Nebules: A 2.5 mg plastic ampoule containing a sterile, aqueous, colourless to pale yellow solution of salbutamol as the sulphate. The concentration, which is expressed in terms of salbutamol is 0.1% (1 mg salbutamol as the sulphate in 1 mL). Each nebule contains 2.5 mL solution equivalent to 2.5 mg salbutamol.
Accuhaler: VENTOLIN ACCUHALER is a moulded plastic device containing a foil strip with 60 regularly spaced blisters each containing 200 micrograms of salbutamol (as sulphate) and lactose (which contains milk protein).
Inhaler: VENTOLIN Inhaler is a pressurised metered-dose inhaler which delivers 100mcg of salbutamol (as sulphate) per actuation. VENTOLIN Inhaler contains the CFC-free propellant HFA 134a.
Solution for Intravenous Infusion: VENTOLIN Solution for Intravenous Infusion 5mg in 5 ml (1mg/ml) is presented as ampoules of 5 ml each containing 5mg salbutamol, as sulphate.
Excipients/Inactive Ingredients: Solution for Intravenous Infusion: Sodium chloride, Sodium hydroxide, Sulfuric acid and Water for Injections.
Nebules: Routine management of chronic bronchospasm - unresponsive to conventional therapy. Treatment of acute severe asthma (status asthmaticus).
Accuhaler: VENTOLIN ACCUHALER can be used in the management of asthma, bronchospasm and/or reversible airways obstruction.
Salbutamol provides short-acting (4-hour) bronchodilation with fast onset (within 5 minutes) in reversible airways obstruction due to asthma. With its fast onset of action, it is particularly suitable for the management and prevention of attack in mild asthma and for the treatment of acute exacerbations in moderate and severe asthma.
VENTOLIN ACCUHALER is particularly suitable for the relief of asthma symptoms. It should be used to relieve symptoms when they occur, and to prevent them in those circumstances recognised by the patient to precipitate an asthma attack (e.g. before exercise or unavoidable allergen exposure).
VENTOLIN ACCUHALER is particularly valuable as relief medication in mild, moderate or severe asthma, provided that reliance on it does not delay the introduction and use of regular inhaled corticosteroid therapy.
Inhaler: VENTOLIN Inhaler provides short-acting (4 to 6 hour) bronchodilatation with fast onset (within 5 minutes) in reversible airways obstruction.
It is particularly suitable for the relief and prevention of asthma symptoms. It should be used to relieve symptoms when they occur, and to prevent them in those circumstances recognised by the patient to precipitate an asthma attack (e.g. before exercise or unavoidable allergen exposure).
VENTOLIN Inhaler is particularly valuable as a relief medication in mild, moderate or severe asthma, provided that reliance on it does not delay the introduction and use of regular inhaled corticosteroid therapy.
Solution for Intravenous Infusion: Salbutamol is a beta-adrenergic stimulant that has a selective action on the beta-2 adrenoceptors in the bronchi and uterus and much less action on the beta-1 adrenoceptors in the heart. VENTOLIN parenteral preparations are indicated for two distinct clinical situations: For the relief of severe bronchospasm associated with asthma or bronchitis and for the treatment of status asthmaticus.
For the short term management of uncomplicated premature labour; to arrest labour between 22 and 37 weeks of gestation in patients with no medical or obstetric contraindication to tocolytic therapy.
Increasing use of beta-2 agonist may be a sign of worsening asthma. Under these conditions a reassessment of the patient's therapy plan may be required and concomitant glucocorticosteroid therapy should be considered.
As there may be adverse effects associated with excessive dosing, the dosage or frequency of administration should only be increased on medical advice.
Nebules: VENTOLIN Nebules are to be used with a nebuliser, under the direction of a physician.
The solution must not be injected, or swallowed.
Clinical efficacy of nebulised salbutamol in infants under 18 months is uncertain. As transient hypoxaemia may occur, supplement oxygen therapy should be considered.
Adults and Children: A suitable starting dose of salbutamol by wet inhalation is 2.5 mg. This may be increased to 5 mg. Treatment may be repeated four times daily. In adults higher dosing, up to 40 mg per day, can be given under strict medical supervision in hospital for the treatment of severe airway obstruction.
Salbutamol has a duration of 4-6 hours in most patients.
VENTOLIN Nebules are intended to be used undiluted. However, if prolonged delivery time is desirable (more than 10 minutes) dilution using sterile normal saline as a diluent may be required.
Accuhaler: VENTOLIN ACCUHALER is for inhalation use only. VENTOLIN ACCUHALER is suitable for many patients including those who cannot use a metered-dose inhaler successfully.
Adults (including the elderly): For the relief of acute bronchospasm, 200mcg as a single dose. The maximum daily dose is 200mcg four times a day.
To prevent allergen- or exercise-induced asthma, 200mcg should be taken 10-15 minutes before challenge.
Children: The recommended dose for relief of acute bronchospasm or before allergen exposure or exercise is 200mcg. The maximum daily dose is 200mcg four times daily.
On demand use of VENTOLIN ACCUHALER should not exceed four times daily. Reliance on such frequent supplementary use, or a sudden increase in dose, indicates poorly controlled or deteriorating asthma (see Precautions).
Inhaler: VENTOLIN inhaler is for oral inhalation use only. A spacer device may be used in patients who find it difficult to synchronise aerosol actuation with inspiration of breath.
Adults (including the elderly): For the relief of acute asthma symptoms including bronchospasm, one inhalation (100mcg) may be administered as a single minimum starting dose. This may be increased to two inhalations if necessary. To prevent allergen- or exercise-induced symptoms, two inhalations should be taken 10-15 minutes before challenge.
For chronic therapy, two inhalations up to four times a day.
Children: For the relief of acute asthma symptoms including bronchospasm, or before allergen exposure or exercise, one inhalation, or two if necessary.
For chronic therapy, two inhalations up to four times a day.
Babies and young children may benefit from use of a spacer device.
On-demand use of VENTOLIN Inhaler should not exceed 8 inhalations in any 24 hours.
Solution for Intravenous Infusion: VENTOLIN parenteral preparations are to be used under the direction of a physician.
In severe bronchospasm and status asthmaticus: Adults: A suitable solution for infusion providing 10 mcg salbutamol / ml is prepared by diluting 5ml of VENTOLIN Solution for Intravenous Infusion to 500ml with an infusion solution such as sodium chloride and dextrose injection BP. Other suitable diluents are Water for Injections BP, Sodium Chloride Injection BP or Dextrose Injection BP.
Infusion rates providing 3 to 20 mcg salbutamol / min (0.3 to 2 ml/min of the previously mentioned infusion solution) are usually adequate. Higher doses have been used with success in patients with respiratory failure.
Paediatric Population: The safety and efficacy of VENTOLIN Solution for Intravenous Infusion in children under the age of 12 has not been established. From the available data no recommendation on posology can be made.
Children aged 12 years and over: Dose as per adult population.
In the short term management of uncomplicated premature labour: Treatment with VENTOLIN Solution for Intravenous Infusion should only be initiated by obstetricians/ physicians experienced in the use of tocolytic agents. It should be carried out in facilities adequately equipped to perform continuous monitoring of maternal and foetus health status.
Duration of treatment should not exceed 48 hours as data show that the main effect of tocolytic therapy is a delay in delivery of up to 48 hours; no statistically significant effect on perinatal mortality or morbidity has been observed in randomized, controlled trials. This short term delay may be used to implement other measures known to improve perinatal health.
VENTOLIN Solution for Intravenous Infusion should be administered as early as possible after the diagnosis of premature labour, and after evaluation of the patient to eliminate any contra-indications to the use of salbutamol (see Contraindications). This should include an adequate assessment of the patient's cardiovascular status with supervision of cardiorespiratory function and ECG monitoring throughout treatment (see Precautions).
Special caution for infusion: The dose must be individually titrated with reference to suppression of contractions, increase in pulse rate and changes in blood pressure, which are limiting factors. These parameters should be carefully monitored during treatment. A maximum maternal heart rate of 120 beats per min should not be exceeded.
Careful control of the level of hydration is essential to avoid the risk of maternal pulmonary oedema (see Precautions). The volume of fluid in which the drug is administered should thus be kept to a minimum. A controlled infusion device should be used, preferably a syringe pump.
Infusion rates providing 10-45 mcg salbutamol / min are generally adequate to control uterine contractions. A starting rate of 10 mcg / min is recommended, increasing the rate at 10-minute intervals until there is evidence of patient response shown by diminution in strength, frequency or duration of contractions. Thereafter, the infusion rate may be increased slowly until contractions cease. Careful attention should be given to cardio-respiratory function and fluid balance monitored. Once uterine contractions have ceased the infusion rate should be maintained at the same level for one hour and then reduced by 50% decrements at six-hourly intervals. If labour progresses despite treatment the infusion should be stopped.
Dilution: The recommended diluent is 5% Dextrose (see Contraindications).
For use in a syringe pump: Prepare a solution providing 200 mcg salbutamol / ml by diluting 10 ml VENTOLIN Solution for Intravenous Infusion with 40 ml diluents. An infusion rate of 10 to 45 mcg / min is equivalent to 0.05 to 0.225 ml / min of this solution.
Other infusion methods: Prepare a solution providing 20 mcg salbutamol / min by diluting 10 ml VENTOLIN Solution for Intravenous Infusion with 490 ml diluents. An infusion rate of 10 to 45 mcg / min is equivalent to 0.5 to 2.25 ml / min of this solution.
The most common signs and symptoms of overdose with VENTOLIN are transient beta agonist pharmacologically mediated events, including tachycardia, tremor, hyperactivity and metabolic effects including hypokalaemia and lactic acidosis (see Precautions and Adverse Reactions).
Hypokalaemia may occur following overdose with VENTOLIN. Serum potassium levels should be monitored.
Lactic acidosis has been reported in association with high therapeutic doses as well as overdoses of short-acting beta-agonist therapy, therefore monitoring for elevated serum lactate and consequent metabolic acidosis (particularly if there is persistence or worsening of tachypnea despite resolution of other signs of bronchospasm such as wheezing) may be indicated in the setting of overdose.
Solution for Intravenous Infusion: Nausea, vomiting and hyperglycaemia have been reported, predominantly in children and when salbutamol overdose has been taken via the oral route.
Further management should be as clinically indicated.
VENTOLIN is contraindicated in patients with a history of hypersensitivity to any of its components.
Non-IV formulations of salbutamol must not be used to arrest uncomplicated premature labour or threatened abortion.
Accuhaler: VENTOLIN ACCUHALER is contraindicated in patients with severe milk-protein allergy.
Solution for Intravenous Infusion: VENTOLIN Solution for Intravenous Infusion is contraindicated in the following conditions: Any condition at a gestational age <22 weeks; As a tocolytic agent in patients with pre-existing ischaemic heart disease or those patients with significant
risk factors for ischaemic heart disease; Threatened abortion during the 1st and 2nd trimester; Any condition of the mother or foetus in which prolongation of the pregnancy is hazardous, e.g. severe toxaemia, intrauterine infection, vaginal bleeding resulting from placenta praevia, eclampsia or severe preeclampsia, placental abruption or cord compression; Intrauterine foetal death, known lethal congenital or lethal chromosomal malformation.
VENTOLIN Solution for Intravenous Infusion is also contraindicated in any pre-existing medical conditions with which a betamimetic would have an untoward effect e.g. pulmonary hypertension and cardiac disorders such as hypertrophic obstructive cardiomyopathy or any type of obstruction of the left ventricular outflow tract, e.g. aortic stenosis.
The management of asthma should normally follow a stepwise programme, and the patient response should be monitored clinically and by lung function tests.
Increasing use of short-acting bronchodilators, in particular beta-2 agonists to relieve symptoms indicates deterioration of asthma control. Under these conditions, the patient's therapy plan should be re-assessed.
Sudden and progressive deterioration in asthma control is potentially life-threatening and consideration should be given to starting or increasing corticosteroid therapy. In patients considered at risk, daily peak flow monitoring may be instituted.
VENTOLIN should be administered cautiously to patients with thyrotoxicosis.
Potentially serious hypokalaemia may result from beta-2 agonist therapy mainly from parenteral and nebulised administration.
Particular caution is advised in acute severe asthma as this effect may be potentiated by concomitant treatment with xanthine derivatives, steroids, diuretics and by hypoxia. It is recommended that serum potassium levels should be monitored in such situations.
As with other inhalation therapy, paradoxical bronchospasms may occur, resulting in an immediate increase in wheezing after dosing. This should be treated immediately with an alternative presentation or a different fast-acting inhaled bronchodilator, if immediately available. VENTOLIN should be discontinued immediately, and if necessary a different fast-acting bronchodilator instituted for ongoing use.
Nebules: VENTOLIN Nebules must only be used by inhalation, to be breathed in through the mouth, and must not be injected or swallowed.
Patients receiving treatment at home with VENTOLIN Nebules must be warned that if either the usual relief is diminished or the usual duration of action reduced, they should not increase the dose or its frequency of administration, but should seek medical advice.
VENTOLIN Nebules should be used with caution in patients known to have received large doses of other sympathomimetic drugs.
A small number of cases of acute angle closure glaucoma have been reported in patients treated with a combination of nebulised salbutamol and ipratropium bromide. A combination of nebulised salbutamol with nebulised anticholinergics should therefore be used cautiously. Patients should receive adequate instruction in correct administration and be warned not to let the solution or mist enter the eye.
Effects on the Ability to Drive and Operate Machinery: None reported.
Accuhaler: The dosage or frequency of administration should only be increased on medical advice. In the event of a previously effective dose of inhaled VENTOLIN failing to give relief for at least three hours, the patient should be advised to seek medical advice in order that any necessary additional steps may be taken.
Inhaler: The dosage or frequency of administration should only be increased on medical advice. If a previously effective dose of inhaled salbutamol fails to give relief for at least three hours, the patient should be advised to seek medical advice.
Nebules/Solution for Intravenous Infusion: In common with other beta-adrenoceptor agonists, VENTOLIN can induce reversible metabolic changes such as reversible hypokalaemia and increased blood glucose levels.
The diabetic patient may be unable to compensate for this and the development of ketoacidosis has been reported. Concurrent administration of corticosteroids can exaggerate this effect.
Diabetic patients and those concurrently receiving corticosteroids should be monitored frequently during intravenous infusion of VENTOLIN so that remedial steps (e.g. an increase in insulin dosage) can be taken to counter any metabolic change occurring. For these patients, VENTOLIN Solution for Intravenous Infusion should be diluted with Sodium Chloride Injection BP, rather than Sodium Chloride and Dextrose Injection BP.
Lactic acidosis has been reported very rarely in association with high therapeutic doses of intravenous and nebulised short-acting beta-agonist therapy, mainly in patients being treated for an asthma exacerbation (see Adverse Reactions). Increase in lactate levels may lead to dyspnoea and compensatory hyperventilation, which could be misinterpreted as sign of asthma treatment failure and lead to inappropriate intensification of short-acting beta-agonist treatment. It is therefore recommended that patients are monitored for the development of elevated serum lactate and consequent metabolic acidosis in this setting.
Solution for Intravenous Infusion: The use of salbutamol parenteral preparations in the treatment of severe bronchospasm or status asthmaticus does not obviate the requirement for glucocorticoid steroid therapy as appropriate.
When practicable, administration of oxygen concurrently with parenteral salbutamol is recommended, particularly when it is given by intravenous infusion to hypoxic patients.
Tocolysis: Any decision to initiate therapy with VENTOLIN Solution for Intravenous Infusion should be undertaken after careful consideration of the risks and benefits of treatment.
Treatment should only be carried out in facilities adequately equipped to perform continuous monitoring of maternal and foetal health status. Tocolysis with beta-agonists is not recommended when membranes have ruptured or the cervix dilation is beyond 4 cm.
VENTOLIN Solution for Intravenous Infusion should be used with caution in tocolysis and supervision of cardiorespiratory function and ECG monitoring, should be performed throughout treatment. The following monitoring measures must be constantly applied to the mother and, when feasible / appropriate, to the foetus: Blood pressure and heart rate; ECG; Electrolyte and fluid balance - to monitor for pulmonary oedema; Glucose and lactate levels - with particular regard to diabetic patients; Potassium levels - beta-agonists are associated with a disease in serum potassium which increases the risk of arrhythmias (see Interactions).
Treatment should be discontinued if signs of myocardial ischaemia (such as chest pain or ECG changes) develop.
VENTOLIN Solution for Intravenous Infusion should not be used as a tocolytic agent in patients with significant risk factors for, or a suspicion of any kind of pre-existing heart disease (e.g. tachyarrhythmias, heart failure or valvular heart disease; see Contraindications). In premature labour in a patient with known or suspected cardiac disease, a physician experienced in cardiology should assess the suitability of treatment before intravenous infusion with VENTOLIN Solution for Intravenous Infusion.
Pulmonary Oedema: As maternal pulmonary oedema and myocardial ischaemia have been reported during or following treatment of premature labour with beta-agonists, careful attention should be given to fluid balance and cardio-respiratory function. Patients with predisposing factors including multiple pregnancies, fluid overload, maternal infection and pre-eclampsia may have an increased risk of developing pulmonary oedema. Administration with a syringe pump as opposed to i.v. infusion will limit risk of fluid overload. If signs of pulmonary oedema or myocardial ischaemia develop, discontinuation of treatment should be considered (see Dosage & Administration and Adverse Reactions).
Blood pressure and heart rate: Increases in maternal heart rate of the order of 20-50 beats per minute usually accompany the infusion of beta-agonists. The maternal pulse rate should be monitored and the need to control such increases by dose reduction or drug withdrawal should be evaluated on a case by case basis.
Generally maternal pulse rate should not be allowed to exceed a steady rate of 120 beats per minute.
Maternal blood pressure may fall slightly during the infusion, the effect of being greater on diastolic than on systolic pressure. Falls in diastolic pressure are usually within the range of 10-20 mmHg.
The effect of infusion on foetal heart rate is less marked, but increases of up to 20 beats per minute may occur.
In order to minimize the risk of hypotension associated with tocolytic therapy, special care should be taken to avoid caval compression by keep the patient in the left or right lateral positions throughout the infusion.
Diabetes: Administration of beta agonists is associated with a rise of blood glucose. Therefore blood glucose and lactate levels should be monitored in mothers with diabetes and diabetic treatment adjusted accordingly to meet the needs of the diabetic mother during tocolysis (see Interactions).
Hyperthyroidism: VENTOLIN Solution for Intravenous Infusion should only be administered cautiously to patients suffering from thyrotoxicosis after careful evaluation of the benefits and risks of treatment.
Pregnancy: Nebules/Accuhaler/Solution for Intravenous Infusion: Administration of drugs during pregnancy should only be considered if the expected benefit to the mother is greater than any possible risk to the fetus.
During world-wide marketing experience, rare cases of various congenital anomalies, including cleft palate and limb defects have been reported in the offspring of patients being treated with VENTOLIN. Some of the mothers were taking multiple medications during their pregnancies.
Because no consistent pattern of defects can be discerned, and baseline rate for congenital anomalies is 2 to 3%, a relationship with salbutamol use cannot be established.
Inhaler: Studies in animals have shown reproductive toxicity. Safety in pregnant women has not been established. No controlled clinical trials with salbutamol have been conducted in pregnant women.
Rare reports of various congenital anomalies following intrauterine exposure to salbutamol (including cleft palate, limb defects and cardiac disorders) have been received. Some of the mothers were taking multiple medications during their pregnancies. VENTOLIN Inhaler should not be used during pregnancy unless clearly necessary.
Lactation: Nebules/Accuhaler/Solution for Intravenous Infusion: As salbutamol is probably secreted in breast milk, its use in nursing mothers is not recommended unless the expected benefits outweigh the potential risk. It is not known whether salbutamol in breast milk has a harmful effect on the neonate.
Inhaler: As salbutamol is probably secreted in breast milk, its use in nursing mothers requires careful consideration. It is not known whether salbutamol has a harmful effect on the neonate, and so its use should be restricted to situations where it is felt that the expected benefit to the mother is likely to outweigh any potential risk to the neonate.
Fertility: There is no information on the effects of salbutamol on human fertility. There were no adverse effects on fertility in animals.
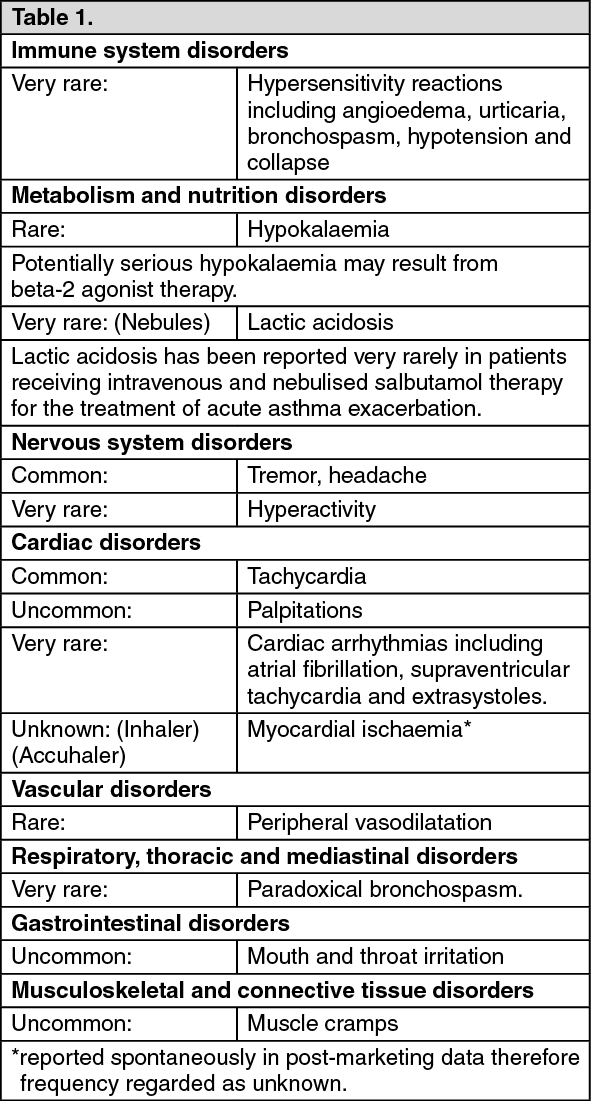
Adverse events are listed as follows by system organ class and frequency. Frequencies are defined as: very common (≥1/10), common (≥1/100 to <1/10), uncommon (≥1/1000 to <1/100), rare (≥1/10,000 to <1/1000) and very rare (<1/10,000) including isolated reports. Very common and common events were generally determined from clinical trial data. Rare and very rare events were generally determined from spontaneous data.
Nebules/Accuhaler/Inhaler: See Table 1.
 Click on icon to see table/diagram/image
Solution for Intravenous Infusion:
Click on icon to see table/diagram/image
Solution for Intravenous Infusion: The most common undesirable effects of VENTOLIN Solution for Intravenous Infusion are correlated with the betamimetic pharmacological activity and may be limited or avoided by a close monitoring of hemodynamic parameters, such as blood pressure and heart rate, and an appropriate adjustment of the dose. They normally recede upon therapy discontinuation. (See Table 2.)
Click on icon to see table/diagram/image
VENTOLIN and non-selective beta-blocking drugs, such as propranolol, should not usually be prescribed together.
VENTOLIN is not contraindicated in patients under treatment with monoamine oxidase inhibitors (MAOIs).
Solution for Intravenous Infusion: Halogenated anaesthetics: Owing to the additional antihypertensive effect, there is increased uterine inertia with risk of haemorrhage; in addition, serious ventricular rhythm disorders due to increased cardiac reactivity, have been reported on interaction with halogenated anaesthetics. Treatment should be discontinued, whenever possible, at least 6 hours before any scheduled anaesthesia with halogenated anaesthetics.
Corticosteroids: Systemic corticosteroids are frequently given during premature labour to enhance foetal lung development. There have been reports of pulmonary oedema in women concomitantly administered with beta-agonists and corticosteroids.
Corticosteroids are known to increase blood glucose and can deplete serum potassium, therefore concomitant administration should be undertaken with caution with continuous patient monitoring owing to the increased risk of hyperglycaemia and hypokalaemia (see Precautions).
Anti-diabetics: The administration of beta-agonists is associated with a rise of blood glucose, which can be interpreted as an attenuation of anti-diabetic therapy; therefore individual anti-diabetic therapy may need to be adjusted (see Precautions).
Potassium depleting agents: Owing to the hypokalaemic effect of beta-agonists, concurrent administration of serum potassium depleting agents known to exacerbate the risk of hypokalaemia, such as diuretics, digoxin, methyl xanthines and corticosteroids, should be administered cautiously after careful evaluation of the benefits and risks with special regard to the increased risk of cardiac arrhythmias arising as a result of hypokalaemia (see Precautions).
Nebules: Dilution: VENTOLIN Nebules may be diluted with sterile normal saline. Any unused solution in the chamber of the nebuliser must be discarded.
Accuhaler: Instructions for Use/Handling: The Accuhaler is sealed in a foil overwrap. The overwrap provides moisture protection and should only be opened when ready to use it for the first time. Once removed/opened the foil overwrap should be discarded.
About the ACCUHALER: When taking ACCUHALER out of its box, it will be in the closed position.
The ACCUHALER contains 60 individually protected doses of the medicine, in powder form.
The dose indicator tells how many doses are left.
Each dose is accurately measured and hygienically protected. It requires no maintenance - and no refilling.
The dose indicator on top of the ACCUHALER tells how many doses are left. Numbers 5 to 0 will appear in RED, to warn when there are only a few doses left.
The ACCUHALER is easy to use. When needing a dose, just follow the four simple steps: 1. Open. 2. Slide. 3. Inhale. 4. Close.
How the ACCUHALER works: Sliding the lever of the ACCUHALER opens a small hole in the mouthpiece and unwraps a dose, ready for inhalation. When closing the ACCUHALER, the lever automatically moves back to its original position, ready for the next dose when needed. The outer case protects the ACCUHALER when it is not in use.
How to use the ACCUHALER: 1. Open: To open the ACCUHALER, hold the outer case in one hand and put the thumb of the other hand on the thumbgrip. The patient should push his/her thumb away from him/her as far as it will go.
2. Slide: The patient should hold the ACCUHALER with the mouthpiece towards him/her.
The patient should slide the lever away from him/her, as far as it will go - until it clicks.
The ACCUHALER is now ready to use.
Every time the lever is pushed back, a dose is made available for inhaling.
This is shown by the dose counter.
Do not play with the lever as this releases doses which will be wasted.
3. Inhale: Before the patient starts to inhale the dose, he/she should read through this section carefully.
Hold the ACCUHALER away from the mouth. Breathe out as far as is comfortable.
Remember - never breathe into the ACCUHALER.
Put the mouthpiece to the lips. Breathe in steadily and deeply - through the ACCUHALER, not through the nose.
Remove the ACCUHALER from the mouth.
Hold the breath for about 10 seconds, or for as long as is comfortable.
Breathe out slowly.
4. Close: To close the ACCUHALER, the patient should put the thumb in the thumbgrip, and slide the thumbgrip back towards him/her, as far as it will go.
When the patient closes the ACCUHALER, it clicks shut.
The lever automatically returns to the original position and is reset.
The ACCUHALER is now ready for use again.
If the patient has been instructed to take two inhalations he/she must close the ACCUHALER and repeat stages 1 to 4.
Remember: Keep the ACCUHALER dry.
Keep it closed when not in use.
Never breathe into the ACCUHALER.
Only slide the lever when ready to take a dose.
VENTOLIN ACCUHALER must only be breathed in through the mouth.
Do not exceed the stated dose.
Inhaler: Testing the inhaler: 1. When using the inhaler for the first time, test that it is working. Remove the mouthpiece cover by gently squeezing the sides with the thumb and forefinger and pull apart.
2. To make sure that it works, shake it well, point the mouthpiece away from the patient and press the canister to release two puffs into the air. If the patient has not used the inhaler for 5 days or more, shake it well and release two puffs of medicine into the air.
Using the inhaler: It is important to start to breathe as slowly as possible just before using the inhaler.
1. Stand or sit upright when using the inhaler.
2. Remove the mouthpiece cover. Check inside and outside to make sure that the mouthpiece is clean and free of objects.
3. Shake the inhaler 4 or 5 times to ensure that any loose objects are removed and that the contents of the inhaler are evenly mixed.
4. Hold the inhaler upright with the thumb on the base, below the mouthpiece. Breathe out as far as is comfortable. Do not breathe in again yet.
5. Place the mouthpiece in the mouth between the teeth. Close the lips around it. Do not bite.
6. Breathe in through the mouth. Just after starting to breathe in, press down on the top of the canister to release a puff of medicine. Do this while still breathing in steadily and deeply.
7. Hold the breath, take the inhaler from the mouth and finger from the top of the inhaler. Continue holding the breath for a few seconds, or as long as is comfortable.
8. If the doctor has told the patient to take two puffs, wait about half a minute before taking another puff by repeating steps 3 to 7.
9. After use always replace the mouthpiece cover straight away to keep out dust. Replace the cover by firmly pushing and clicking into position.
Young children may need help and their parents may need to operate the inhaler for them. Encourage the child to breathe out and operate the inhaler just after the child starts to breathe in. Practise the technique together.
Older children or people with weak hands may find it easier to hold the inhaler with both hands. Put the two forefingers on top of the inhaler and both thumbs on the bottom below the mouthpiece. If this does not help, the doctor, nurse or pharmacist will be able to advise the patient.
Cleaning the inhaler: To stop the inhaler blocking, it is important to clean it at least once a week.
To clean the inhaler: 1. Remove the metal canister from the plastic casing of the inhaler and remove the mouthpiece cover.
2. Rinse the plastic casing thoroughly under warm running water.
3. Dry the plastic casing THOROUGHLY inside and out.
4. Replace the metal canister into the plastic casing and put on mouthpiece cover.
DO NOT PUT THE METAL CANISTER INTO WATER.
Solution for Intravenous Infusion: Dilution: VENTOLIN parenteral preparations may be diluted with Water for Injections BP, Sodium Chloride Injection BP, Sodium Chloride and Dextrose Injection BP or Dextrose Injection BP. These are the only recommended diluents.
VENTOLIN parenteral preparations should not be administered in the same syringe or infusion as any other medication.
The contents of the ampoule of VENTOLIN Solution for Intravenous Infusion must not be injected in the undiluted form; the concentration should be reduced at least by 50% before administration.
Nebules: Protect from light.
Accuhaler: Protect from frost and light. Store in a dry place.
The Accuhaler should be discarded 6 months after removal from the foil overwrap pack.
Inhaler: Replace the mouthpiece cover firmly and snap it into position. Protect from frost and direct sunlight.
As with most inhaled medications in aerosol canisters, the therapeutic effect of this medication may decrease when the canister is cold.
Do not store above 25°C.
This canister contains a pressurised liquid. Do not expose to temperatures higher than 50°C. The canister should not be broken, punctured or burnt, even when apparently empty.
Solution for Intravenous Infusion: All unused admixtures of VENTOLIN Parenteral Preparations with infusion fluids should be discarded twenty-four hours after preparation.
R03AC02 - salbutamol ; Belongs to the class of adrenergic inhalants, selective beta-2-adrenoreceptor agonists. Used in the treatment of obstructive airway diseases.
R03CC02 - salbutamol ; Belongs to the class of adrenergics for systemic use, selective beta-2-adrenoreceptor agonists. Used in the treatment of obstructive airway diseases.
Inhaler: P1; Accuhaler, Soln for IV infusion (amp), Nebules: P1S1S3
Ventolin accuhaler 200 mcg/actuation
60 actuation x 1's
Ventolin infusion 5 mg/5 mL
10 × 1's
Ventolin inhaler 100 mcg/actuation
(CFC-free) 200 actuation x 1's
Ventolin nebules 2.5 mg/2.5 mL
20 × 1's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image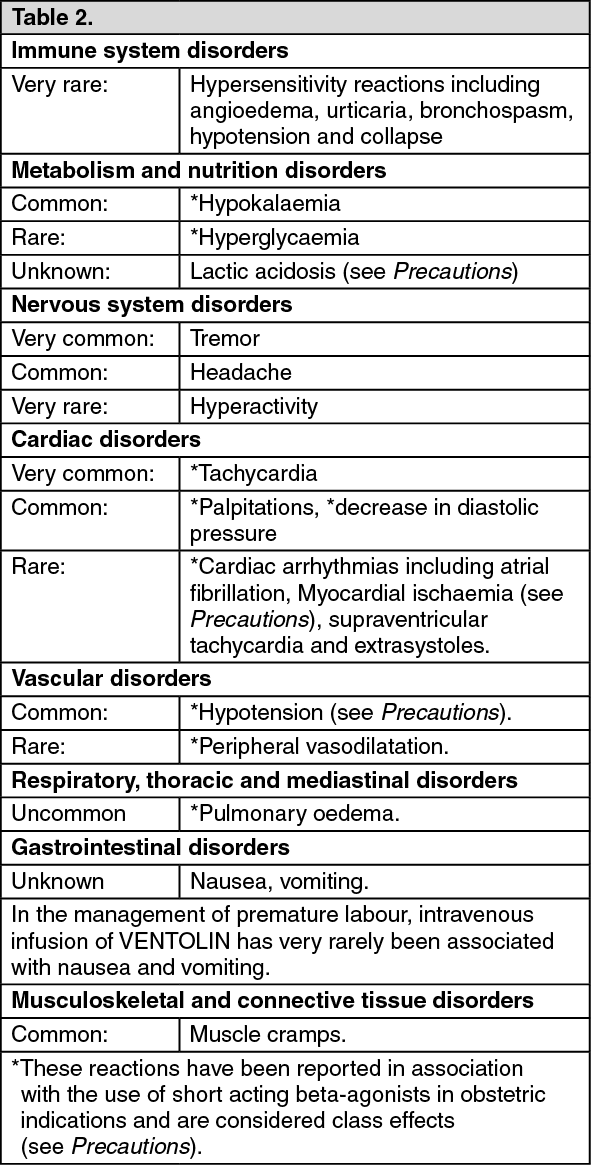 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
