolism of other medicinal products hepatically metabolised has not been observed in humans.
Mild myocardial degeneration in the heart of mice and rats was observed following administration of abacavir for two years. The systemic exposures were equivalent to 7 to 21 times the expected systemic exposure in humans. The clinical relevance of this finding has not been determined.
Reproductive toxicology: In reproductive toxicity studies in animals, dolutegravir, lamivudine and abacavir were shown to cross the placenta.
Oral administration of dolutegravir to pregnant rats at doses up to 1000 mg/kg daily from days 6 to 17 of gestation did not elicit maternal toxicity, developmental toxicity or teratogenicity (50 times the 50 mg human clinical exposure when administered in combination with abacavir and lamivudine based on AUC).
Oral administration of dolutegravir to pregnant rabbits at doses up to 1000 mg/kg daily from days 6 to 18 of gestation did not elicit developmental toxicity or teratogenicity (0.74 times the 50mg human clinical exposure when administered in combination with abacavir and lamivudine based on AUC). In rabbits, maternal toxicity (decreased food consumption, scant/no faeces/urine, suppressed body weight gain) was observed at 1000 mg/kg (0.74 times the 50 mg human clinical exposure when administered in combination with abacavir and lamivudine based on AUC).
Lamivudine was not teratogenic in animal studies but there were indications of an increase in early embryonic deaths in rabbits at relatively low systemic exposures, comparable to those achieved in humans. A similar effect was not seen in rats even at very high systemic exposure.
Abacavir demonstrated toxicity to the developing embryo and foetus in rats, but not in rabbits. These findings included decreased foetal body weight, foetal oedema, and an increase in skeletal variations/malformations, early intra-uterine deaths and still births. No conclusion can be drawn with regard to the teratogenic potential of abacavir because of this embryo-foetal toxicity.
Fertility studies in rats have shown that dolutegravir, abacavir and lamivudine have no effect on male or female fertility.